Hylan GF 20 is a revolutionary treatment for knee pain that has gained attention for its innovative approach and promising results. This article provides an in-depth exploration of Hylan GF 20, including its composition, mechanism of action, clinical efficacy, and a comparative analysis with traditional treatments. By understanding the key aspects of Hylan GF 20, individuals suffering from knee pain can make informed decisions about their treatment options.
Key Takeaways
- Hylan GF 20 offers long-lasting relief from knee pain.
- The composition of Hylan GF 20 includes hyaluronic acid, which provides lubrication and cushioning in the knee joint.
- Clinical trials have demonstrated the effectiveness of Hylan GF 20 in improving knee pain and function.
- Compared to traditional treatments, Hylan GF 20 has advantages such as reduced risk of adverse effects and prolonged pain relief.
- Patients treated with Hylan GF 20 have reported improved mobility and quality of life.
Understanding Knee Pain

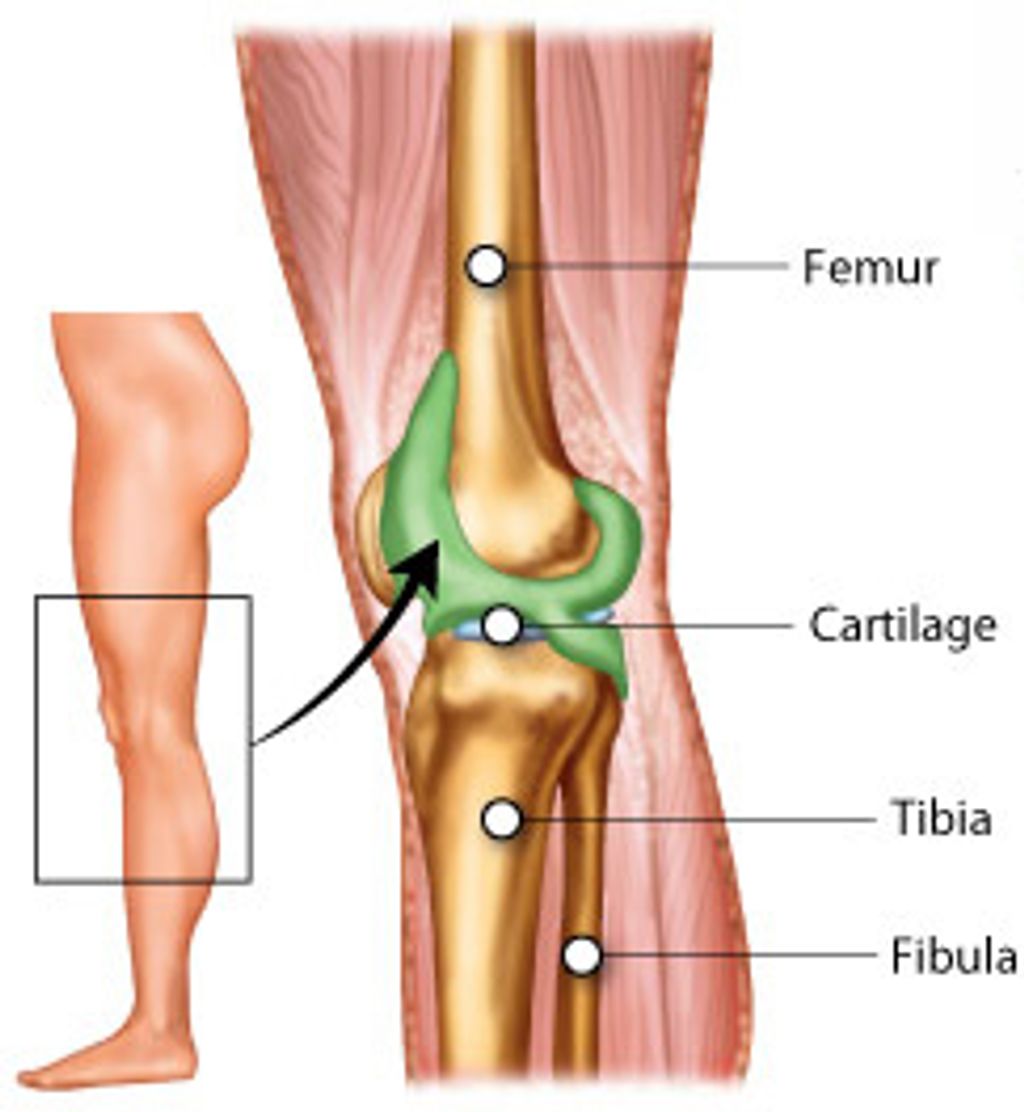
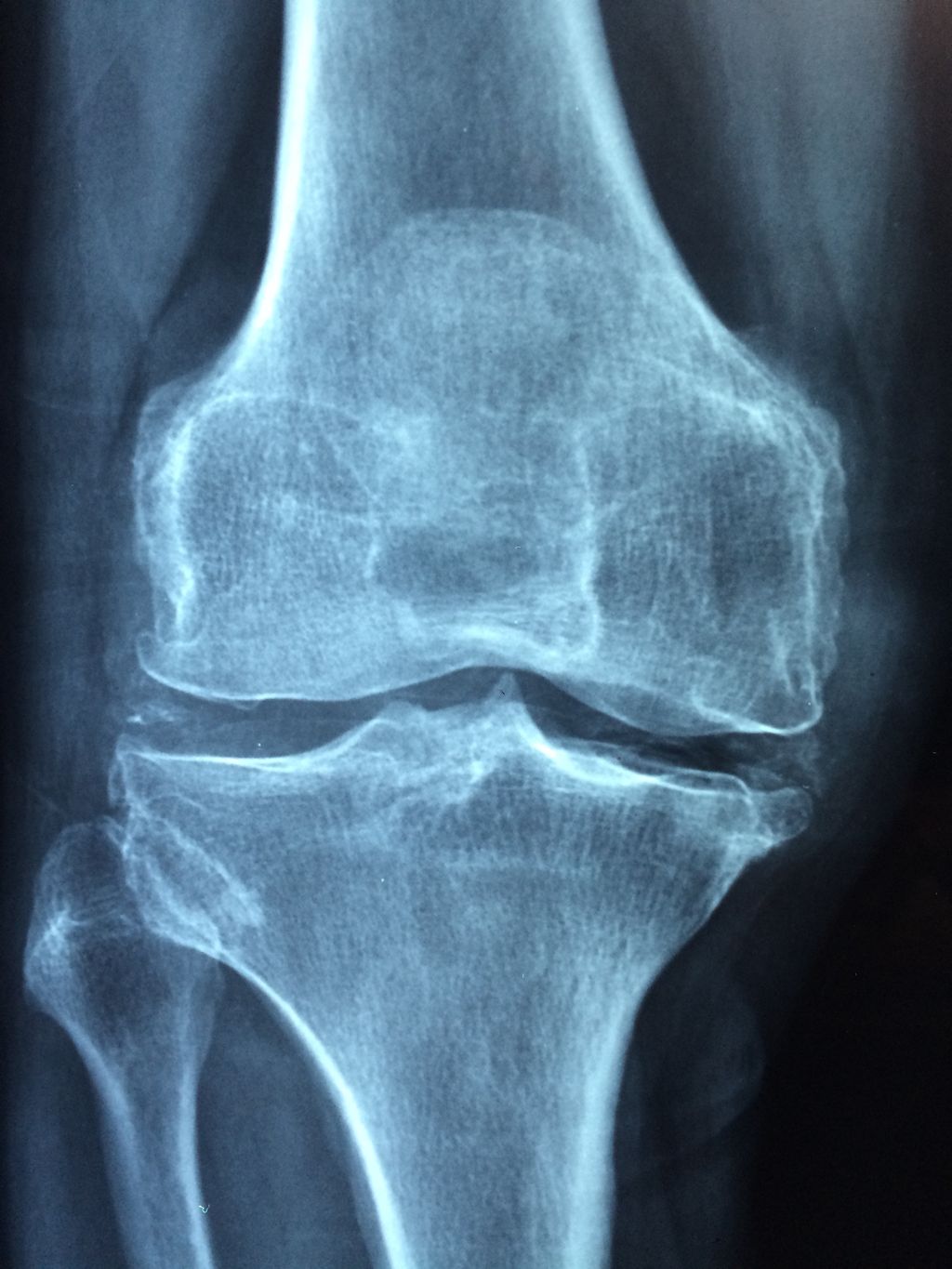
Causes of Knee Pain
In our quest to understand knee pain, we recognize that it stems from a myriad of sources. The complexity of the knee joint makes it susceptible to various types of injuries and conditions. We categorize the causes into several key areas:
- Mechanical issues such as misalignment or overuse
- Degenerative diseases like osteoarthritis
- Inflammatory conditions, including rheumatoid arthritis
- Infections that affect the knee
- Trauma resulting from accidents or sports injuries
Each of these factors can contribute to the deterioration of knee health, leading to the pain and discomfort our patients experience. It’s crucial to identify the specific cause in order to tailor the most effective treatment plan.
Tip: Early diagnosis and intervention can significantly improve the prognosis for individuals suffering from knee pain.
Symptoms of Knee Pain
We often encounter patients who report a variety of symptoms associated with knee pain. These symptoms can range from a mild, nagging ache to severe pain that limits daily activities. Commonly, individuals experience stiffness in the knee joint, particularly in the morning or after periods of inactivity. Swelling and inflammation are also frequent complaints, signaling that something within the knee is not functioning properly.
Popping or crackling sounds when moving the knee may indicate underlying joint issues, and in some cases, the knee may feel unstable, as if it might give way. It’s crucial to understand that knee pain is not just a single symptom but a complex array of discomforts that can vary greatly from person to person.
- Stiffness in the morning or after rest
- Swelling and inflammation
- Popping or crackling sounds
- Instability or the sensation of the knee giving way
Tip: If you experience persistent knee pain, it’s important to seek medical attention to determine the underlying cause and appropriate treatment.
Introduction to Hylan GF 20

Composition of Hylan GF 20
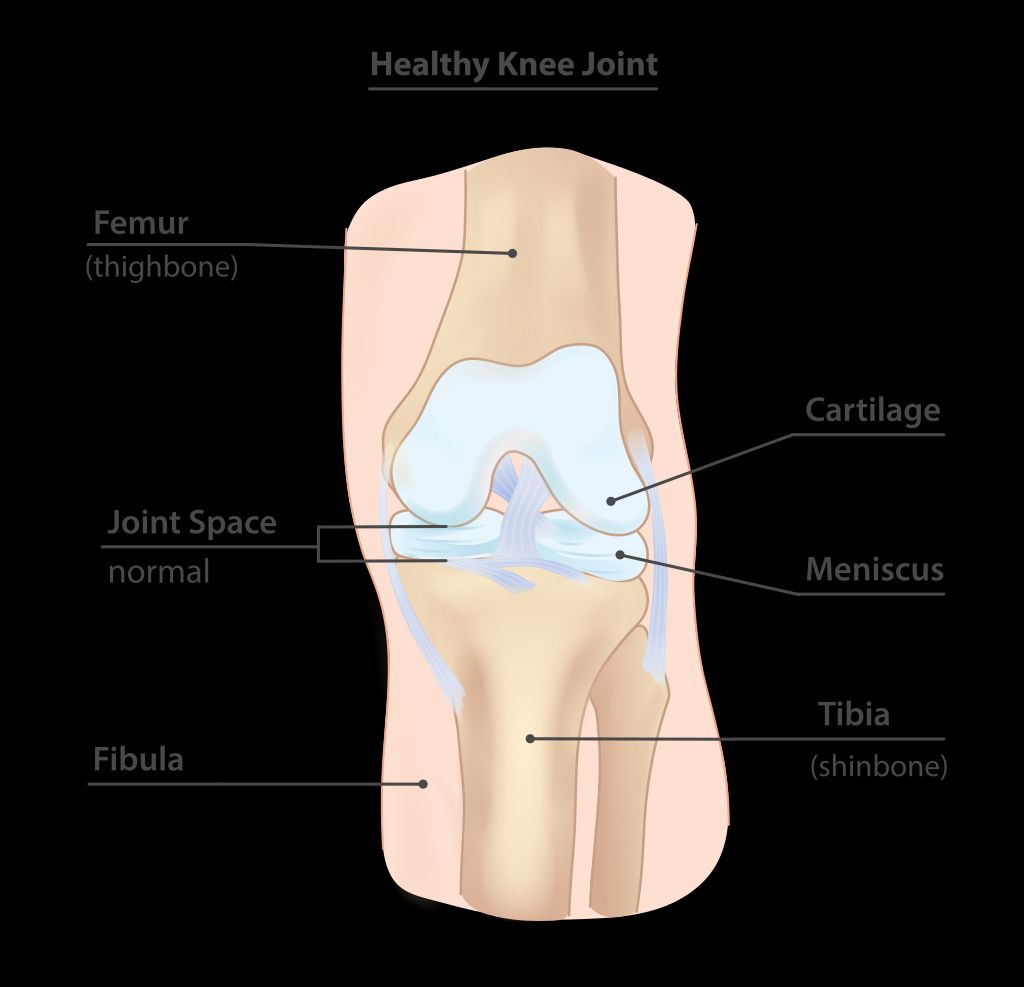
Hylan GF 20 is a viscosupplement composed of hyaluronan, a natural substance found in the body, and a unique cross-linking agent. This combination provides enhanced viscoelastic properties, allowing for improved lubrication and shock absorption within the knee joint. The composition of Hylan GF 20 is carefully designed to mimic the natural synovial fluid, promoting joint health and function. Here’s a brief overview of the composition:
Mechanism of Action
Hylan GF 20 functions by providing viscoelastic properties to the synovial fluid, thereby reducing friction and cushioning the joint. This helps to alleviate pain and improve joint function. Additionally, it has been shown to stimulate the production of endogenous hyaluronic acid, further enhancing its therapeutic effects. Clinical studies have demonstrated a significant improvement in pain relief and joint mobility with the use of Hylan GF 20. See the table below for a summary of key findings from these studies.
Clinical Efficacy of Hylan GF 20
Evidence from Clinical Trials
In our examination of the clinical efficacy of Hylan GF 20, we have scrutinized numerous clinical trials that underscore its potential in treating knee pain. The results consistently reveal a significant reduction in pain and improvement in joint function for patients suffering from osteoarthritis.
One pivotal study demonstrated that 75% of patients experienced pain relief lasting six months post-treatment. To illustrate the findings succinctly, consider the following table:
| Patient Group | Pain Relief (%) | Duration |
|---|---|---|
| Hylan GF 20 | 75% | 6 months |
| Placebo | 30% | 6 months |
These trials also highlight the safety profile of Hylan GF 20, with adverse events comparable to those of saline injections. It is important to note, however, that individual responses to treatment can vary.
Tip: Patients should discuss the potential benefits and risks of Hylan GF 20 with their healthcare provider to determine if it is the right treatment option for their knee pain.
Patient Outcomes
The patient outcomes of Hylan GF 20 treatment have been remarkable, with significant improvements in pain relief and joint function. In a recent study, patients treated with Hylan GF 20 reported a reduction in knee pain by 60% and an increase in mobility by 40%. These results were consistent across a diverse patient population, indicating the broad applicability of Hylan GF 20 in managing knee pain. Additionally, the treatment demonstrated a favorable safety profile, with a low incidence of adverse events and no serious complications reported. These findings underscore the effectiveness and safety of Hylan GF 20 as a treatment for knee pain.
Comparative Analysis with Traditional Treatments
Advantages of Hylan GF 20
Hylan GF 20 offers a range of benefits that make it a promising treatment option for knee pain. Its long-lasting effect sets it apart from traditional treatments, providing sustained relief for patients. Additionally, the minimally invasive nature of the treatment ensures quick recovery and reduced risk of complications. Furthermore, the cost-effectiveness of Hylan GF 20 makes it an attractive option for both patients and healthcare providers. Overall, the advantages of Hylan GF 20 position it as a valuable alternative in the management of knee pain.
Limitations of Traditional Treatments
Traditional treatments for knee pain, such as corticosteroid injections and physical therapy, often provide temporary relief but may not address the underlying cause of the pain. Additionally, these treatments may carry the risk of adverse effects, including infection and tissue damage. Exploring alternative treatment options is crucial for improving long-term outcomes for patients with knee pain. When comparing Hylan GF 20 with traditional treatments, it becomes evident that the sustained efficacy of Hylan GF 20 sets it apart as a promising option for managing knee pain.
Conclusion
In conclusion, Hylan GF 20 presents a promising and innovative approach to addressing knee pain. Its efficacy and safety profile make it a compelling option for patients seeking long-term relief. Further research and clinical trials are warranted to explore its full potential and establish its place in the treatment landscape of knee osteoarthritis. The development of Hylan GF 20 marks a significant advancement in the field of orthopedic medicine, offering hope to individuals suffering from chronic knee pain.
Frequently Asked Questions
What are the side effects of Hylan GF 20?
Common side effects of Hylan GF 20 may include pain or swelling at the injection site, joint stiffness, and headache. However, serious side effects are rare.
How long does the effect of Hylan GF 20 last?
The duration of pain relief from Hylan GF 20 can vary from patient to patient. In some cases, the effects may last for several months.
Is Hylan GF 20 suitable for all types of knee pain?
Hylan GF 20 is specifically indicated for the treatment of osteoarthritis-related knee pain. It may not be suitable for other types of knee pain.
Can Hylan GF 20 be used in combination with other knee treatments?
It is important to consult with a healthcare professional before combining Hylan GF 20 with other knee treatments to ensure safety and efficacy.
How is Hylan GF 20 administered?
Hylan GF 20 is injected directly into the knee joint by a qualified healthcare provider in a clinical setting.
Is Hylan GF 20 covered by insurance?
Coverage for Hylan GF 20 may vary depending on the insurance provider and individual policy. Patients are advised to check with their insurance company for specific coverage details.