New brain biometrics could help determine whether an athlete is ready to return to play after a concussion, according to new research from the University of South Australia.
Conducted in collaboration with the University of California San Francisco (UCFC), researchers found that changes in brain micro-movements – called ‘head pulses’ – could detect the lasting effects of a concussion.
Using a custom-designed headset* to evaluate head pulse biometry among 101 amateur male and female Australian Rules Football players in South Australia, researchers identified brain abnormalities in 81% of concussed players, indicating persistent injury that lasts longer than the expected recovery times.
These head pulse changes lasted 14 days after concussion symptoms and were exacerbated by return to play or unsupervised physical activity.
UniSA professor of kinesiology Kevin Norton says headpulse measures could complement current return-to-play protocols.
“Traumatic brain injuries affect more than 60 million people every year, a third of which are sports-related,” says Prof. Norton.
“While we know that the Australian sporting sector takes concussion seriously – through informed return-to-play protocols – we also know that objective measures of concussion recovery have not been fully established.
“In this study, we used head pulses – a normal measure of brain ‘wobble’, matched to each heartbeat – to assess any changes in frequency due to concussion.
“We found that almost all players who suffered a concussion had a ‘disconnect’ between their symptoms and the head pulse, so that even when the players said they felt fine, the head pulse still showed signs of brain injury.”
While most players felt like they had recovered 10 to 14 days after their injury, the study showed that some players took as long as four weeks to recover and return to normal head pulse patterns.
Concussion recovery protocols in Australian Football require 24 to 48 hours of strict physical and cognitive rest, followed by graded individual training and then team training, provided there is no worsening of symptoms; the earliest permitted return to play upon completion of protocol and medical clearance is 12 days post-concussion.
The Australian Senate Committee Report Concussion and repetitive head trauma in contact sports Published this month, it recommends that national sporting associations should explore further rule changes for sport to prevent and reduce the impact of concussions and repetitive head trauma.
This research adds to the growing body of knowledge underlying concussion protocols.
Comments
*The headset is patented by UCSF and licensed by medical technology company MindRhythm.
Data on sports-related concussions and repetitive head trauma are under-reported in Australia, but the latest AIHW data shows that 2305 sports-related concussions occurred between 2019 and 2020. Men suffered 70% of concussions and over a third of people hospitalized were young athletes aged 15 to 24.
About 730 of the concussions occurred while playing some form of football; and approximately 440 occurred while cycling
Balance training under fatigue: a randomized controlled trial of the effect of fatigue on adaptations to balance training.
Keller M, Lichtenstein E, Roth R, Faude O. J Strength Cond Res. August 29, 2023. doi: 10.1519/JSC.0000000000004620. E-publishing prior to printing. PMID: 37643391.
Full text freely available
Take home message
Balance training in a non-fatigued state produces better balance performance than training in a fatigued state. When combining balance training with other more specific training regiments, balance training should be performed before any activity that may cause fatigue.
Background
Balance training can help prevent ankle injuries. Many injury prevention programs are completed tirelessly. However, fatigue has a negative impact on the risk of lower extremity injury. To optimize our balance training, we need to know whether to ask athletes to perform the training in a fatigued or untiring state.
Study aim
The researchers completed a randomized controlled trial to assess the neuromuscular performance benefits of balance training, regardless of whether they were fatigued or not.
Methods
Initially, 52 participants completed a pre-test, including a balance assessment on 3 surfaces (wobble board, soft mat and solid ground), jump height and shuttle run test before and after high-intensity interval training (HIIT) to induce fatigue. The researchers randomly assigned participants to 1 of 3 groups: 1) balance training alone, 2) balance training while fatigued (after HIIT), and 3) balance training before fatigue (before HIIT). Participants completed 12 sessions over 6 weeks, with a minimum of 48 hours between sessions. All participants completed identical balance training interventions. Participants then completed assessments 2 to 5 days after the final training session, including a balance assessment, jump height and shuttle run test.
Results
In all six balance assessment conditions (three surfaces, fatigued or not), the group that performed balance training while fatigued experienced smaller benefits than the groups that performed balance training only or balance training before fatigue. In terms of performance, both groups that performed HIIT had greater jump height and shuttle run improvements than the group that only did balance training. Four of the five people lost to follow-up participated in the balance training while fatigued.
Viewpoints
Overall, the results of the study showed that fatigue has a negative impact on balance training. Therefore, athletes should perform balance training in a non-fatigued state (for example, at the beginning of a training session). The results also show that balance training can be combined with performance training for additional benefits. However, athletes should complete performance training after balance training to maximize the benefits of each. Ultimately, almost 1 in 4 people who performed the balance training while fatigued quit the program. This finding may indicate that athletes do not enjoy doing balance training in a fatigued state, which could lead to compliance issues in the real world.
Clinical implications
Clinicians should ask athletes to perform balance training at the beginning of a training session (before fatigue sets in).
Questions for discussion
How and when do you implement balance training in your clinical practice? What changes might you make based on the evidence presented in this study?
Written by Kyle Harris Reviewed by Jeffrey Driban
related posts
Balancing ankle injuries and football with… Balance Save the ankles with bracing or balance training: both are better than nothing Shake It Up: vibration training improves balance in chronic ankle instability A simple balance test can identify the risk of non-contact lower limb injury Balance assessments cannot predict ACL injury in elite female athletes
We know that after a lower extremity injury, such as an ACL tear, joint-related symptoms often occur, such as swelling, loss of motion and instability. But as we learn more about these injuries, there also appear to be several neuromuscular consequences.
In this episode, I talk to Terry Grindstaff of Creighton University about his research into these neuromuscular sequelae after an ACL injury, and how this could impact our initial rehabilitation, return to sport progressions, and even long-term outcomes years later.
Show notes
Terry Grindstaff is a physical therapist and athletic trainer with more than 20 years of clinical experience. He has a PhD in Kinesiology and is a professor in the Department of Physical Therapy at Creighton University. His research examines the neuromuscular consequences of lower extremity joint injuries and rehabilitation management to improve function. He provides clinical services in the athletic training room at Creighton University and is a member of the volunteer medical pool for USA Wrestling.
Social tools for COS: –Twitter: @grindstafftl – Instagram: @grindstafftl
Whether you are an athlete looking to improve performance or recovering from an injury or surgery, Blood Flow Restriction Therapy (BFR) can be a game-changer for your life. BFR has been one of the major breakthroughs in the physical therapy industry, allowing physical therapists to alleviate atrophy and muscle weakness and achieve strength gains while minimizing joint stress. With BFR, physiotherapists can improve patient outcomes and unlock new possibilities.
What is blood flow restriction therapy (BFR)?
Blood flow restriction therapy, also called occlusion training, uses a device such as a cuff or wrap and places it around an arm or leg to stop partial blood flow to the affected area. Blood flow is restricted by restricting arterial flow and venous return. Restricting blood flow creates higher levels of metabolic stress. Metabolic stress and mechanical strain are associated with increased muscle growth. Exercises can be performed with low-load resistance training and achieve the same (if not better results) as traditional strength training.
Benefits of blood flow restriction therapy
1. Increases muscle growth and strength
One of the biggest challenges after an injury or surgery is regaining muscle mass and strength. Women have a greater challenge than men in recovering muscle function after injury or surgery. Healthy men naturally have high levels of muscle-building testosterone and growth hormone to restore muscle mass, while women have less of both. After surgery, losing muscle size lasts about three days without use. The muscle shuts down due to the stress of a surgical process or injury. Myostatin, the hormone that muscle cells produce, inhibits muscle rebuilding and promotes scar tissue to limit growth.
2. Speeds up recovery
Occlusion training allows patients to achieve their goals in fewer sessions because it can produce similar results to traditional high-load training with lighter weights.
3. Restores muscle function
Rehabilitation with BFR can help minimize muscle and strength loss during immobilization or injury. In addition, it can aid in postoperative recovery and the recovery of muscle function.
4. Improves cardiovascular health
Blood flow restriction training can affect your cardiovascular system similar to traditional aerobic exercise. It can potentially improve important measures of cardiovascular health, such as VO2 max (a measure of aerobic fitness) and endothelial function (the health of your blood vessels).
Common conditions BFR Physiotherapy treats
Osteoarthritis (OA): According to studies in the Strength and Conditioning Journal, BFR may help improve OA muscle function and aid in pain management, leading to better overall function and quality of life. Overall, BFR can improve joint health.
Sports injuries: BFR treats muscle strains, ligament sprains or tendonitis
Chronic conditions: BFR treats common cardiovascular diseases such as COPD and high blood pressure, which affect more than millions of people.
Muscle weakness: BFR addresses atrophy due to various causes, such as disuse, immobilization or neurological disorders.
Edema (inflammation and swelling): BFR stimulates fluid mobilization and improves circulation in the affected area. This may especially benefit patients with acute or chronic swelling conditions, such as postoperative or post-traumatic cases.
BFR assessment in physiotherapy
Patients are assessed for the appropriate level of bladder flow restriction. Physiotherapists can use a specialized Doppler, which determines when complete occlusion of blood flow has been achieved. Additionally, a personalized treatment plan and exercise program are designed to ensure the most effective results.
Is blood flow restriction therapy safe?
Many patients are initially concerned about the safety of BFR. Blow Flow Restriction Therapy is safe for post-surgical patients, athletes, seniors and anyone who wants to accelerate effective strengthening results. Therefore, we recommend the use of blood flow restrictions under the guidance of a physiotherapist, as the exact occlusion pressure will be assessed in each patient.
Risks and side effects
At Foothills we are often asked, “Does BFR cause blood clots?” BFR should not impede overall circulation or increase the risk of blood clots. Many case studies have concluded that BFR can release anticoagulant hormones when the cuff is released.
Blood flow restriction therapy is not recommended for patients with uncontrolled high blood pressure. However, if you have uncontrolled high blood pressure or a cardiovascular condition, it is critical to consult a physical therapist or your doctor before considering BFR training. Additionally, they can assess your specific medical situation, evaluate potential risks, and provide personalized advice on whether BFR is right for you.
It is always important to prioritize your health and consult a physiotherapist who specializes in BFR for personalized guidance. If you’re curious if BFR is right for you, schedule a FREE assessment near a Foothills location! We’ve enjoyed helping people from all walks of life return to the sports and activities they love. We look forward to introducing you to the BFR training world and witnessing its incredible impact on your fitness and rehabilitation goals.
Osteoarthritis (OA) is the most common form of arthritis and is one of the top 10 conditions that contribute to the number of years lived with a disability – a measure that reflects the impact a disease has on quality of life before it disappears or leads to death. To date, no treatments have been approved that slow the progression of the disease. The development of treatments has been frustrating in part because animal models of disease caused by joint trauma poorly reflect the human disease, which usually occurs over many years and without prior trauma.
Researchers from Boston University Chobanian & Avedisian School of Medicine now propose to study individuals after they suffer knee trauma, such as anterior cruciate ligament (ACL) tears.
“Given the repeated, expensive, and discouraging past failures in developing effective treatments for osteoarthritis, a new approach is needed that focuses research for effective treatments on people with early disease,” said corresponding author David T. Felson , MD, MPH, professor of medicine and epidemiology at the School of Medicine and Boston University School of Public Health.
While most patients recover after sustaining a serious joint injury, such as an ACL tear, some experience persistent pain and develop osteoarthritis. Felson suggests that sufficient numbers of such patients exist and can be identified in advance to form a risk group in which treatments to prevent disease can be tested.
Current treatment options that reduce joint pain, such as nonsteroidal anti-inflammatory drugs (NSAIDs), are successful in some patients, but their use is limited by their toxicity. Exercise or weight loss are effective, but long-term compliance is poor. The number of total knee replacement surgeries is rising rapidly, indicating that nonsurgical treatments have not successfully alleviated patients’ pain and disability.
Researchers from BU and Cleveland Clinic reviewed data from the MOON (Multicenter Orthopedic Outcomes Network) cohort, a group of 2,340 individuals who underwent ACL reconstruction (ACLR) after traumatic tears. The MOON researchers reported that 26% of ACL reconstruction patients who responded had at least moderate knee pain with daily activities, especially climbing stairs and walking. They also found that 16.6% had a KOOS (Knee Injury and Osteoarthritis Outcome Score) pain score of less than 80 (scale 0-100 with 100 being no pain), indicating that mild to moderate pain is not rare after ACLR.
By using the MOON risk factors – which include pain and structural changes in all joint tissues, especially cartilage loss – to select individuals at high risk for subsequent pain, they were able to create a cohort at high risk for substantial post-ACLR pain . “This approach offers the potential to prevent disease and is especially valuable in targeting young adults who, following a knee injury, may have significant joint pain and disability for years before they are considered for joint replacement,” he adds.
These findings appear online in the Annals of the rheumatic diseases.
Funding for this study was provided by the Arthritis Foundation and by the National Institutes of Health (NIH P30 AR072571).
Neuropathological and clinical findings in young contact athletes exposed to repetitive head impacts
McKee AC, Mez J, Abdulmohammad B, et al. JAMA Neurology. Published online 2023. doi:10.1001/jamaneurol.2023.2907 Full article available for free
Take home message
Less than half of young adults exposed to repetitive head impacts through sports and who suffered from mental health and cognitive disorders before death met clinical criteria for a diagnosis of chronic traumatic encephalopathy (CTE). Other factors may contribute to CTE-like symptoms in this group.
Background
The sports community is increasingly concerned about the long-term consequences of repetitive head impacts (e.g. CTE). CTE can cause cognitive impairment, mental health problems and mood disorders. Very few studies have examined the presence of CTE in a large group of young adults, which could provide insight into CTE in former youth athletes without other age-related brain changes.
Study aim
The authors sought to understand the pathological brain changes and symptoms of former contact athletes under the age of 30 at death.
Methods
The authors used donated brains from 152 young individuals (13 to 29 years) with a known history of repeated head impacts. These brains come from the Brain Bank Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE). Researchers contacted next of kin to conduct cognitive and mental health assessments of the donor. A team of four neuropathologists diagnosed CTE or other neurodegenerative diseases based on established evaluation criteria.
Results
Overall, based on the 152 brain samples, 41% of donors had CTE. Of these, all but three brains had only mild CTE. Older donors and former American football athletes with a longer history of participation in contact sports were more likely to develop CTE. Clinical cognitive and mental health problems were common among participants regardless of CTE diagnosis.
Viewpoints
The authors found that ~41% of people under the age of 30 with a history of contact sports and cognitive and mental health problems have CTE. Thus, for individuals under age 30 at death, their cognitive and mental health problems may be caused by something other than CTE (e.g., life stressors, genetics, and other underlying mental health problems). It is important to avoid applying these findings to the broader athletic population because most, if not all, brains were donated due to observed pathology before death. Additionally, this study group was predominantly male (93%) and white (73%), further limiting interpretation.
Clinical implications
In practice, this research suggests that CTE may be just one of many causes of cognitive and mental health problems after exposure to repetitive head impacts through sports. As a result, physicians must be prepared to support patients with mental health needs and promote timely referral to mental health professionals for further care. We must also educate our patients that not all cognitive and mental health problems in athletes are due to CTE and that it remains unknown how many people have CTE among those with or without a history of sports participation.
Questions for discussion
What other factors may contribute to CTE-like symptoms in former contact athletes? What experiences have you had with former/current athletes suffering from CTE or CTE-like symptoms?
related posts
Few definitive CTE cases have been detected with and without history of brain injury and collision sports
Most military service members don’t have to worry about CTE
Treatable conditions should be explored in former athletes with CTE-like symptoms
by Danielle Dupont, PT, DPT, RRS, NASM-CNC – North Central Phoenix
Whether you’re a seasoned marathon runner or just starting your fitness journey, running and physical therapy can play a crucial role in optimizing your performance. PT can also help prevent injuries and promote overall well-being.
Top 10 Reasons Why Runners Should Seek a Physical Therapist:
Injury prevention: Physical therapists can assess your running biomechanics and identify potential problems that could lead to injuries. They can provide personalized advice and exercises to address weaknesses, imbalances or poor running form. Reducing the risk of injuries such as shin splints, stress fractures or runner’s knee.
Rehabilitation: If you have already suffered a running injury, physical therapists can tailor a rehabilitation program to help you recover safely and quickly. They use evidence-based techniques to restore strength, flexibility and range of motion. This allows you to start running again with less risk of new injuries.
Performance improvement: Physical therapists can work with you to improve your running efficiency and technique. They can identify areas where you can improve your stride, posture and gait so you can run faster and with less effort. This can be especially valuable for competitive runners who want to achieve personal bests.
Custom training plans: Physiotherapists can develop personalized training plans that take into account your individual strengths and weaknesses. This can help you avoid overtraining and make safe progress toward your running goals.
Pain Management: If you experience persistent pain during or after running, a physical therapist can provide pain relief strategies such as manual therapy, modalities such as ultrasound or electrical stimulation, and education on self-care techniques.
Biomechanical analysis: A physical therapist can perform a comprehensive assessment of your walking biomechanics. This may include analyzing your footstep pattern, joint movements and muscle activation to recommend appropriate footwear, orthotics or exercises to optimize your walking mechanics.
Postoperative rehabilitation: If you have had surgery for a running injury, physical therapists can guide you through postoperative rehabilitation to ensure a successful recovery and a gradual return to running.
Education and guidance: Physical therapists can educate you on proper warm-up and cool-down techniques, stretching exercises, and injury prevention strategies. They can also give you advice on how to adjust your running program as you get older or encounter new challenges.
Motivation and support: Building a strong relationship with a physical therapist can provide the motivation needed to continue your rehabilitation. They can encourage and support you as you work toward your running goals.
Whole body health: Physiotherapists take a holistic approach to health, taking into account the impact of various factors on your running performance. Including nutrition, sleep and stress management. They can guide you in optimizing these aspects of your life to support your running efforts.
Physiotherapists are movement experts who improve the quality of life through practice-oriented care, patient education and prescribed movement. Seeking the expertise of a physical therapist can be extremely helpful for runners of all levels. Whether you want to prevent injuries, improve performance, or recover from an injury, a physical therapist can provide personalized care and guidance to help you achieve your running goals safely and effectively.
Find a location near you for a free port analysis and tips to start your pain-free running journey.
All participants (demographic and anthropometric data are shown in Table 1) successfully completed the experimental sessions without side effects, except for some cases of mild tingling in the fingers at the end of the measurements. Regarding RTD, three men had to be excluded from the data analyzes because the occlusion of arterial blood flow was not possible with the MS and/or LS cuff due to the painful pinching of the skin fold and the stretching of the cuff up to the yield point. In addition, one female was excluded from data analyzes for vsysRPP, SMO2and tHb because arterial blood flow was already occluded at 20% overlap using the HS cuff.
Table 1 Participant characteristics expressed as means ± standard deviations
Overlap to occlusion
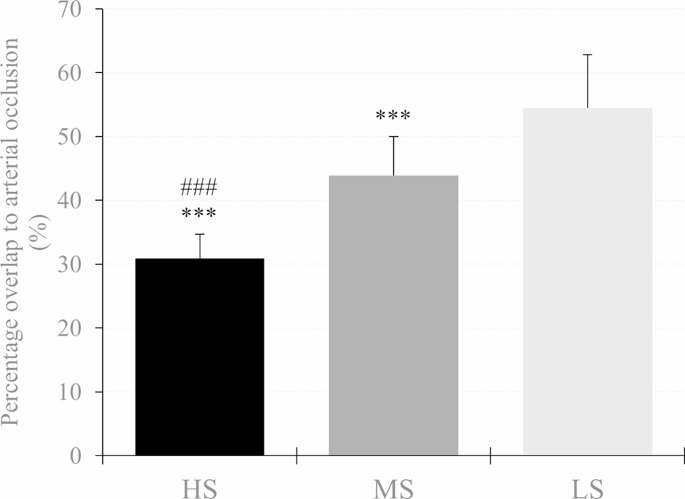
There was a main effect of cuff (F2.62 = 175.679, P< 0.001, theP2= 0.850) and post hoc analysis indicated that RTD was lower in the HS compared to the MS (MD = -13.06% (-16.18 to -9.93%), P< 0.001, D= 2.06) and LS cuff (MD = -23.78% (-26.90 to -20.65%), P< 0.001, D= 3.75). In addition, RTD was also lower using the MS compared to the LS cuff (MD = -10.72% (-13.85 to -7.60%), P< 0.001, D= 1.69). Descriptive data are shown in Table 2; Fig. 3.
Table 2 Hemodynamic, physiological and perceptual responses to progressive practical blood flow restrictions (10%, 20% and 30% overlap relative to the individual’s upper arm circumference) using a high stiffness (HS), medium stiffness cuff ( MS) and low stiffness (LS). Data are expressed as means ± standard deviations
Fig. 3
Percent overlap needed for arterial occlusion in the high stiffness (HS), medium stiffness (MS), and low stiffness (LS) cuff. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ### p < 0.001 respectively
Peak systolic velocity of blood flow
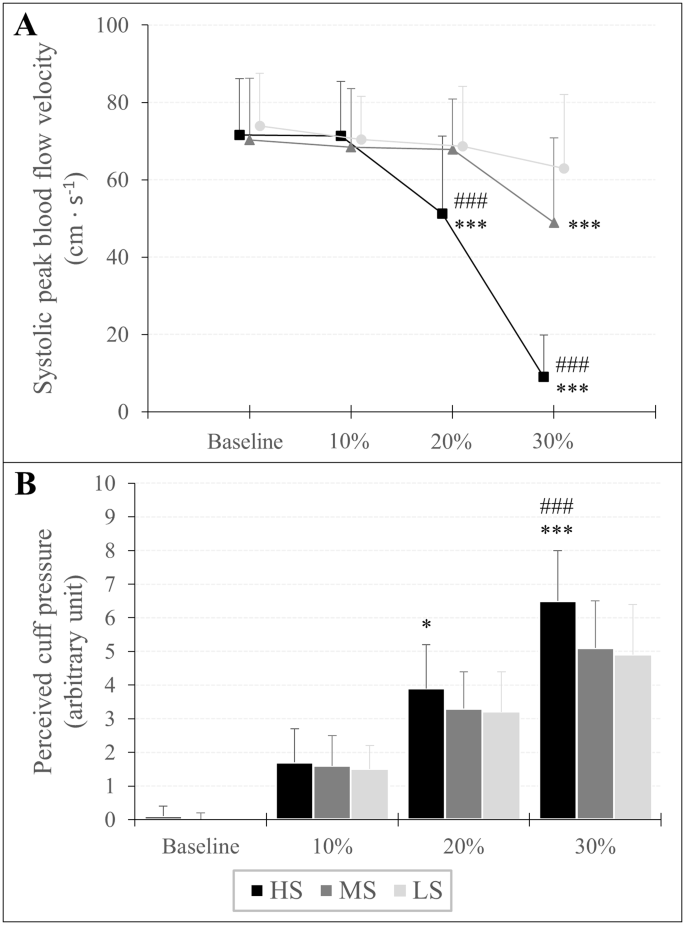
There was an overlap × cuff interaction (F3,642,120,192 = 71.952, P< 0.001, theP2= 0.686) and a main effect of overlap (F1,770,58,422 = 161.427, P< 0.001, theP2= 0.830) and cuff (F2.66 = 50.380, P< 0.001, theP2= 0.604) for vsys. Post hoc analysis showed that vsys was lower at 30% overlap in each cuff compared to baseline (HS: MD = -62.67 cm s− 1(-70.97 to -54.37 cm s− 1 ), P< 0.001, D= 3.95; MS: MD = -21.53 cm s− 1(-29.83 to -13.24 cm s− 1 ), P< 0.001, D= 1.36; LS: MD = -11.02 cm s− 1(-19.31 to -2.72 cm s− 1 ), P< 0.001, D= 0.69). Furthermore, when the HS cuff was applied, vsys was also lower at 20% overlap compared to baseline (MD = -20.51 cm s− 1(-28.80 to -12.21 cm s− 1 ), P< 0.001, D= 1.29). As for cuff differences, vsys was lower at 20% and 30% overlap using the HS cuff compared to the MS (MD = -16.89 cm s− 1(-26.08 to -7.70 cm s− 1 ), P< 0.001, D= 1.07 and MD = -39.91 cm s− 1(-49.11 to -30.71 cm s− 1 ), P< 0.001, D= 2.52, respectively) and the LS cuff (MD = -17.60 cm s− 1(-26.80 to -8.41 cm s− 1 ), P< 0.001, D= 1.11 and MD = -53.99 cm s− 1(-63.18 to -44.79 cm s− 1 ), P< 0.001, D= 3.40 respectively). Furthermore vsys was also lower at 30% overlap using the MS compared to the LS cuff (MD = -14.08 cm s− 1(-23.27 to -4.88 cm s− 1), P< 0.001, D= 0.89). Descriptive data are shown in Table 2; Fig. 4.
Fig. 4
Peak systolic velocity of blood flow (A) and assessment of perceived cuff pressure (B) in response to progressive practical pressure on blood flow restriction, expressed as percent overlap in relation to the individual’s arm circumference. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ###p < 0.001 respectively
Assessment of perceived cuff pressure
An overlap × cuff interaction (F3,946,130,209 = 13.994, P< 0.001, theP2= 0.298) and a main effect of overlap (F1,668,55,046 = 674.771, P< 0.001, theP2= 0.953) and cuff (F2.66 = 11.067, P< 0.001, theP2= 0.251) was found for RPP. A post hoc analysis showed that RPP increased at each %overlap stage compared to baseline for all three cuffs (HS10%: MD = 1.57 au (0.98 to 2.17 au), P< 0.001, D= 1.51; HS20%: MD = 3.80 au (3.21 to 4.40 au), P< 0.001, D= 3.66; HS30%: MD = 6.41 au (5.82 to 7.00 au), P< 0.001, D= 6.16; MS10%: MD = 1.54 au (0.94 to 2.13 au), P< 0.001, D= 1.48; MS20%: MD = 3.32 au (2.72 to 3.91 au), P< 0.001, D= 3.19; MS30%: MD = 5.03 au (4.44 to 5.63 au), P< 0.001, D= 4.84; LS10%: MD = 1.46 au (0.87 to 2.05 au), P< 0.001, D= 1.40; LS20%: MD = 3.18 au (2.59 to 3.77 au), P< 0.001, D= 3.05; LS30%: MD = 4.95 au (4.36 to 5.55 au), P< 0.001, D= 4.76). Regarding differences between cuffs, RPP was higher using the HS cuff with 20% overlap compared to the LS cuff (MD = 0.71 au (0.06 to 1.37 au), P= 0.016, D= 0.69) and with an overlap of 30% compared to Member States (MD = 1.43 (0.78 to 2.09 au), P< 0.001, D= 1.38) and LS cuff (MD = 1.54 au (0.89 to 2.19 au), P< 0.001, D= 1.48). Descriptive data are shown in Table 2; Fig. 4.
Oxygenation of the muscles
SMO2: There was an overlap × cuff interaction (F2,374,78,326 = 3.232, P= 0.037, theP2= 0.089) and a main effect of overlap (F1,297,42,808 = 404,914.= P< 0.001, theP2= 0.925) and gender (F1.33 = 5.096, P= 0.031, theP2= 0.134) for SMO2. Post hoc analysis showed that SMO2 was lower at 20% overlap (HS: MD = -9.94% (-12.43 to -7.45%), P< 0.001, D= 1.15; MS = -8.28% (-10.77 to -5.78%), P< 0.001, D= 0.96; LS: MD = -7.42% (-9.98 to -5.00%), P< 0.001, D= 0.87) and 30% overlap (HS: MD = -17.46% (-19.95 to -14.97%), P< 0.001, D= 2.02; MS: MD = -14.91% (-17.42 to -12.42%), P< 0.001, D= 1.72; LS: MD = -13.79% (-16.28 to -11.30%), P< 0.001, D= 1.59) compared to baseline. Furthermore, the main effect of sex indicated that regardless of overlap and cuff used, SMO2 was lower in men than in women (MD = -5.16% (-9.80 to -0.51%), P= 0.031, D= 0.60).
tHb: An overlap × cuff (F3,072,101,386 = 6,440, P< 0.001, theP2= 0.163) and overlap × sex interaction (F1,187,39,158 = 14.814, P< 0.001, theP2= 0.310) and a main effect of overlap (F1,187,39,158 = 117,125.= P< 0.001, theP2= 0.780) and gender (F1.33 = 27.981, P< 0.001, theP2= 0.459) was found for tHb. Post hoc tests showed that tHb was higher at 20% overlap (HS: MD = 0.13 au (0.09 to 0.18 au), P< 0.001, D= 0.45; MS: MD = 0.10 au (0.05 to 0.14 au), P< 0.001, D= 0.32; LS: MD = 0.06 au (0.02 to 0.11 au), P< 0.001, D= 0.20) and 30% overlap (HS: MD = 0.22 au (0.18 to 0.27 au), P< 0.001, D= 0.75; MS: MD = 0.17 au (0.12 to 0.21 au), P< 0.001, D= 0.55; LS: MD = 0.15 au (0.10 to 0.19 au), P< 0.001, D= 0.45) compared to baseline. Moreover, tHb was already higher at a 10% overlap using the HS (MD = 0.05 au (0.00 to 0.09 au), P= 0.018, D= 0.16) compared to baseline. Regarding sex differences, post hoc analysis showed that regardless of cuff, tHb was higher by 10% (MD = 0.06 au (0.01 to 0.10 au), P= 0.003, D= 0.20), 20% (MD = 0.15 au (0.11 to 0.20 au), P< 0.001, D= 0.52) and 30% overlap (MD = 0.24 au (0.19 to 0.29 au), P< 0.001, D= 0.80) in men, while in women tHb was only higher during a 30% overlap compared to baseline (MD = 0.12 au (0.07 to 0.16 au), P< 0.001, D= 0.39). In addition, tHb was higher in men compared to women at baseline (MD = 0.51 au (0.31 to 0.70 au), P< 0.001, D= 1.69). Descriptive data are shown in Table 2.
Injuries to the anterior cruciate ligament (ACL), located in the knee, are commonly thought to be caused by acute traumatic events, such as sudden twists. Led by researchers at Penn State, new work analyzing an animal model of ACLs suggests that such injuries may also occur as a result of chronic overuse, specifically due to a reduced ability to repair microtraumas associated with overuse. Importantly, according to the team, women are less able to heal from these microtraumas than men, which could explain why women are two to eight times more likely to tear their ACL ligaments than men.
“ACL tears are one of the most common injuries, affecting more than 200,000 people in the US each year, and women are known to be particularly susceptible,” said lead researcher Spencer Szczesny, associate professor of biomedical engineering and orthopedics and rehabilitation at Penn . Stands. “Although recent research suggests that chronic overuse may lead to ACL injuries, no one has yet examined the different biological responses of female and male ACLs to applied force.”
From the research, published in the Journal of Orthopedic Researchresearchers placed ACLs from deceased male and female rabbits in a custom-built bioreactor that simulated the conditions of a living animal but allowed for direct observation and measurement of the tissue. They then applied repetitive forces to the ACLs that mimicked the forces that would naturally occur during activities such as standing, walking and trotting, and measured the expression of genes related to healing.
In male samples, the team found that low and moderate applied forces, such as those that would occur while standing or walking, resulted in increased expression of anabolic genes, which are related to building molecules needed for healing. In contrast, greater applied forces, such as would occur with repetitive trotting, reduced the expression of these anabolic genes. However, in female samples, the amount of force applied did not affect the level of anabolic gene expression.
“It didn’t matter whether there was low, medium or high activity in women,” said Lauren Paschall, a biomedical engineering graduate student at Penn State and first author of the paper. “Female ACLs exposed to chronic use simply did not heal as well as male ACLs, which may explain why women are prone to injuries. This supports the hypothesis that non-contact ACL injuries are attributed to microtraumas associated with chronic overuse that predisposes the ACL make for injuries.” .”
According to the researchers, one explanation for the gender differences the team observed could be due to the higher amounts of estrogen in women.
“Some studies have shown that the overall effect of estrogen on ACL injury is negative,” Paschall said. “Specifically, studies have shown that human women are more likely to tear their ACLs during the preovulatory phase, when estrogen levels are high, than during the postovulatory phase, when estrogen levels are low.”
She said the team plans to further investigate the role of estrogen in ACL injuries.
Szczesny noted that although the team’s research did not take place in humans, the findings may indicate that providing women with additional recovery time after injuries could be beneficial.
“Ultimately, this work could also help identify targets for therapies to prevent ACL injury in women,” he said.
Other Penn State authors on the paper include Sabrina Carrozzi, graduate student; Erdem Tabdanov, assistant professor of pharmacology; and Aman Dhawan, professor of orthopedics and rehabilitation.
The Orthopedic Research and Education Foundation and the Congressional Directed Medical Research Program supported this research.
Post-injury outcomes following non-sports related concussion: a CARE Consortium study.
Roby PR, Mozel AE, Arbogast KB, Buckley T, Caccese JB, Chrisman SP, Clugston JR, Eckner JT, Esopenko C, Hunt T, Kelly LA, McDevitt J, Perkins SM, Putukian M, Susmarski A, Broglio SP, Pasquina PF , McAllister TW, McCrea M, Head CL; Researchers from the CARE consortium. J Athl train. September 8, 2023. doi: 10.4085/1062-6050-0181.23. E-publishing prior to printing. PMID: 37681681.
Full text freely available
Take home message
Athletes who sustain a non-sports-related concussion, compared to a sport-related concussion, are more likely to delay reporting, take longer to return to play, and have more symptoms.
Background
Most concussions are not related to sports, but most concussion research includes only sports-related concussions. When non-sports-related concussions are reported in the literature, participants come from a specialized concussion clinic or emergency department, potentially biasing the population toward those with more severe injuries or longer recoveries.
Study objectives
The authors examined the reporting characteristics and clinical outcomes of non-sports-related concussions among collegiate athletes.
Methods
The authors used data from the NCAA-DOD CARE Consortium. They grouped the participants based on the mechanism of their concussion: sports-related or non-sports-related. The authors only analyzed a person’s first concussion. Demographic information, injury information, and outcomes include, but are not limited to, age, gender, race, ethnicity, sport, history of concussion, the physician who made the initial diagnosis, time of reporting, delayed onset of symptoms, and a graduated symptom checklist. The authors also analyzed recovery outcomes, including duration of symptoms, provider who cleared the patient, and whether the patient experienced a slow recovery, which was defined as ≥14 days to asymptomatic or ≥24 days to indefinite return to play.
Results
The authors were able to analyze 3,500 people who suffered a concussion, 555 of which were non-sports related. Women suffered more than twice as many (23% versus 10%) non-sports-related concussions as men. The most common mechanisms of non-sports-related concussions were falls, slips or trips (28%), being hit by an object (26%), car accidents (20%) and unintentional contact with another person (9%). Patients who suffered a non-sports related concussion were less likely to report it immediately. They were four times more likely to require hospital transport, had greater severity of symptoms, longer duration of symptoms and more days lost due to injury. Athletes with a non-sports-related concussion were 1.5 times more likely to have a slow recovery and a greater chance of being diagnosed and cleared by a primary care physician than athletes with a sports-related concussion.
Viewpoints
Providers should keep in mind that patients who sustain a non-sports-related concussion are more likely to delay reporting, have a higher symptom burden, and take longer to recover. Athletic trainers must appreciate the unique challenges a patient with a non-sports-related concussion experiences in order to provide the same level of high-quality care.
Clinical implications
Sports medicine personnel can serve as a resource and advocate for education and referrals for patients who sustain a non-sports-related concussion. It is also important to emphasize to athletes the importance of reporting all concussions immediately, regardless of whether they occur during sport.
Related posts
Don’t wait any longer and report your concussion today CDC HEADS UP program increases concussion knowledge and injury communication
Written by Mitch Barnhart Reviewed by Jeffrey Driban