Description: American Hip Institute is a successful sports medicine practice supported by a very active Research Foundation led by Dr. Dumb. As a Clinical Research Intern you will have the opportunity to be responsible for a variety of clinical, surgical and research roles including: maintaining a comprehensive surgical database, writing or acting as a medical assistant in the clinic, assisting with the writing of research studies and supporting research processes such as journal publication, conference submissions and prospective study management. The skills acquired in clinical, surgical and research environments offered at this institute provide participants with an excellent foundation for their medical career.
Duration and reimbursement: This position is offered for a period of 10 months and includes a stipend of $800 per month. Clinical Research Assistants are asked to begin immediately in Summer 2023 and end in July 2024.
If you are interested in applying, you can send a motivation letter and CV to:
Benjamin Hill, MD This email address is being protected from spambots. You need JavaScript enabled to view it.
Researchers from Keele University’s School of Medicine have found that painkilling drugs – commonly known as ‘analgesics’ – are being widely prescribed across England to people with inflammatory arthritis, despite little research evidence that they improve pain in these patients, and studies which show that they can cause serious side effects. -Effects.
The study, funded by the National Institute for Health and Care Research (NIHR) and published in the journal RheumatologyResearch found that all types of painkillers were widely prescribed: About two-thirds of patients with inflammatory arthritis received a prescription painkiller in 2020, and one in four patients received long-term prescription opioids. Many of these long-term prescriptions for opioids started around the time people were diagnosed with inflammatory arthritis.
Worryingly, many types of painkillers were more likely to be prescribed to people with inflammatory arthritis who were older (and therefore most at risk of side effects from medicines), were women, lived in deprived areas and in the north of England. This suggests there is unfairness about pain, or the way pain is managed in people with inflammatory arthritis in the NHS.
Inflammatory arthritis groups together conditions that cause joint pain and swelling. Its three main types – rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis – affect more than 1% of adults in England. Pain is a major challenge for patients with inflammatory arthritis, with most patients suffering daily pain and viewing pain as the area of their health they most want to see improved.
The crucial first step in improving NHS pain care for these patients is understanding how it is managed. To address this, the research team looked at data from a large GP database – the Clinical Practice Research Datalink Aurum – which currently contains information from more than 1,400 GP practices across England.
They looked at data from 2004 to 2020 to understand how different types of painkillers are prescribed to patients with inflammatory arthritis, and how this varies between people based on their age, gender, ethnicity and where they live.
Lead author Dr Ian Scott said the findings show there is an urgent need to improve the way pain is treated in patients with inflammatory arthritis in the English NHS. He described the fact that one in four patients were prescribed long-term opioids, and in 2020, one in ten patients were prescribed gabapentinoids, despite these medications having many potential side effects and no clinical trials showing they help when taken on be used this way. , as “very worrying”.
There are better ways to treat pain in patients with inflammatory arthritis that have been shown to help in clinical trials. These include reducing joint inflammation using specialized disease-modifying medications and exercise. We need to shift the focus of pain care from the long-term use of ineffective painkillers to the use of treatments that have been shown to help.”
Dr. Ian Scott, lead author
Source:
Magazine reference:
Scott, I.C., et al. (2023) Painkiller prescribing in patients with inflammatory arthritis in England: observational studies in the Clinical Practice Research Datalink. Rheumatology. doi.org/10.1093/rheumatology/kead463.
My gift to my community is the easy-to-navigate, clickable transcript.
Bone turnover markers:
“Therapeutic targets provide medical information that a physician can use to monitor physiological improvements with repeated testing. These can improve assessment of bone loss and are critical to management of therapy. Just as you would practice hitting the bullseye To improve your skills as a competitive shooter, we can refine treatment by targeting abnormal physical signs, symptoms and laboratory test results and then applying therapy to correct those abnormal findings.”
R. Keith McCormick, DC from his upcoming book: Great Bones: Control Your Osteoporosis.
This transcript will be your guide in understanding the need for bone turnover markers, what they are, and the importance of “test, don’t guess.” These tests can be done in between your bone density testing (DXA). The Bone Marker PDF is a clickable guide to make navigating the document easier.
Strongly recommended:
Click below to get a copy of my PDF guide to bot turnover marking.
The link asks for your email address so the guide can be emailed to your inbox.
This promotion will add your name to my email list that I email bi-monthly at “All things bone related”.
You can unsubscribe at any time.
Please enjoy the transcription below.
Interview PDF
This PDF is clickable. You can select a bone marker you want to learn more about and then return to the table of contents.
Do you already know you want to work with my team?
It is best to start with a comprehensive private session where a plan is designed specifically for you and your bones.
Investment in your bones:
$200, includes next steps and follow-up notes via email.
Let me support your bones
Receive an in-depth, tailor-made private session
Book a Private Coaching with Irma
Join our amazing Bone Tribe community
Get the support and information you need to live fearlessly with your bone diagnosis
Are you one of the 80% of adults suffer from adrenal fatigue?
Worried about how stress can silently sabotage your bones and contribute to osteoporosis?
Ready to discover one groundbreaking, cost-free strategy that would revolutionize your bone health?
Then you shouldn’t miss this episode!
Come with me as I sit down Dr. Tricia Pingel, a licensed naturopathic doctor known as the Adrenal Whisperer. Delve deep into the mysteries of adrenal gland healthdiscover the surprising ties with stress and osteoporosisand find out how restore your bone strength andrevive your vitality.
Episode timeline
0:00 – Episode begins
1:37 – Introduction to Dr. Tricia Pingel
3:08 – Dr. Pingel’s journey to tackling adrenal fatigue and stress
5:06 – Identifying adrenal gland problems in men and women aged 50-70+ with osteopenia and osteoporosis
6:40 – Recommended tests for suspected adrenal gland problems
8:15 – The link between stress, adrenal glands and bone health
11:39 – Everyday stressors that affect health
15:14 – Actionable steps for self-assessment and improvement
17:54 – The profound impact of intentional breathing on reducing stress, improving bone health and promoting overall well-being
20:15 – Connection between thyroid and bone health
24:02 – Dancing for healthier bones and better mental health
30:05 – Simple ways to return to the present moment
34:30 – Where to meet Dr. Pingel and how she can help you on your journey to better bone health
Below you will find resources from Dr. Tricia Pingel!
>> Read more about Dr. here. Tricia on her website!
>> Connect with Dr. Tricia on Facebook
>> Follow Dr. Tricia on Instagram
>> Follow Dr. Tricia on TikTok
>> Connect with Dr. Tricia on LinkedIn
What can you do to support your bone health and this podcast?
1. Press the “Subscribe” button on your respective podcast player (i.e. Apple, Google, Spotify, Stitcher, iHeart Radio and TuneIn). Never miss an episode that can help improve your bone health.
2. Leave a review. The more positive ratings and reviews and the more subscribers we have, the more people can find us and get the answers to the questions they need. Thank you! 🙂
3. Tell a friend about The Bone Coach Podcast or share via text, email or social. Do you know of a Facebook group where people can benefit from this information? Feel free to hit any of the share buttons below.
About Dr. Tricia Pingel:
Dr. Pingel, a certified naturopathic doctor, is known as the Adrenal Whisperer. She has dedicated almost 15 years of her career as an adrenal gland and stress expert.
She helps Rockstar women look and feel great by restoring their adrenal glands without the use of drugs. Her specialty is identifying the cause of health problems and restoring health and youthful energy.
Since learning that she was one of the 80% of adults suffering from adrenal fatigue, Dr. Pingel passionately taught about the impact that stress has on the adrenal glands. She has helped thousands of people restore their adrenal glands, resulting in the reversal of many other health symptoms, including perimenopause. Her greatest joy is guiding people to return to their happy, vibrant and energetic selves.
Dr. Pingel has appeared in nearly a dozen television shows, including: The Dr. Ax Show, Ask the Expert with JJ Virgin, Good Morning Arizona, The Arizona Daily Mix with Brad Perry and many others.
She has contributed to many publications, most notably: Mind Body Green, Prevention Magazine, Yoga Journal, Eat This Not That, MSN.com, Vitamin Shoppe, Health Central, Birdie and Livestrong.
Dr. Pingel, affectionately known as The Hip Hop Adrenal Doc, can often be found on social media cheering on her two boys at soccer, making healthy vegan recipes in her kitchen, and cuddling her three dogs and cats at home with her husband. Phoenix, Ariz.
Medical disclaimer
The information shared above is for informational purposes only and is not intended as medical or nutritional therapy advice; it does not diagnose, treat or cure any disease or condition; it should not be used as a substitute or substitute for medical advice from physicians and trained medical professionals. If you are under the care of a healthcare professional or are currently taking prescription medications, you should discuss any changes in your diet and lifestyle or possible use of nutritional supplements with your doctor. You should not stop prescribed medications without first consulting your doctor.
Do you know how many people walk around with a torn meniscus without knowing they have a tear?
💥About 5% of young people and up to 67% of older people have asymptomatic (non-painful) meniscus tears! 💥
How is that possible?
Depending on the type of injury and how it is treated, the symptoms of a meniscus tear may resolve within days to weeks or months; and you may not even know the tear exists!
The initial injury may not even have been severe enough to warrant a visit to an orthopedist or ordering an X-ray or MRI, especially if the knee only hurt for a few days before the pain went away.
Here’s what you need to know about meniscus injuries so they don’t hinder your favorite activities…
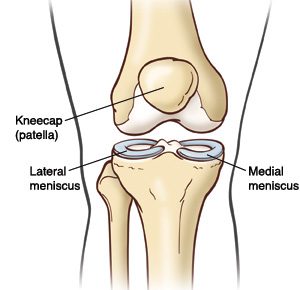
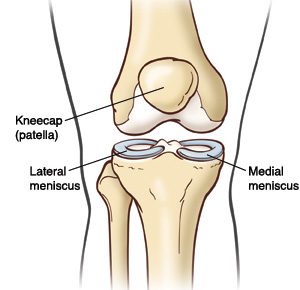
Where is the meniscus?
The meniscus is a “C”-shaped disk made of cartilage that is located in the knee, between the shin bone and the femur. It sits on the weight-bearing surface of the tibia, or tibia, in the joint capsule.
There are two menisci, one on the lateral (outside) of the knee and one on the medial (inside). A healthy meniscus provides space, cushion and lubrication to the joint so that the knee can bend, straighten and bear weight comfortably.
The meniscus is located deep in the knee, along with the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL). Due to their deep location, the menisci do not have a very good blood supply, so certain areas are not likely to heal from an injury.
💥 🤯 However, the fact that the meniscus does not heal properly on its own does not mean that a tear always needs to be repaired!
What does the meniscus do and why is it so important?
Shock absorption: The meniscus acts as a shock absorber for shocks that occur during daily activities, such as walking, running, jumping and sports. As we move, force travels through the foot and through the shin bone to the knee, where the meniscus absorbs and disperses that force through the knee, so the impact is spread out and not concentrated in one area.
Stability: The meniscus also acts as a wedge that supports the front and back of your knee, keeping the knee from going beyond a certain range of motion, such as hyperextension, which puts you at risk for other injuries.
How does the meniscus become injured?
The meniscus is most commonly injured during twisting of the knee when the foot is planted on the ground. Rotational stress or “shearing” can cause the femur and tibia to rotate beyond what the meniscus can handle, resulting in a tear in the cartilage.
Meniscal tears are common in athletes who exert a large amount of force on one leg and twist their body in a different direction, such as football 🏈, soccer ⚽️, lacrosse 🥍, tennis 🎾, or basketball 🏀. Field and field athletes often put their feet down to stop and change direction; and in a split second the knee rotates with enough force to cause a meniscus tear.
Snow sports, such as skiing ⛷ and snowboarding 🏂, also carry a high risk of meniscus injuries. The edge of a ski or board can unexpectedly hit the snow, causing a sudden rotation of the leg. The long lever arm can quickly generate a high-speed rotational force, strong enough to cause meniscus injury.
Meniscal tears occur in people of all ages, including athletes and non-athletes. In middle-aged and older adults, meniscus tears can occur due to wear and tear on the knee joint. As the body ages, degeneration of the cartilage tissue occurs as the joints are exposed to force for years.
Osteoarthritis, a condition in which cartilage wears away over time, is common in older adults and is often accompanied by a torn meniscus. A meniscus tear earlier in life can also make the knee more susceptible to earlier-onset osteoarthritis. That’s why it’s so important to learn the right moves and exercises to protect your knees!
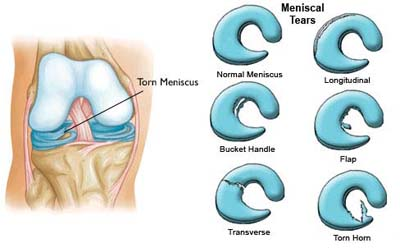
I have a meniscus tear. What now?
Depending on the type of meniscus tear, you may experience symptoms such as pain, swelling, locking, or locking of the knee. Although a meniscal injury cannot be detected on X-rays, it can be diagnosed through a careful examination or an MRI.
Most meniscal tears are initially treated conservatively (without surgery); although an orthopedic doctor may recommend surgery if symptoms persist and daily activities are limited.
Meniscectomy: The most common surgery for a meniscus tear is called a menisectomy, in which the surgeon removes the torn piece of cartilage and cleans up the surrounding ragged tissue. Although it is a surgical procedure, recovery after a meniscectomy is relatively short. Most people can resume daily activities within a few weeks and exercise within a few months.
It is important to add that everyone responds to surgery differently; and a ‘minor’ surgery for one person may be a more stressful experience and longer rehabilitation for someone else.
Meniscus repair: An alternative surgery is a meniscus repair, which is performed when the orthopedic surgeon believes the torn cartilage structure can be sewn together, saving cartilage to prevent osteoarthritis in the future. This procedure is typically performed more in younger people to preserve the cartilage rather than remove it. Recovery from a meniscus repair takes longer than a menisectomy and involves close monitoring of range of motion, weight bearing, and activity progression during rehabilitation.
Non-surgical treatment A meniscus tear is very common and results in great results in most cases! A diagnosis of a meniscus tear does NOT mean that surgery is always necessary!
Although a meniscus tear will not heal itself, you can strengthen the knee and improve movement patterns to disperse forces and reduce stress at the site of the tear, which will help resolve symptoms.
💪 With the right exercises and learning to move properly, most meniscus tears can be treated conservatively WITHOUT surgical intervention.
💥It’s important to remember that you are not your MRI result; and a meniscus tear should not determine the rest of your life.
How can you treat a meniscus injury without surgery?
A meniscus injury must be properly guided through the healing phases. Pain and inflammation are likely to be early symptoms, while stiffness and weakness may be the main complaints after a few weeks. Dealing with injuries with “PEACE & LOVE” is a good reference for dealing with acute injuries.
To return to normal activities, follow the guidance of your physical therapist, who will develop a care plan for strengthening, balance training, improving mobility, and returning to exercise.
👉Doing the right exercises with good form and consistency will significantly increase your ability to recover from a meniscus tear and prevent future injuries.
If you’re ready to start strengthening at home, ACL Strong has courses that include all the necessary components of exercise and movement to train your body and brain to protect your knees now and for the long term.
Whether you have a torn meniscus or not, doing the right exercises the right way will keep your knees strong and stable, so you’ll be less prone to further injury and better equipped to maintain an active lifestyle for as long as you want. to lead!
Rheumatoid arthritis (RA) is a chronic autoimmune disease that affects millions of people worldwide. It is characterized by joint inflammation, pain and stiffness, which can significantly affect a person’s quality of life. Understanding the mechanisms behind inflammation in rheumatoid arthritis is crucial for developing effective treatments and improving patient outcomes.
Introduction
Rheumatoid arthritis is a chronic inflammatory disease that mainly affects the joints. It is an autoimmune disease in which the body’s immune system mistakenly attacks its own tissues, leading to inflammation and damage. This chronic inflammation can lead to joint deformity, loss of function and disability if left untreated. Therefore, gaining insight into the mechanisms that drive inflammation in rheumatoid arthritis is crucial.
What is inflammation?
Inflammation is a natural process that occurs when the body’s immune system responds to injury or infection. It involves the release of various chemical signals and the activation of immune cells to protect the body and promote healing. While acute inflammation is a temporary response to a specific trigger, chronic inflammation, as seen in rheumatoid arthritis, persists for an extended period of time. It is this inflammation that causes the symptoms seen in RA.
Inflammation in rheumatoid arthritis
Rheumatoid arthritis is characterized by persistent inflammation in the synovial joints, mainly affecting the hands, feet and wrists. The synovium, a thin membrane that lines the joints, becomes inflamed, leading to pain, swelling and stiffness. If left untreated, this inflammation can gradually damage the joints, cartilage and surrounding tissues.
Inflammatory mechanisms in rheumatoid arthritis
The inflammatory process in rheumatoid arthritis involves a complex interplay of immune cells, cytokines and genetic factors. Initially, immune cells such as macrophages and dendritic cells are activated, causing an immune response. These cells produce pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-alpha), interleukin-1 (IL-1), and interleukin-6 (IL-6), which play an important role in promoting inflammation and joint destruction . .
The role of the immune system
In rheumatoid arthritis, the immune system plays a crucial role in causing inflammation. T cells and B cells, two types of lymphocytes, are mainly involved in the inflammatory process. T cells recognize specific antigens and release cytokines that further activate immune cells and enhance the inflammatory response. B cells produce autoantibodies that target the body’s own tissues, contributing to tissue damage and inflammation.
Inflammatory mediators
Several inflammatory mediators contribute to the persistent inflammation that occurs in rheumatoid arthritis. Prostaglandins, leukotrienes and cytokines are among the key players in the inflammatory cascade. Prostaglandins and leukotrienes are lipid mediators that promote vasodilation, increase vascular permeability, and recruit immune cells to the site of inflammation. Cytokines, such as TNF-alpha, IL-1 and IL-6, enhance the immune response and support the inflammatory process.
Inflammation and joint damage
The chronic inflammation in rheumatoid arthritis can lead to irreversible joint damage. The continued presence of inflammatory mediators and immune cells promotes the destruction of cartilage and bone. Over time, this can result in joint deformities, loss of mobility and functional limitations. Early intervention to control inflammation is crucial in preventing or minimizing joint damage.
Inflammation and systemic effects
Inflammation in rheumatoid arthritis not only affects the joints, but can also have systemic consequences. Chronic inflammation increases the risk of developing cardiovascular diseases, such as heart attack and stroke. Additionally, it can lead to osteoporosis, a condition characterized by weakened bones, making people more susceptible to fractures. Controlling inflammation in rheumatoid arthritis is therefore essential for overall health and well-being.
Current treatment methods
Treatment for rheumatoid arthritis aims to reduce inflammation, relieve symptoms and prevent joint damage. Conventional medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs), and corticosteroids, are often prescribed to control inflammation and manage pain. Biological therapies, such as TNF inhibitors and interleukin blockers, target specific inflammatory pathways and have revolutionized the treatment of rheumatoid arthritis.
Possible future directions
Research into inflammation in rheumatoid arthritis is constantly evolving, leading to the development of new treatment methods. Emerging therapies, including Janus kinase (JAK) inhibitors and small molecule inhibitors, show promise in targeting specific molecules involved in the inflammatory process. Personalized medicine, based on an individual’s genetic profile, is also an area of active research, aimed at optimizing treatment outcomes and minimizing side effects.
Lifestyle and diet adjustments
In addition to medical interventions, lifestyle changes can play an important role in controlling inflammation in rheumatoid arthritis. Regular physical activity, tailored to individual capabilities, helps reduce joint stiffness and maintain joint flexibility. Following an anti-inflammatory diet rich in fruits, vegetables, whole grains and omega-3 fatty acids can provide essential nutrients and possibly ease symptoms.
Conclusion
Inflammation is a major cause of rheumatoid arthritis and contributes to joint damage and systemic effects. Understanding the complicated mechanisms involved in inflammation can help develop targeted therapies and improve the lives of people with rheumatoid arthritis. By controlling inflammation, maintaining joint function, and taking a comprehensive approach that includes lifestyle changes, people with rheumatoid arthritis can live fulfilling lives with a reduced burden of disease.
The Bone Health & Osteoporosis Foundation (BHOF) is currently collecting written stories as part of a support initiative called Voices of Osteoporosis: Stories of Hope and Inspiration.
If you have experienced osteoporosis as a patient or caregiver, we invite you to share your story.Your story can inspire others to learn how to protect their ability to live their best life and stay strong.
If you are interested in participating in this initiative, please contact us click here to complete a short interest form online. A BHOF representative will then contact you to answer any questions you may have and coordinate the time frame for your submission.
Below are some important details about participating in this initiative:
Examples –click here for a few sample stories that others have shared before: if you scroll down the page, you’ll see some listed and you can click on each story to expand it.
Length – We request that all stories be submitted in a Word document; stories must be written in the first person and are typically about 800 words long.
To process – BHOF only very minimally, if at all, edits each person’s story because we want it to come directly from each person as his or her own lived experience.
Title – Add an inspiring title to your story.
Photos – We request that you submit 2-3 photos of yourself along with your story. At least one of the photos must be horizontal, as it will be placed as the main image at the top of your story web page. The ideal size for the horizontal image is 1400×600.
Release form – Once you complete the online interest form, a BHOF representative will contact you to answer any questions you may have and coordinate the time frame for your submission. At that time they will also ask you that sign this release form and send it back before sharing your story.
Process & BHOF Contact – You can forward all articles to your BHOF contact person by e-mail. They will also help you with any questions you may have throughout the process.
Share your story – Your story may be shared through a variety of channels including the Bone Talk blog, the BHOF website, email communications and social media.
Do you have questions? Your BHOF contact will be happy to help you every step of the way!
by Danielle Dupont, PT, DPT, RRS, NASM-CNC – North Central Phoenix
Whether you’re a seasoned marathon runner or just starting your fitness journey, running and physical therapy can play a crucial role in optimizing your performance. PT can also help prevent injuries and promote overall well-being.
Top 10 Reasons Why Runners Should Seek a Physical Therapist:
Injury prevention: Physical therapists can assess your running biomechanics and identify potential problems that could lead to injuries. They can provide personalized advice and exercises to address weaknesses, imbalances or poor running form. Reducing the risk of injuries such as shin splints, stress fractures or runner’s knee.
Rehabilitation: If you have already suffered a running injury, physical therapists can tailor a rehabilitation program to help you recover safely and quickly. They use evidence-based techniques to restore strength, flexibility and range of motion. This allows you to start running again with less risk of new injuries.
Performance improvement: Physical therapists can work with you to improve your running efficiency and technique. They can identify areas where you can improve your stride, posture and gait so you can run faster and with less effort. This can be especially valuable for competitive runners who want to achieve personal bests.
Custom training plans: Physiotherapists can develop personalized training plans that take into account your individual strengths and weaknesses. This can help you avoid overtraining and make safe progress toward your running goals.
Pain Management: If you experience persistent pain during or after running, a physical therapist can provide pain relief strategies such as manual therapy, modalities such as ultrasound or electrical stimulation, and education on self-care techniques.
Biomechanical analysis: A physical therapist can perform a comprehensive assessment of your walking biomechanics. This may include analyzing your footstep pattern, joint movements and muscle activation to recommend appropriate footwear, orthotics or exercises to optimize your walking mechanics.
Postoperative rehabilitation: If you have had surgery for a running injury, physical therapists can guide you through postoperative rehabilitation to ensure a successful recovery and a gradual return to running.
Education and guidance: Physical therapists can educate you on proper warm-up and cool-down techniques, stretching exercises, and injury prevention strategies. They can also give you advice on how to adjust your running program as you get older or encounter new challenges.
Motivation and support: Building a strong relationship with a physical therapist can provide the motivation needed to continue your rehabilitation. They can encourage and support you as you work toward your running goals.
Whole body health: Physiotherapists take a holistic approach to health, taking into account the impact of various factors on your running performance. Including nutrition, sleep and stress management. They can guide you in optimizing these aspects of your life to support your running efforts.
Physiotherapists are movement experts who improve the quality of life through practice-oriented care, patient education and prescribed movement. Seeking the expertise of a physical therapist can be extremely helpful for runners of all levels. Whether you want to prevent injuries, improve performance, or recover from an injury, a physical therapist can provide personalized care and guidance to help you achieve your running goals safely and effectively.
Find a location near you for a free port analysis and tips to start your pain-free running journey.
You have been diagnosed with osteoporosis or osteopenia and told that exercise can help. But what kind of exercise should you do? How do you know you won’t hurt yourself? What if you’ve never exercised before – how do you even get started? Or if you’re already an exercise enthusiast, what else can you do that you may have overlooked before?
Let’s start by identifying how exercise can benefit your bones. Your bones are living tissue that change thickness, mass and shape with use, just like your muscles. If you wanted to strengthen your muscles, you would use them by pulling objects (like lifting weights) and pushing things (like push-ups). You can strengthen your bones in much the same way.
Your bones adapt and respond to loads by strengthening and strengthening themselves to be able to bear that same load again in the future. When you resist external forces like gravity or weights, your bones reap the reward. On the other hand, not using your bones results in a weakening of their structure and composition. Ever seen the wrist of someone whose cast has just been removed? The wrist size has generally become smaller compared to the other wrist due to its immobility and lack of use. Similarly, NASA research has shown how the absence of gravity in space, which also limits the ability of muscles to pull on bones, causes reductions in bone mass.
To know which type of exercise to engage in, you need to understand that bone is built from three sources when it comes to activity:
1–Weight load
Every time you stand upright, you are working against gravity and supporting the weight of your body. When you crawl or exercise on the floor and support your body with your hands and wrists, you similarly support your weight through your forearm bones.
2–Resistance
Your muscles facilitate movement against additional forces such as weights, bands or pulleys when you exercise. They also contract during daily activities such as carrying objects and moving furniture.
3–Effect
Your bones respond to compressive forces and receive further stimuli to become stronger when a greater force is added that increases the gravitational effect. You’re probably familiar with the term “high impact,” which refers to activities like running and jumping that some people find uncomfortable on their joints as they get older. High impact may not be recommended if you have osteoporosis, and especially if you have had a fracture, but it is important for building maximum bone mass in younger individuals. Low impact can be achieved by repeatedly stomping your feet or dropping your heels.
Knowing which exercises to perform – and even which type of exercise (strength training, Pilates, yoga, HIIT, aerobics, to name a few examples) – depends on your physical capacity, history of physical activity and history of fractures . (If you have had a fracture, you should get permission from your doctor to begin an exercise program.)
To actually increase bone density through exercise after menopause, you probably need high-intensity exercise (lifting heavy weights with a load of at least 80% of the maximum you can lift in a single repetition, along with a high impact). That assumes you don’t have any comorbidities (other conditions) or safety concerns that could make it contraindicated, and you have access to a gym and a trainer to supervise you.
You can also aim to maintain the bone density you have, train for strength and power, and absorb impact at lower loads. No matter what, to avoid injuries, maintain good form by mastering basic movements and training for mobility to achieve the necessary range of motion in your joints.
So when the question arises as to what is the one form of exercise you should be doing for osteoporosis, there is not ONE! The three bone-strengthening elements mentioned above are essential in addition to mobility training, but as the 2014 consensus document ‘Too Fit to Fracture’ pointed out, the best strategy is a multimodal approach that also combines balance and posture training (which we will discuss in this article). a future part of this series.)
A few important things to keep in mind as you begin your training journey:
Be consistent. As with any activity or skill, consistency is key to experiencing results and promoting motivation
Keep challenging yourself. Your bones and muscles are both adaptive organs. So to continue to reap the benefits of exercise, you need to continually and gradually make things harder so you don’t plateau.
Make it fun. If you find it annoying, you’re more likely to procrastinate and avoid it! The best exercise is the one you are going to do.
Sometimes getting started is the biggest hurdle you have to overcome. Know that exercise affects more than just your bones and muscles, joints and soft tissues. It is multisystemic and can improve other systems of your body, such as your digestion, your circulation and your cognition. Furthermore, the more physically active you become, the stronger you feel. One of the often overlooked aspects of osteoporosis is the emotional difficulty that patients experience, regardless of whether they have suffered a fracture. Taking charge of your health through exercise can be one of the best actions you can take to transform yourself from a sense of fear and vulnerability to a sense of confidence and capability.
Stay tuned for the next part of this series demonstrating specific posture training exercises that you can incorporate into your daily life. The smallest change in body position can make a big difference in the experience and effects of your exercise program.
A few weeks ago I worked virtually with a client who was 10 weeks post-surgery. We had started working together around week 3 and so far he had absolutely dominated the recovery process.
In addition to his physical therapy appointments, he would meet with me virtually once a week to determine the best plan of attack for his workouts with the Neubie… and then he would get after it. By incorporating our recommended workouts with the Neubie 3x per day into his routine, he regained full strength and range of motion before 8 weeks post-surgery.
But around week 10, they started increasing the load at his physical therapy appointments. In particular, they started trying to increase the weight of his exercise on the knee extension machine, which led to a bit of pain in the front of the knee. Each day he returned to do the knee extensions, the pain in the front of his knee increased.
As I mentioned earlier, this client met with me once a week, and by the time we met again, he had reached a point where the pain continued even in his daily activities. He no longer had the ability to fully extend the knee without pain.
Despite doing everything right and botching the first eight weeks of the recovery process, he experienced a setback in week 10.
Setbacks can be difficult, but with the right strategies you can overcome them quickly and emerge stronger.