In this study, we showed that among the SE alleles, HLA-DRB1*04:05 in particular was strongly associated with the prognosis of ABT treatment. The allele frequency of HLA-DRB1*04:05 in Japanese patients with ACPA-positive RA is reported to be approximately 28%. Because each individual carries two HLA-DRB1 alleles, approximately half of ACPA-positive RA patients have at least one copy of HLA-DRB1*04:05. And HLA-DRB1*04:05 is strongly associated with the development of ACPA-positive RA, with an odds ratio of 5.023. HLA, which is innate and unchangeable throughout a person’s life, suggests that the association between HLA and treatment prognosis is not merely coincidental. In other words, the HLA genotype is the cause, which leads to favorable treatment results. Although several associations between the efficacy of SE and ABT have been reported9,10,11details at the allele level are limited, even though the significance of the specific alleles as potential biomarkers is promising.
In this study, it was found that only HLA-DRB1*04:05 showed an association with response to ABT treatment, while HLA-DRB1*01:01 and 04:10, which share similar SE, showed no significant association. with treatment responsiveness. In addition to the effect of small sample size, the following reasons can be considered. Amino acids at positions 11, 13 and 67 of HLA-DRB1, which are different amino acid sequences than SE, are also involved in the risk of developing RA. Specifically, it was found that in DRB1*04:05 and 04:10, the valine at position 11 is the amino acid most strongly associated with RA sensitivity, while DRB1*01:01 has another amino acid, leucine, at position 11.25. Furthermore, in a study on the risk of developing RA in the Japanese population, it was shown that the risk of RA differs based on the variant of HLA-DRB1, even sharing the same HLA SE allele. It is suggested that HLA-DRB1*01:01, 04:05 and 04:10 are not bioequivalent23. Furthermore, HLA risk alleles for autoimmune diseases have been reported to significantly influence the pattern of CDR3 sequences in T cell receptors. Furthermore, CDR3 sequences modified by HLA risk alleles have been associated with the recognition of citrullinated antigens. Therefore, sequences other than SE are also believed to be associated with the development and progression of RA and other diseases26.
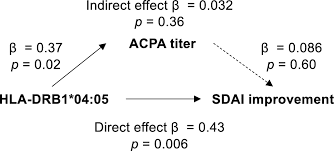
SE and ACPA-positive RA are strongly associated, and ACPA is also associated with the prognosis of ABT treatment27,28. Previous reports have also shown that SE is associated with ABT outcomes, even after adjusting for the effect of ACPA9,10. In this study, both multiple regression analysis and mediation analysis suggested that the effect of the HLA-DRB1*04:05 allele was not an indirect effect mediated by ACPA (Table 4, Figure 2). The impact of SE has been reported to be stronger in ACPA-positive RA than in ACPA-positive non-RA controls29.30. In other words, SE may be involved in the pathogenesis of RA through mechanisms other than direct effects on ACPA positivity. RA risk HLA is robustly associated with CD4 T cell receptor repertoire+ T cells26.31. RA-sensitive HLA alleles, such as HLA-DRB1*04:05, are associated with autoreactive CD4+ T cells, which may be therapeutic targets for ABT.
In this study, methotrexate use was low in the abatacept group. Because in general it has been reported that concurrent use of MTX may not increase the effectiveness of ABT. For example, in a phase III study, ABT did not induce immunogenicity associated with loss of safety or efficacy either with or without MTX32. Also in a retrospective cohort study of RA patients with similar background characteristics who underwent treatment with abatacept, concurrent MTX did not appear to influence clinical outcomes.33. Based on these findings, we believe that ABT would be a suitable treatment option in daily clinical practice in patients with contraindications to MTX.
In this study, the association between the HLA-DRB1*04:05 allele, an SE allele, and favorable treatment outcomes was significant only in ABT-treated patients, but not in those treated with the IL-6 receptor inhibitor TCZ or a TNF drug. inhibitors. This is consistent with the association between the better prognosis with ABT and SE reported in the Early-AMPLE trial comparing ABT with the TNF inhibitor adalimumab.11. SE was also not strongly associated with the efficacy of the JAK inhibitor tofacitinib10. These findings may reflect the difference in mechanism of action between ABT, which inhibits costimulation of antigen-presenting cells, and CD4.+ T cells and IL-6 receptor inhibitors, TNF inhibitors and JAK inhibitors, which are drugs that block inflammatory cytokine signaling.
There are several limitations to this study. First, due to the retrospective nature of this analysis, we cannot exclude the possibility of selection bias. Second, the number in each treatment group is small, so the effect of HLA alleles with small frequency or small effect size may not have been fully realized. Third, since this study was conducted in a single Japanese cohort and there are ethnic differences in the frequencies of the HLA-DRB1 allele, it is necessary to verify whether the results can be generalized to other cohorts, including other ethnic groups.
In conclusion, we analyzed the association between HLA-DRB1 alleles and prognosis in Japanese patients with RA who initiated treatment with ABT, TCZ, and TNF inhibitors, and we showed that among SE alleles, the HLA-DRB1*04 :05 allele was associated with better outcomes with ABT. This study demonstrates the feasibility of stratifying RA patients based on disease risk HLA alleles and supports the need for a larger prospective study.
Leave a Reply