Inverted knees, also known as genu recurvatum, is a condition where the knees bend backwards, causing discomfort and difficulty in movement. This article explores the anatomy, causes, symptoms, diagnosis, and treatment options for managing inverted knees.
Key Takeaways
- Understanding the anatomy and causes of inverted knees is essential for effective treatment and management.
- Physical therapy plays a crucial role in strengthening the muscles around the knee and improving flexibility.
- Bracing and support devices can help stabilize the knee joint and reduce strain on the inverted knees.
- Surgical treatment for inverted knees may involve realignment procedures and a comprehensive rehabilitation process.
- Regular orthopedic evaluations are important for monitoring the progress of inverted knee treatment and addressing any potential complications.
Understanding Inverted Knees

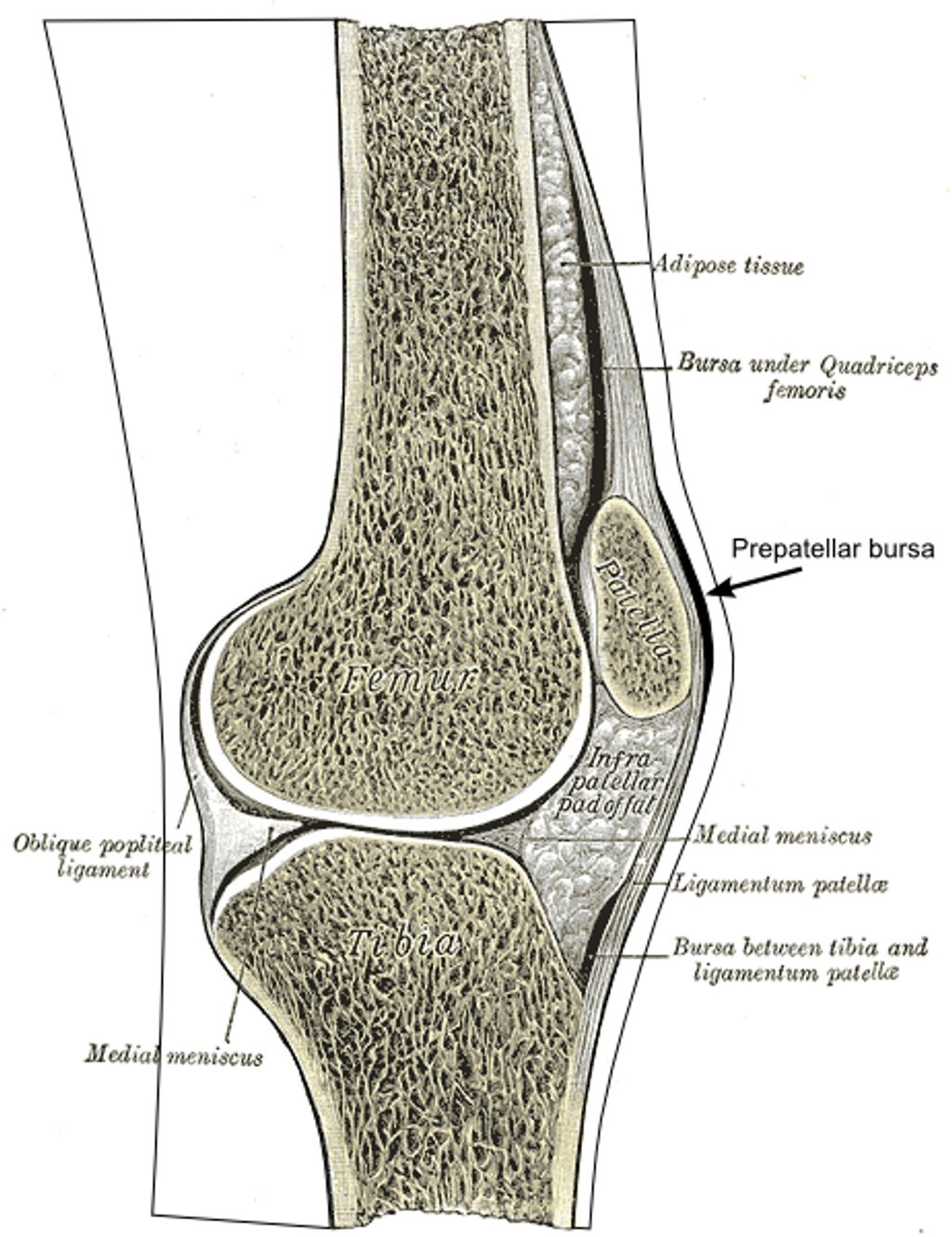
Anatomy of Inverted Knees
Inverted knees, also known as genu varum, are characterized by an inward deviation of the knees. This condition can affect individuals of all ages, from children to adults. The alignment of the lower extremities plays a crucial role in weight-bearing and locomotion. Understanding the anatomy of inverted knees is essential for evaluating the impact of this condition on musculoskeletal function. The table below summarizes the key anatomical features of inverted knees:| Feature | Description || — | — || Femoral-Tibial Angle | The angle formed by the intersection of the femur and tibia. || Joint Space Width | The distance between the femur and tibia at the knee joint. || Patellar Alignment | The position of the patella in relation to the femur and tibia. |
Causes of Inverted Knees
We recognize that the etiology of inverted knees is multifaceted, often involving a combination of genetic and environmental factors. Genetic predisposition plays a significant role, as the condition can run in families. However, environmental influences, such as repetitive stress on the knees from certain sports or occupations, also contribute to the development of this condition.
Injuries and muscle imbalances are other critical factors that can lead to inverted knees. For instance, damage to the knee ligaments or muscles can alter leg alignment, causing the knees to invert. Additionally, muscle weakness, particularly in the muscles around the hips and thighs, can exacerbate this misalignment.
- Genetic Predisposition
- Repetitive Stress
- Injuries and Muscle Imbalances
- Muscle Weakness
Tip: Strengthening exercises for the hips and thighs can help in managing knee alignment and reducing the risk of inverted knees.
Symptoms of Inverted Knees
Inverted knees can cause discomfort and affect our daily activities. It’s important to pay attention to subtle changes in the alignment of the knees, such as inward pointing of the knees during standing or walking. These changes may indicate the presence of inverted knees and should be evaluated by a healthcare professional. Additionally, individuals with inverted knees may experience instability during physical activities, which can lead to further complications. It’s crucial to recognize these symptoms early and seek appropriate medical advice.
Diagnosing Inverted Knees

Physical Examination
Upon completion of the physical examination, we carefully analyze the patient’s gait, joint stability, and range of motion. Additionally, we assess for any signs of discomfort or pain during movement. This comprehensive evaluation informs our decision-making process and guides the development of a personalized treatment plan.
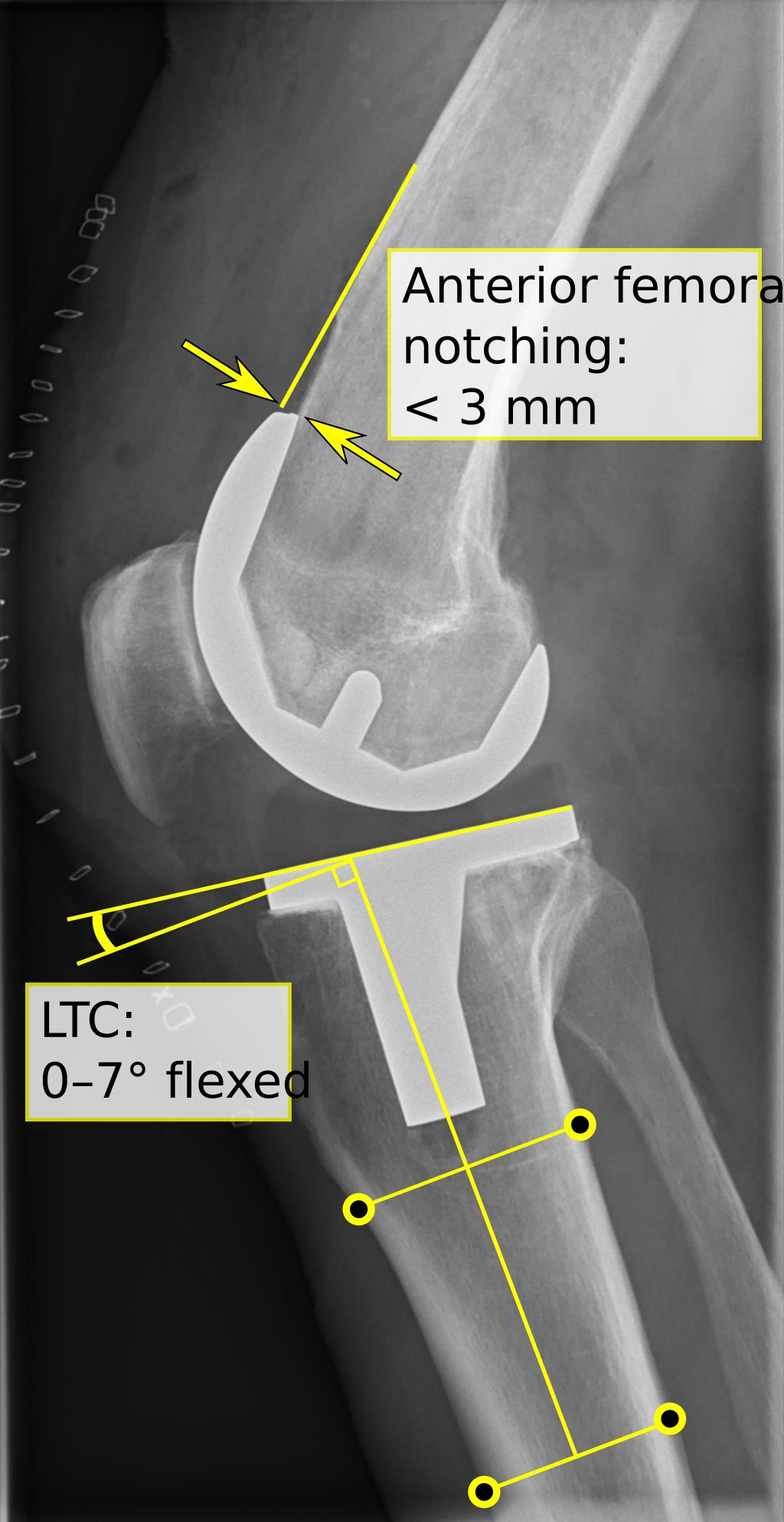
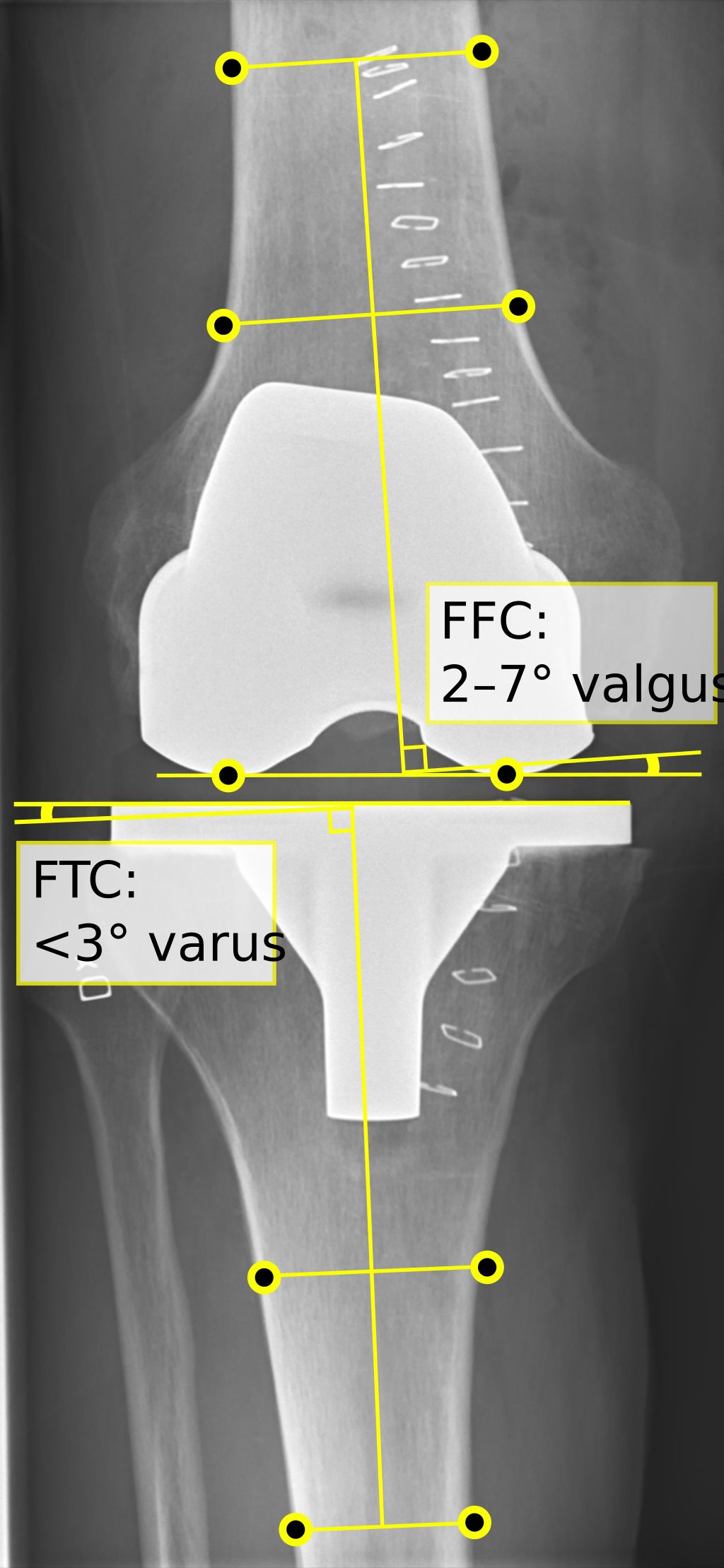
In some cases, imaging tests such as X-rays, MRIs, or CT scans may be utilized to further assess the alignment and condition of the knee joint. These diagnostic tools provide valuable insights into the structural integrity and any potential abnormalities.
Furthermore, the orthopedic evaluation involves a detailed assessment of the patient’s medical history, previous injuries, and lifestyle factors that may contribute to the condition. This holistic approach enables us to consider all relevant factors when determining the most effective course of action.
Lastly, it is important to note that the results of these diagnostic procedures are crucial in establishing a precise diagnosis and formulating an evidence-based treatment strategy.
Imaging Tests
In our assessment of inverted knees, we place significant emphasis on imaging tests. These tests provide us with a detailed view of the knee’s structure, allowing us to identify any abnormalities or underlying conditions that may be contributing to the inversion. Common imaging tests include X-rays, which can reveal bone deformities, and MRI scans, which offer a more comprehensive look at both bone and soft tissue.
- Magnetic Resonance Imaging (MRI):* Provides detailed images of soft tissues such as ligaments, tendons, and cartilage.
- X-ray:* Useful for detecting bone deformities and ruling out other conditions.
- Ultrasound:* Can assess the soft tissue structures around the knee and their dynamic function.
Remember, the choice of imaging test will depend on the individual’s specific condition and the information required to formulate an effective treatment plan.
Orthopedic Evaluation
After the orthopedic evaluation, we carefully assess the patient’s range of motion, joint stability, and gait. Additionally, we may conduct specialized tests to evaluate ligament and tendon function. We prioritize a comprehensive approach to ensure accurate diagnosis and personalized treatment plans. This may involve collaborating with other healthcare professionals to gather a holistic view of the patient’s condition. In some cases, a table summarizing the results of the evaluation may be beneficial for tracking progress and informing treatment decisions.
Non-Surgical Treatment Options

Physical Therapy
Physical therapy plays a crucial role in the management of inverted knees. It is a comprehensive approach that focuses on improving strength, flexibility, and range of motion in the affected knees. Our team emphasizes the importance of personalized exercise regimens tailored to each patient’s specific needs. Additionally, we track progress through regular assessments to ensure that the therapy is yielding the desired results. Here’s a brief overview of the key components of physical therapy for managing inverted knees:
- Strength Training: Targeted exercises to build muscle strength and stability around the knee joint.
- Flexibility Exercises: Techniques to enhance the flexibility of the knee joint and surrounding muscles.
- Range of Motion Activities: Controlled movements to improve the range of motion in the knee joint.
By incorporating these elements into our physical therapy programs, we aim to optimize the functional capacity of the knees and enhance overall mobility and comfort.
Bracing and Support
After discussing the benefits of bracing and support in managing inverted knees, we can see that these interventions play a crucial role in providing stability and reducing discomfort. Bracing helps to align the knee joint, while support aids in distributing weight more evenly. It’s important to note that the effectiveness of these interventions may vary depending on the severity of the condition and individual response. Additionally, a table comparing different types of braces and their features can provide valuable insights for patients and healthcare professionals alike. This table can include information on material, adjustability, and recommended usage. Furthermore, a bulleted list outlining the key considerations for selecting the appropriate brace can help patients make informed decisions. Remember, proper fitting and regular assessment are essential for optimal outcomes.
Pain Management
After exploring various non-surgical treatment options, we have found that physical therapy is an essential component of managing inverted knees. It focuses on strengthening the muscles around the knee joint and improving flexibility. Additionally, bracing and support can provide stability and reduce discomfort during physical activities. Pain management techniques, such as medication and ice therapy, are also crucial for alleviating discomfort and promoting mobility. Here’s a brief overview of the non-surgical treatment options:
| Treatment Option | Description |
|---|---|
| Physical Therapy | Strengthens muscles and improves flexibility |
| Bracing and Support | Provides stability and reduces discomfort |
| Pain Management | Alleviates discomfort and promotes mobility |
It’s important to note that these non-surgical treatment options may vary based on individual needs and the severity of the condition. Seeking professional guidance is essential for determining the most suitable treatment plan for each patient.
Surgical Treatment for Inverted Knees

Surgical Procedures
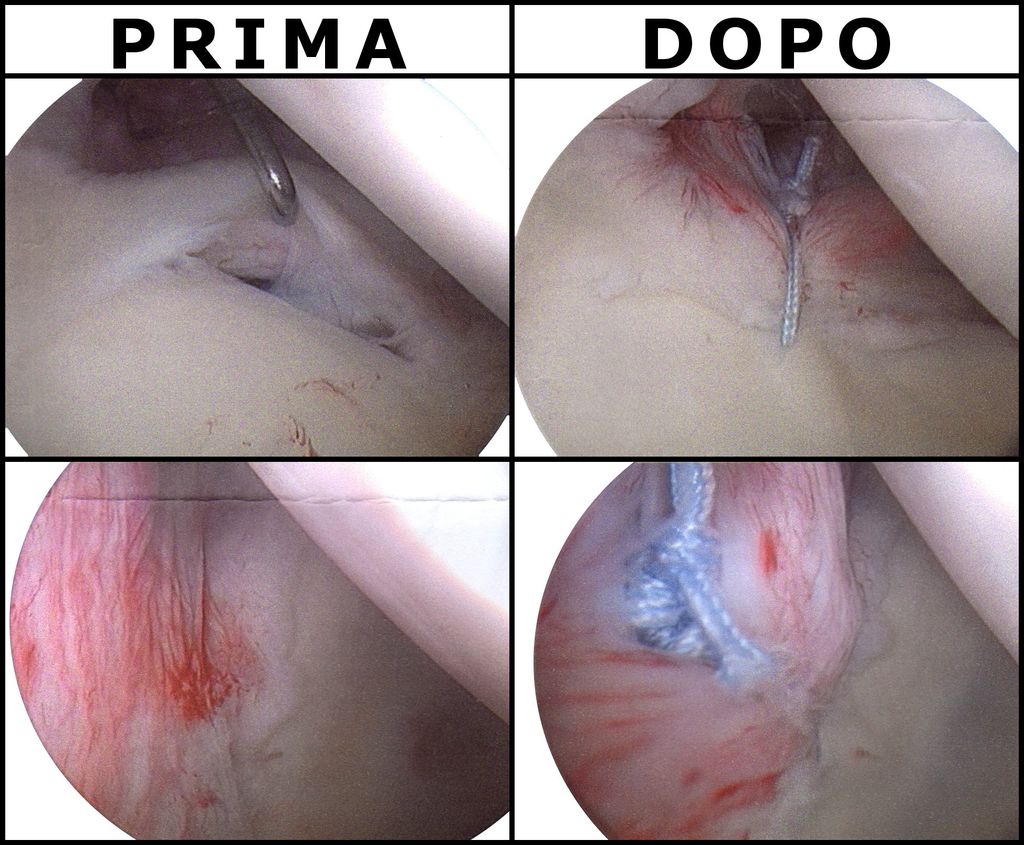
Surgical procedures for treating inverted knees are crucial for addressing severe cases. These procedures may include realignment osteotomy, soft tissue release, and ligament reconstruction. Each procedure is tailored to the individual’s specific condition and needs.
- Realignment Osteotomy: This procedure involves cutting and repositioning the bone to correct the alignment of the knee joint.
- Soft Tissue Release: This technique focuses on releasing tight or contracted soft tissues around the knee joint to improve mobility and function.
- Ligament Reconstruction: This surgical intervention aims to repair or replace damaged ligaments, restoring stability and strength to the knee.
Tip: Post-surgery rehabilitation plays a vital role in optimizing outcomes. Adhering to the prescribed rehabilitation plan and closely following the guidance of healthcare professionals is essential for a successful recovery.
Rehabilitation Process
Following surgical intervention for inverted knees, we embark on a critical phase: the rehabilitation process. This journey is tailored to each individual’s needs, aiming to restore knee function and strength. We typically observe a phased approach, starting with gentle range-of-motion exercises and gradually incorporating strength training and functional activities.
In the initial weeks, patients may experience varying degrees of discomfort and swelling. It’s essential to adhere to the prescribed pain management plan and to monitor for any signs of complications. As we progress, we introduce more demanding exercises, always within the patient’s tolerance levels.
Rehabilitation Timeline:
- Week 1-2: Gentle range-of-motion exercises, swelling control, and pain management.
- Week 3-6: Gradual introduction of weight-bearing activities and strength exercises.
- Week 7-12: Increased exercise intensity and functional training.
Remember, the path to recovery is not always linear. A client’s recovery from knee surgery was going well until a setback at week 10. Despite setbacks, overcoming them with the right strategies is possible.
We encourage patients to maintain open communication with their rehabilitation team, reporting any concerns or unusual symptoms immediately. It is through this collaborative effort that we can ensure the best possible outcome for our patients.
Potential Risks and Complications
After undergoing surgical treatment for inverted knees, it is important to be aware of the potential risks and complications that may arise. These can include infection, blood clots, and nerve damage. Additionally, there is a possibility of prolonged recovery time and the need for further interventions. It is crucial to closely follow post-operative care instructions and attend all scheduled follow-up appointments to monitor and address any issues that may arise. Vigilance and proactive communication with your healthcare provider are essential for ensuring a successful recovery.
Conclusion
In conclusion, the management of inverted knees presents a complex challenge, requiring a multifaceted approach that encompasses both conservative and surgical interventions. While physical therapy and orthotic devices play a crucial role in mitigating symptoms, surgical correction may be necessary in severe cases. The decision-making process should be guided by a thorough assessment of the individual’s condition, taking into account factors such as age, activity level, and overall health. Further research and advancements in medical technology are essential for enhancing the efficacy of treatment options for this condition.
Frequently Asked Questions
What are the common causes of inverted knees?
The common causes of inverted knees include genetics, muscle imbalances, and abnormal bone structure.
Can physical therapy help with inverted knees?
Yes, physical therapy can be beneficial for strengthening muscles, improving flexibility, and correcting alignment in inverted knees.
Are there non-surgical treatment options for managing inverted knees?
Yes, non-surgical treatment options include physical therapy, bracing, and pain management techniques.
What surgical procedures are available for treating inverted knees?
Surgical procedures such as osteotomy and realignment surgery may be recommended for severe cases of inverted knees.
What are the potential risks and complications of surgical treatment for inverted knees?
Potential risks and complications of surgical treatment include infection, blood clots, and nerve damage.
How long is the rehabilitation process after surgical treatment for inverted knees?
The rehabilitation process after surgical treatment can vary, but it typically involves physical therapy and gradual return to normal activities.