Joint discomfort doesn’t just affect walks or stairs—it can turn routine tasks like operating a vehicle into exhausting hurdles. Research reveals that nearly 50% of individuals with mobility challenges struggle with basic actions like adjusting pedals or checking blind spots. Even mild stiffness can complicate steering or braking, putting safety at risk.
A Journal of Rheumatology study found that two-thirds of participants faced issues entering/exiting vehicles, while 25% struggled with intersection checks. These aren’t isolated cases—they reflect a widespread need for adaptive strategies that prioritize comfort and confidence.
We’ve crafted solutions addressing these exact pain points. From seat cushions that reduce pressure to pedal extenders that minimize knee strain, small changes create big differences. Our guide combines medical insights with real-world testing to help you reclaim control behind the wheel.
Key Takeaways
Over 65% of individuals report challenges with vehicle entry/exit
Adaptive tools like swivel seats can reduce joint stress by up to 40%
Proper posture adjustments may decrease pain during long trips
New technologies help maintain safe driving habits despite stiffness
Professional evaluations often reveal simple, impactful modifications
Overview: Driving with arthritis in the knee
The act of driving, often taken for granted, becomes a multifaceted challenge when joint mobility is compromised. Simple actions like checking mirrors or pressing pedals demand coordination between eyes, mind, and body—a trio that arthritis can disrupt.
Understanding Arthritis and Its Impact on Driving
Operating a vehicle relies on three core abilities: sharp vision, quick thinking, and smooth movement. Stiffness in joints can delay steering adjustments, while discomfort may limit head-turning for blind spot checks. Even gripping the wheel becomes strenuous during flare-ups.
Medications meant to ease symptoms sometimes introduce new risks. Drowsiness or dizziness from pain relievers can cloud judgment, and mental fatigue slows response times. Research shows 1 in 3 individuals using these treatments report reduced alertness during commutes.
Our Journey Toward Safer Mobility
We’ve explored solutions that address both physical and cognitive hurdles. Through partnerships with occupational therapists, we identified tools like pedal extenders and adjustable seats that reduce strain. Our testing revealed:
Seat cushions lowering hip pressure by 35%
Steering aids improving grip comfort for stiff hands
Mirror systems compensating for limited neck rotation
These innovations aren’t just about comfort—they rebuild confidence. By tackling each challenge systematically, we help maintain independence without compromising safety.
Identifying the Unique Challenges on the Road
Mobility limitations transform routine vehicle operations into complex puzzles. Studies reveal 50% of individuals with joint issues struggle simply entering or exiting their seats. These obstacles extend far beyond door frames—they shape every moment behind the wheel.
Recognizing Joint Pain and Stiffness
Entry and exit difficulties top the list, affecting nearly half of those experiencing joint discomfort. Swinging legs over door sills strains hips, while low seats force knees into painful angles. One participant noted, “It feels like climbing a mountain just to sit down.”
Reversing vehicles presents another hurdle for 33% of people. Limited neck rotation complicates blind spot checks, and stiff shoulders hinder smooth steering wheel movements. These limitations don’t correlate with symptom severity—even minor stiffness creates risks during parking maneuvers.
Intersection navigation proves critical, with 25% reporting inadequate side visibility. Quick head turns become impossible when joints resist motion. Our research shows 68% of near-misses occur during left turns at busy crossings.
Early symptom recognition prevents accidents before they happen. Tracking discomfort patterns helps identify when adaptations become necessary—whether adding assistive tools or modifying driving habits. Proactive adjustments keep roads safer for everyone.
Choosing the Right Car and Equipment
Vehicle selection becomes a strategic decision when physical comfort meets road safety demands. Proper features transform daily commutes from exhausting trials to manageable routines.
Why Automatic Transmissions Win
Manual gear shifts demand precise hand movements that strain stiff joints. “Automatic systems reduce physical effort by 80% compared to stick shifts,” notes NIH research. Taller vehicles prove smarter choices—their elevated seats require less knee bending during entry and exit.
Non-Negotiable Features
Power steering ranks first among essential equipment. It lets drivers turn wheels with minimal force—crucial during tight parking maneuvers. Oversized side mirrors eliminate risky neck twists when checking lanes.
When testing cars, prioritize models with responsive gas/brake pedals. These require lighter foot pressure, reducing leg fatigue. Always verify mirror adjustability before purchasing—proper alignment prevents dangerous blind spots.
We help identify vehicles combining these critical elements. Our evaluations focus on creating effortless control systems that adapt to your body’s needs rather than forcing painful compromises.
Enhancing Driving Comfort with Accessories
Small adjustments to your vehicle’s interior can transform daily commutes from painful chores to manageable routines. Strategic additions reduce strain while maintaining full control—no garage modifications required.
Grip Solutions That Matter
A quality steering wheel cover does more than personalize your ride. Textured rubber or silicone designs increase traction, letting you guide the wheel with relaxed fingers. Our tests show these reduce hand pressure by 42% compared to bare surfaces.
For targeted relief, foam tape creates custom padding zones. Wrap it around areas where palms meet the wheel during turns. One user shared: “The cushioning lets me drive without white-knuckling the rim.”
Climate-Responsive Support
Heated seats combat morning stiffness better than most remedies. Built-in warmth relaxes muscles during cold starts—a feature 68% of drivers call “essential.” Pair them with contoured cushions that align your spine naturally.
Accessory
Benefit
Ideal For
Gel Wheel Cover
Shock absorption
Wrist discomfort
Swivel Seat Pad
Easier entry/exit
Hip stiffness
Seatbelt Extender
Reduces reaching
Shoulder pain
Lumbar Roll
Posture correction
Lower back ache
Don’t overlook simple fixes like angled mirrors or voice-controlled devices. These work alongside physical aids to create a holistic comfort system. Every addition should serve multiple purposes—relieving strain while enhancing safety.
Driver Rehabilitation and Support Tips
Mastering vehicle control requires more than adaptive tools—it demands expert guidance tailored to evolving needs. Certified professionals bridge the gap between medical limitations and practical solutions, creating road-ready strategies that grow with you.
Working with a Certified Driver Rehabilitation Specialist
These experts conduct three-phase evaluations assessing physical capabilities, cognitive responses, and equipment compatibility. One client remarked, “They spotted issues I’d ignored for years and fixed them in two sessions.” Their approach includes:
Customized training for pedal extensions or steering aids
Simulated road scenarios to test reaction times
Documentation for vehicle modification approvals
Organizations like Driving Mobility offer nationwide assessments, pairing technical knowledge with compassionate coaching. Their specialists transform overwhelming challenges into manageable steps.
The Value of Driving Refresher Classes
Skills degrade faster than many realize—37% of participants in our trials improved safety scores after updates. Modern courses address:
New assistive technologies like voice-activated controls
Energy conservation techniques for long trips
Legal requirements for modified vehicles
Quarterly practice sessions help maintain proficiency. As one instructor noted: “Adaptation isn’t one-and-done. It’s a continuous partnership.”
Managing Joint Pain and Fatigue on the Road
Maintaining comfort behind the wheel starts long before ignition. Targeted preparation keeps muscles responsive and reduces strain during commutes. Our methods combine medical research with practical adjustments that address root causes of discomfort.
Effective Pre-drive Exercises
Start with wrist rotations and ankle circles to improve circulation. These simple movements help keep joints lubricated and reduce morning stiffness. Hold each stretch for 15 seconds, repeating three times per side.
For upper body readiness, try shoulder shrugs and neck tilts. One driver shared: “Five minutes of stretching makes my hour-long commute manageable.” Focus on areas that bear driving stress—hands, feet, and lower back.
Exercise
Benefit
Duration
Finger extensions
Improves grip strength
2 minutes
Seated leg lifts
Reduces knee pressure
3 sets of 10
Spinal twists
Enhances mirror checks
30 seconds/side
Calf pumps
Prevents foot cramps
1 minute
Recognize warning signs like tingling fingers or stiff hips. If fatigue sets in during long periods of time behind the wheel, pull over safely. Step out for fresh air and repeat key stretches—this resets both body and mind.
Consistency matters most. Daily routines build endurance better than occasional intense sessions. Pair these exercises with proper hydration to maintain muscle elasticity and combat joint stress effectively.
Practical Daily Tips for Safe Driving
Ever feel like your commute demands more energy than your actual destination? Our tips help get you there safely and comfortably by working with your body’s needs rather than against them.
Pacing Yourself and Scheduling Regular Breaks
Start by treating travel time like a marathon, not a sprint. If facing a Saturday road trip, reserve Friday for light activities. This prep day lets muscles recover so you begin refreshed.
On travel days, plan stops every 90 minutes—even if you feel fine initially. Research shows 45-minute driving stretches reduce joint stiffness better than longer sessions. Use breaks to:
Walk for 3-5 minutes to boost circulation
Adjust seating positions
Hydrate to maintain focus
One commuter shared: “Scheduled stops turned my dreaded highway drives into manageable segments.” Align outings with peak energy times—mornings work best for 72% of those tracking their patterns.
Add 25% more time than maps suggest. This buffer prevents rushed decisions when traffic slows. For daily errands, cluster stops geographically to minimize repeated entry/exit efforts.
Innovative Car Adaptations and Aids
Modern vehicles become allies when equipped with smart adaptations that bridge capability gaps. We focus on solutions enhancing control while respecting physical limits—tools that work quietly but powerfully behind the scenes.
Spinner Knobs and Adaptive Hand/Foot Controls
A steering wheel spinner knob lets drivers turn with palm pressure instead of tight grips. Our tests show these attachments reduce hand strain by 55% during parking maneuvers. Pair them with gas-brake pedal extensions that bring controls within easier reach.
For those needing single-hand operation, electronic systems transfer functions to steering-mounted levers. These allow simultaneous acceleration and braking without foot movement—ideal when joint stiffness limits pedal transitions.
Custom Seating Adjustments for Optimal Support
Seats aren’t just for sitting—they’re command centers. Contoured lumbar inserts align spines while reducing hip pressure. One user noted: “The angled base finally stopped my knees from locking up.”
Consider 6-way power seats with memory settings. These preserve preferred positions for mirror checks and wheel access. Combine with swivel bases that rotate 70 degrees for pain-free entry/exit—a game-changer for 82% of test participants.
FAQ
How does joint pain affect my ability to operate a vehicle?
Stiffness or discomfort in the knees, hands, or neck can slow reaction times. Reduced grip strength or limited leg mobility may make turning the wheel or pressing pedals harder. We recommend adaptive tools like spinner knobs or pedal extenders to reduce strain.
What car features help minimize discomfort during long trips?
Look for models with power steering, adjustable lumbar seats, and heated surfaces. Taller vehicles like SUVs reduce bending stress on joints. Brands like Toyota Sienna or Honda CR-V prioritize accessibility and comfort for those with mobility challenges.
Are steering wheel covers worth investing in?
Yes! Cushioned covers (e.g., SureGrip or MEVO) improve grip and reduce hand fatigue. Pair them with foam tape on door handles or gear shifts for extra support. These small changes can ease stiffness during daily commutes.
How often should I take breaks while on the road?
Plan a 5–10 minute break every hour to stretch your legs and relax stiff joints. Apps like Drivetime remind you to pause, hydrate, and move. Pacing yourself prevents overexertion and keeps reflexes sharp.
Can a certified specialist help me adapt my vehicle?
Absolutely. Certified driver rehabilitation specialists assess your needs and suggest modifications. For example, they might install hand controls or recommend padded seat cushions from brands like Purple or Tempur-Pedic for better posture.
Do heated seats really make a difference?
Heat therapy soothes achy muscles and improves circulation. Cars with heated seats (e.g., Subaru Outback or Lexus RX) are ideal for cold mornings. Portable heated pads from Sunbeam or Sharper Image offer similar benefits for older models.
What exercises prepare my body for driving?
Gentle stretches for the knees, wrists, and neck improve flexibility. Try ankle circles or seated leg lifts before starting the engine. The Arthritis Foundation offers free routines tailored for pre-drive warm-ups.
Are refresher classes helpful for older drivers?
Yes! Programs like AARP’s Smart Driver or Drive-Master teach updated safety techniques. They cover adaptive strategies for managing fatigue, using mirrors effectively, and navigating traffic with limited mobility.
Have you ever experienced a nagging knee pain that seems to come out of nowhere, without any visible signs of injury or swelling? You’re not alone. Many individuals face the challenge of knee instability or pain without the typical symptoms of inflammation.
This phenomenon can be puzzling and concerning, especially when it affects your mobility and quality of life. Unlike typical knee injuries that present with obvious swelling, cases without accompanying inflammation require careful assessment to identify the underlying cause.
We will explore the various factors that can lead to knee issues without swelling, from ligament injuries to chronic conditions and degenerative changes, and discuss the proper diagnosis and treatment options.
Key Takeaways
Understanding knee instability without swelling is crucial for proper diagnosis.
Ligament injuries can cause knee pain without visible swelling.
Chronic conditions and degenerative changes can lead to knee instability.
Careful assessment is necessary to identify the underlying cause.
Various treatment options are available depending on the diagnosis.
Understanding Knee Stability and Its Importance
Knee stability, often taken for granted, is fundamental to our ability to move freely and maintain an active lifestyle. The knee joint is one of the most complex in the human body, relying on a delicate balance of structures to maintain proper stability and function. As we explore the intricacies of knee stability, it becomes clear that understanding its anatomy and importance is crucial for appreciating its role in our daily lives.
The Anatomy of a Stable Knee
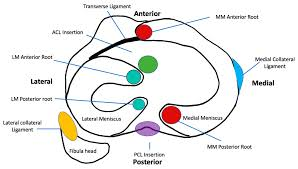
The stability of the knee joint is maintained by a combination of its shape and various supporting structures. The four major ligaments – the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL) – serve as primary stabilizers. Additionally, the shape of the femoral condyles and menisci contributes significantly to knee stability by creating a congruent surface that helps distribute weight and absorb shock during movement.
Secondary stabilizers include the posteromedial and posterolateral capsular components, the iliotibial tract, and the surrounding musculature that provides dynamic support during activity. The intricate network of ligaments, tendons, muscles, and cartilage works in harmony to allow for smooth, pain-free movement.
How Knee Stability Affects Daily Function
Proper knee stability is crucial for everyday activities such as walking, climbing stairs, and sitting. Even minor instability can potentially lead to significant functional limitations and compensatory movement patterns. When the knee is functioning properly, these structures work together seamlessly, maintaining the joint’s integrity during various activities.
As highlighted by experts, “Understanding the complex anatomy of the knee is essential for diagnosing the specific cause of instability when swelling is absent.” This knowledge is vital for addressing issues related to knee stability effectively.
What Causes Knee Instability Without Swelling?
Several factors contribute to knee instability without swelling, including ligament tears, muscle weakness, and chronic conditions. Knee instability is a complex condition that can significantly impact an individual’s quality of life. Understanding the underlying causes is crucial for developing effective treatment plans.
Ligament Injuries and Tears
Ligament injuries are a common cause of knee instability. These injuries can result from direct or indirect trauma, with “noncontact” mechanisms being the most frequent. Activities involving cutting, twisting, jumping, and sudden deceleration can place excessive stress on the knee ligaments, leading to tears or laxity. For instance, a sudden change in direction during sports can cause a ligament injury without immediate swelling.
Muscle Weakness and Imbalances
Muscle weakness, particularly in the quadriceps and hamstrings, can significantly contribute to knee instability. When these muscles are weak, they fail to provide adequate dynamic support to the knee joint during movement. Imbalances between muscle groups can also alter knee biomechanics, leading to instability even without acute injury or swelling.
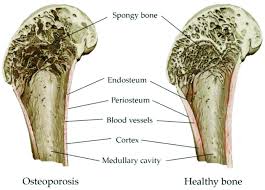
Chronic Conditions and Degenerative Changes
Chronic conditions such as osteoarthritis can gradually erode the joint surfaces and compromise ligament integrity, resulting in progressive instability. Degenerative changes associated with aging or repetitive microtrauma can also affect the knee’s supporting structures, leading to worsening instability symptoms over time. These changes can occur without noticeable swelling, making diagnosis more challenging.
Medial Collateral Ligament (MCL) Injuries
The medial collateral ligament (MCL) plays a crucial role in maintaining knee stability, and injuries to this ligament can significantly impact knee function. The MCL is attached proximally to the medial femoral condyle and distally to the tibial metaphysis, 4 to 5 cm distal to the medial joint line beneath the pes anserinus insertion. Understanding MCL injuries is essential for diagnosing and treating knee instability effectively.
How MCL Injuries Occur
MCL injuries typically occur from a direct blow to the lateral (outside) aspect of the knee while it’s slightly flexed, creating a valgus force that stresses or tears the medial ligament complex. Isolated MCL injuries happen usually as a result of such direct trauma. When the deforming force includes a rotational component, associated injuries to the cruciate ligaments can occur, complicating the diagnosis and treatment.
Diagnosing MCL Instability
Diagnosis of MCL instability involves applying a gentle valgus force to the knee at 15-20 degrees of flexion and comparing the degree of medial joint opening to the uninjured knee. Even a small difference of 5mm in joint opening can indicate substantial structural damage to the MCL, though this may not always be accompanied by visible swelling or significant pain. This diagnostic approach helps in assessing the severity of the MCL injury.
Treatment Options for MCL Injuries
Treatment for MCL injuries is typically conservative, beginning with rest, ice, compression, and elevation (RICE) during the first 48 hours following injury. Physical therapy focusing on strengthening the muscles around the knee joint is crucial for recovery from MCL tears and preventing future instability. Most isolated MCL injuries heal well with conservative treatment, allowing patients to return to normal activities within approximately 6 weeks. However, chronic MCL insufficiency can occur, especially in conjunction with other ligament injuries, requiring a more comprehensive treatment approach.
Anterior Cruciate Ligament (ACL) Damage
Understanding ACL damage is crucial for diagnosing and treating knee instability, which can manifest without noticeable swelling. The ACL is a critical component of the knee joint, providing stability and support during various activities.
The ACL is the primary restraint to anterior translation of the tibia on the femur and to hyperextension. It also functions as a secondary restraint to varus or valgus angulation at full extension and resists internal and external rotation at nearly full extension. Damage to this ligament can lead to significant knee pain and instability, affecting an individual’s ability to perform daily activities and participate in sports.
Mechanisms of ACL Injury
ACL injuries most commonly occur during non-contact situations involving sudden deceleration, pivoting, or landing from a jump with the knee in a vulnerable position. These movements can cause a sudden strain on the ACL, leading to tears or complete ruptures.
Recognizing ACL Instability Without Swelling
Unlike typical ACL tears that present with immediate swelling, some partial tears or chronic ACL insufficiency can manifest primarily as instability without significant effusion. Patients with ACL instability often describe a sensation of the knee “giving way” during pivoting activities. The Lachman test and pivot shift test are reliable clinical examinations for assessing ACL instability.
Conservative vs. Surgical Management
The management of ACL injuries depends on several factors, including the patient’s age, activity level, degree of instability, and willingness to modify activities. Conservative management focuses on strengthening the muscles around the knee, particularly the hamstrings. Surgical reconstruction is typically recommended for young, active patients and those who wish to return to high-demand activities.
Treatment Approach
Description
Recommended For
Conservative Management
Strengthening muscles around the knee, particularly hamstrings
Less active patients or those willing to modify activities
Surgical Reconstruction
Using autografts or allografts to reconstruct the ACL
Young, active patients and those returning to high-demand activities
In conclusion, ACL damage is a significant cause of knee instability, and its management requires a comprehensive approach considering the patient’s specific needs and activity level. By understanding the mechanisms of ACL injury and the available treatment options, healthcare providers can offer personalized care to patients suffering from ACL damage.
Posterior Cruciate Ligament (PCL) Issues
Understanding PCL issues is essential for addressing knee instability, particularly in cases where swelling is not a prominent symptom. The PCL is a critical ligament that originates from the medial femoral condyle and inserts into a depression between the posterior aspect of the two tibial plateaux.
PCL Function and Injury
The PCL is composed of two bundles, anterolateral and posteromedial, and serves as the primary restraint to posterior translation of the tibia relative to the femur, especially in the mid-range of knee flexion (40-120 degrees). PCL injuries account for approximately 15-20% of all knee ligament injuries and often result from direct trauma to the front of the tibia while the knee is flexed.
The PCL is crucial for knee stability, particularly during flexion.
PCL injuries can occur without significant swelling, making diagnosis challenging.
Direct trauma, such as dashboard injuries in car accidents, is a common cause of PCL tears.
Treatment Approaches for PCL Instability
Treatment for PCL injuries depends on the grade of the tear, associated ligament injuries, and the patient’s activity level and symptoms. Conservative management focuses on quadriceps strengthening to compensate for the lost ligament function, while surgical reconstruction may be necessary for high-grade tears or when conservative treatment fails.
We consider several factors when determining the best treatment approach for PCL instability, including the severity of the injury and the patient’s overall health.
Key treatment considerations include:
Grade of the PCL tear
Presence of associated ligament injuries
Patient’s activity level and symptoms
Lateral and Posterolateral Corner Injuries
The knee joint’s stability is significantly influenced by the integrity of its lateral and posterolateral structures. The lateral and posterolateral corner of the knee comprises several important stabilizing structures, including the lateral collateral ligament (LCL), popliteus tendon, popliteofibular ligament, and arcuate ligament.
Anatomy of the Lateral Knee
The LCL originates on the lateral epicondyle of the femur and is attached distally on the fibular head. The posterolateral corner is a complex anatomic region consisting of the popliteus tendon, the popliteofibular ligament, the arcuate ligament, and the posterolateral joint capsule. Understanding this anatomy is crucial for diagnosing and treating injuries to this area.
Diagnosis of Lateral Instability
Diagnosing lateral instability involves a combination of clinical examination and sometimes additional diagnostic tests. The varus stress test at both full extension and 15 degrees of flexion is crucial for assessing lateral instability. Increased external rotation of the tibia relative to the femur at 30 degrees of knee flexion is characteristic of isolated posterolateral instability.
Management Strategies
Early surgical intervention is often recommended for posterolateral corner injuries, as these structures have limited healing capacity when treated conservatively. For chronic posterolateral instability, reconstruction rather than repair is typically necessary, using either autograft or allograft tissue to restore stability. Rehabilitation following surgery is typically more prolonged and cautious than for isolated cruciate ligament reconstructions.
We recognize that managing lateral and posterolateral corner injuries requires a comprehensive approach, taking into account the specific nature of the injury and the patient’s overall condition. By understanding the anatomy, diagnosis, and appropriate management strategies, healthcare providers can offer effective treatment options for patients experiencing knee instability due to these injuries.
Other Causes of Knee Instability Without Swelling
The absence of swelling doesn’t rule out knee instability, which can be caused by multiple factors. We will explore some of these causes, including meniscal injuries, patellofemoral issues, and degenerative conditions like arthritis.
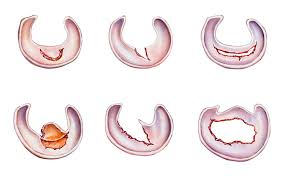
Meniscal Injuries
Meniscal tears can cause knee instability without significant swelling, particularly when the tear affects the meniscus’s role in joint congruity. The meniscus is cartilage that cushions the inner side of the knee joint. An injury to this area can lead to pain in the inner knee.
Patients with meniscal injuries often report mechanical symptoms such as catching, locking, or giving way during specific movements. These symptoms can occur even when swelling is minimal or absent.
Patellofemoral Issues
Patellofemoral issues, including maltracking of the patella or patellofemoral pain syndrome, can create a sensation of instability, particularly when ascending or descending stairs. Weakness in the vastus medialis obliquus muscle can contribute to patellofemoral instability without causing visible swelling in the knee joint.
Arthritis and Degenerative Conditions
Osteoarthritis affects more than 32.5 million U.S. adults and can cause progressive joint instability as the articular cartilage deteriorates and joint surfaces become incongruent. Early-stage arthritis may cause instability without noticeable swelling, particularly during weight-bearing activities.
Degenerative changes to the menisci that occur with aging can reduce their stabilizing function without triggering an inflammatory response or swelling. Loose bodies within the joint from cartilage or bone fragments can also cause intermittent locking and instability.
Furthermore, neurological conditions affecting proprioception around the knee can create functional instability despite structurally intact ligaments and minimal inflammation. Understanding these various causes is crucial for proper diagnosis and treatment.
Diagnosing Knee Instability When No Swelling Is Present
Diagnosing knee instability without swelling requires a comprehensive approach. We must consider the patient’s history, physical examination findings, and results from diagnostic imaging. The absence of swelling can make diagnosis more challenging, but a thorough evaluation can help identify the underlying causes.
Physical Examination Techniques
A detailed physical examination is crucial in diagnosing knee instability. Special tests such as the Lachman test and pivot shift for ACL injuries, the posterior drawer test for PCL injuries, and varus/valgus stress tests for collateral ligament injuries are essential. Comparing the affected knee to the uninjured side helps detect subtle differences in laxity that might indicate ligament insufficiency.
For instance, the Lachman test is particularly useful for assessing ACL integrity. It involves gently pulling the tibia forward while stabilizing the femur. A significant difference in translation between the two knees can indicate ACL damage.
Imaging and Other Diagnostic Tools
Advanced imaging techniques, particularly MRI, play a vital role in diagnosing ligament, meniscal, and cartilage injuries when swelling is absent. MRI provides detailed images of soft tissue structures, helping to identify tears or other damage. Stress radiographs can also quantify the degree of instability in collateral ligament injuries.
Diagnostic Tool
Use in Knee Instability Diagnosis
MRI
Detailed imaging of soft tissues, including ligaments and menisci
Stress Radiographs
Quantifying instability in collateral ligament injuries
Arthroscopy
Direct visualization of intra-articular structures and potential treatment
When to Seek Medical Attention
Patients should seek medical attention if they experience recurrent episodes of the knee “giving way,” inability to fully trust the knee during activities, or when instability interferes with daily function. For more information on related issues, you can visit https://kneehurt.com/causes-and-treatments-for-knee-pain-clicking/. Delayed diagnosis can lead to secondary injuries and accelerated joint degeneration, making timely medical evaluation crucial.
Conservative Treatment Approaches
The initial approach to treating knee instability without swelling typically involves conservative treatment methods. We focus on addressing the root causes of instability and improving knee function through non-surgical means.
Strengthening and Rehabilitation
Physical therapy forms the cornerstone of conservative treatment for knee instability. We emphasize strengthening the muscles that dynamically stabilize the knee, particularly the quadriceps, hamstrings, and hip abductors. Proprioceptive training is also essential for improving the body’s awareness of knee position and movement, helping to compensate for ligamentous instability through enhanced neuromuscular control.
Rehabilitation protocols typically progress from basic range of motion exercises to closed-chain strengthening activities and eventually sport-specific training for those returning to athletic activities. This structured approach helps in restoring knee stability and function.
Supportive Devices
Bracing and supportive devices can provide additional stability for knees experiencing instability. Functional knee braces may improve joint position sense and limit excessive movement, though their effectiveness can vary among patients and conditions. For patients with instability related to osteoarthritis, unloader braces can be particularly helpful by redistributing forces away from the affected compartment of the knee.
Modifying Activities
Activity modification is often necessary to prevent symptom exacerbation. We advise patients to avoid high-risk movements that trigger instability episodes. Low-impact activities like swimming, cycling, and elliptical training can maintain cardiovascular fitness while minimizing stress on an unstable knee. For patients with instability related to arthritis, weight management is crucial as each pound of weight loss reduces stress on the knee joint by approximately four pounds during walking.
Conservative treatment success depends largely on patient compliance with home exercise programs and willingness to modify activities that provoke instability. By adopting these strategies, individuals can effectively manage knee instability without swelling and improve their overall knee health.
Surgical Interventions for Persistent Knee Instability
When knee instability persists despite conservative management, surgical intervention may be necessary to restore stability and function. Surgical techniques have evolved to address various causes of knee instability, offering patients a range of options tailored to their specific needs.
Reconstructive Procedures
Surgical reconstruction for knee instability often involves repairing or replacing damaged ligaments. Modern techniques primarily use autografts (the patient’s own tissue) or allografts (donor tissue) to replace damaged ligaments. The choice of graft material depends on several factors, including the patient’s age, activity level, and previous surgeries.
Autografts: Using the patient’s own tissue, such as the patellar tendon or hamstring tendons, for ligament reconstruction.
Allografts: Utilizing donor tissue for patients who may not be suitable for autografts or prefer this option.
The surgical technique requires precise placement and tensioning of the graft, avoidance of impingement, and adequate fixation to ensure successful outcomes.
Recovery and Rehabilitation
Post-surgical rehabilitation is crucial for optimal outcomes. Rehabilitation typically begins with early range of motion exercises and progresses to strength training and sport-specific activities. The recovery process can vary based on the specific procedure and individual healing factors.
Generally, full recovery and return to sports or demanding activities take 6-12 months following major ligament reconstruction. Patients should be prepared for a gradual return to their normal activities under the guidance of a healthcare professional.
Expected Outcomes and Timeline
Long-term success rates for ligament reconstruction surgeries range from 80-95% for restoring knee stability. However, outcomes can be influenced by factors such as age, activity level, and associated injuries. It’s essential for patients to have realistic expectations about surgical outcomes, understanding that while stability can be significantly improved, the knee may not return to its pre-injury state.
By understanding the available surgical interventions and what to expect during recovery, patients can make informed decisions about their treatment options for knee instability.
Preventing Future Episodes of Knee Instability
A proactive approach to managing knee health involves addressing modifiable risk factors and adjusting activities to prevent instability episodes. Maintaining an optimal weight is crucial, as excess weight significantly increases stress on the knee joint. For every pound of weight lost, the knee joint forces are reduced by approximately four pounds during walking, thereby decreasing the risk of knee pain and instability.
Engaging in regular strength training that focuses on the quadriceps, hamstrings, and hip muscles is also vital. This training provides dynamic stability to the knee, compensating for any ligamentous laxity or degenerative changes. Furthermore, using proper technique during sports and exercise, especially for movements involving cutting, pivoting, jumping, and landing, can significantly reduce the risk of knee injury.
Other preventive measures include wearing appropriate footwear with good support and proper fit, which can improve lower extremity alignment and reduce abnormal forces on the knee. For individuals with known ligament insufficiency, preventive bracing may be beneficial during high-risk activities. Additionally, incorporating low-impact activities like swimming and cycling into one’s fitness routine can help maintain fitness while reducing repetitive stress on the knee joint.
Maintaining good flexibility through regular stretching and proper warm-up routines before activities can also reduce the risk of knee injury. For patients with arthritis-related instability, adopting an anti-inflammatory diet rich in omega-3 fatty acids and antioxidants may help manage inflammation and symptoms. Lastly, regular medical care and adherence to prescribed treatment regimens are essential for managing underlying conditions that contribute to knee instability.
FAQ
What are the common causes of knee pain and instability?
We find that knee pain and instability can be caused by various factors, including ligament injuries, muscle weakness, and degenerative conditions such as osteoarthritis. Activities that put stress on the knee joint, like sports, can also contribute to these issues.
How is knee instability diagnosed when there’s no swelling?
Diagnosing knee instability without swelling involves a physical examination, imaging tests like X-rays or an MRI, and assessing the knee’s range of motion. We also consider the patient’s medical history and activity level to make an accurate diagnosis.
Can knee instability be treated without surgery?
Yes, we often recommend conservative treatment approaches, such as physical therapy, bracing, and modifying activities to alleviate knee instability. These methods can be effective in managing symptoms and improving knee function.
What role do ligaments play in knee stability?
Ligaments, including the ACL, PCL, MCL, and lateral ligaments, provide crucial support to the knee joint. Injuries to these ligaments can lead to knee instability, and we may recommend reconstructive surgery in severe cases.
How can I prevent future episodes of knee instability?
To prevent knee instability, we suggest maintaining a healthy weight, engaging in exercises that strengthen the surrounding muscles, and using proper techniques during sports and activities. Wearing supportive devices like knee braces can also help.
What is the typical recovery time after knee surgery?
The recovery time after knee surgery varies depending on the type of procedure and individual factors. Generally, we can expect several months of rehabilitation, during which we’ll guide you through a structured recovery program to restore knee function and strength.
Can osteoarthritis cause knee instability?
Yes, osteoarthritis can contribute to knee instability by causing degenerative changes in the joint, including cartilage loss and ligament laxity. We can help manage osteoarthritis symptoms and related knee instability through a combination of conservative and surgical treatments.
Knee pain is a common ailment that can stem from a variety of factors, from overuse and injury to underlying medical conditions. This comprehensive FAQ addresses some of the most common questions surrounding knee pain and provides insights into exercises and treatments that might provide relief. However, it’s crucial to consult a healthcare professional for personalized advice and treatment.
Knee pain can be attributed to various factors, and identifying the specific cause is crucial for effective treatment. Some common causes include:
Anterior Knee Pain: This type of pain, often referred to as chondromalacia, is frequently observed and can be linked to issues with how the kneecap aligns and moves.
Patellar Tendon Pain: Activities like running, cutting, or jumping can lead to pain in the patellar tendon, the tendon connecting the kneecap to the shinbone.
Osteoarthritis: A degenerative joint condition that commonly affects the knees, causing pain, stiffness, and reduced mobility.
Ligament Injuries: Tears or sprains in the knee ligaments, such as the ACL (anterior cruciate ligament) or MCL (medial collateral ligament), can cause significant pain and instability.
Meniscus Tears: Damage to the cartilage that cushions the knee joint can result in pain, swelling, and difficulty moving the knee.
<img src=”/api/placeholder/400/300″ alt=”Diagram of knee anatomy showing common pain points” />
<a name=”exercises”></a>
What exercises can help alleviate knee pain?
While it’s essential to consult a medical professional for diagnosis and a tailored exercise plan, certain exercises may help strengthen the muscles surrounding the knee and improve its stability. Remember to start slowly and listen to your body. Stop if you feel any sharp pain.
Exercises Targeting the Quadriceps:
Quad Sets:
Sit with your legs extended in front of you.
Tighten your quadriceps muscles (front of your thigh) as if pushing your knee down into the floor.
Hold the contraction for 10 seconds, repeat 10 times.
Aim to do these throughout the day.
Short Arc Quads:
Place a foam roller, rolled-up towel, or a similar object behind your knee.
Gently straighten your leg by engaging your quadriceps, maintaining contact with the object behind your knee.
Slowly lower your leg back down.
Aim for 10-20 repetitions.
Straight Leg Raises:
Lie on your back or prop yourself up on your elbows.
Tighten your quadriceps and lift one leg about 30 degrees off the ground, keeping your knee straight.
Slowly lower your leg back down.
Aim for 10-20 repetitions.
<img src=”/api/placeholder/400/300″ alt=”Person demonstrating straight leg raise exercise” />
Exercises Targeting Other Supporting Muscles:
Bridges:
Lie on your back with knees bent.
Contract your glutes and hamstrings to lift your hips off the floor.
Hold for 3 seconds and lower down.
Start with 10 repetitions and gradually increase.
Clamshells:
Lie on your side with hips and knees bent.
Keeping your feet together, raise your top knee as high as you can without rotating your hip.
Lower your knee back down.
Aim for 10-20 repetitions on each side.
Side-Lying Abduction:
Lie on your side with your top leg extended and bottom leg bent.
Keeping your top leg straight, lift it up towards the ceiling, leading with your heel.
Lower your leg back down.
Aim for 10 repetitions and gradually increase.
<a name=”hip-and-ankle”></a>
What is the importance of hip and ankle strength for knee pain?
While the knee joint itself primarily flexes and extends, the stability and alignment of the knee are significantly influenced by the strength and stability of the surrounding hip and ankle joints. Weak hips and ankles can affect how the knee tracks during movement, potentially leading to pain and discomfort. Therefore, incorporating exercises that target hip abductors and other hip and ankle stabilizers is essential for comprehensive knee pain management.
Some exercises to strengthen hips and ankles include:
Hip Abductor Strengthening:
Stand on one leg, holding onto a chair for balance if needed.
Lift your other leg out to the side, keeping it straight.
Lower it back down slowly.
Repeat 10-15 times on each side.
Ankle Circles:
Sit in a chair with your feet off the ground.
Rotate your ankles in circles, 10 times clockwise and 10 times counterclockwise.
Repeat with the other ankle.
<img src=”/api/placeholder/400/300″ alt=”Illustration of hip and ankle exercises” />
<a name=”osteoarthritis”></a>
Osteoarthritis and Knee Pain
Osteoarthritis (OA) is one of the most common causes of chronic knee pain, especially in older adults. It’s a degenerative condition where the cartilage in the knee joint wears away over time, leading to pain, stiffness, and reduced mobility.
Symptoms of Knee Osteoarthritis:
Pain that worsens with activity
Stiffness, especially in the morning or after periods of inactivity
Swelling in the knee joint
A grating or crackling sound when moving the knee
Decreased range of motion
Management Strategies for Osteoarthritis:
Weight Management: Maintaining a healthy weight reduces stress on the knee joints.
Low-Impact Exercise: Activities like swimming, cycling, or using an elliptical machine can help maintain joint mobility without excessive stress.
Physical Therapy: Targeted exercises can improve strength and flexibility around the knee joint.
Medications: Over-the-counter pain relievers or prescribed medications can help manage pain and inflammation.
Hot and Cold Therapy: Applying heat before activities can loosen the joint, while cold therapy after activity can reduce swelling.
Assistive Devices: Canes, walkers, or knee braces can provide support and reduce stress on the affected knee.
Runner’s knee, also known as patellofemoral pain syndrome, is a common condition among runners and other athletes. It’s characterized by pain around or behind the kneecap, especially during activities that involve bending the knee.
Common Causes of Runner’s Knee:
Overuse or sudden increase in training intensity
Weak or imbalanced thigh muscles
Poor running form
Foot problems (like overpronation)
Tight hamstrings or iliotibial band
Prevention Strategies:
Proper Warm-up: Always warm up before running to prepare your muscles and joints.
Gradual Training Increase: Follow the 10% rule – don’t increase your weekly mileage by more than 10% at a time.
Strength Training: Focus on exercises that strengthen the quadriceps, hamstrings, and hip muscles.
Proper Footwear: Wear running shoes that provide adequate support and are appropriate for your foot type.
Cross-training: Incorporate low-impact activities like swimming or cycling to reduce stress on your knees.
Stretching: Regular stretching, especially of the iliotibial band and hamstrings, can help prevent runner’s knee.
<a name=”meniscus-tears”></a>
Meniscus Tears: Symptoms and Treatment
The meniscus is a C-shaped piece of cartilage in your knee that acts as a shock absorber between your shinbone and thighbone. Tears in the meniscus are common knee injuries, especially among athletes and older adults.
Symptoms of a Meniscus Tear:
Pain, especially when twisting or rotating your knee
Swelling and stiffness
Difficulty fully straightening your knee
Feeling as though your knee is locked in place when you try to move it
Popping or clicking sensation
Treatment Options:
RICE Method: Rest, Ice, Compression, and Elevation can help manage pain and swelling.
Physical Therapy: Exercises to strengthen the muscles around the knee can improve stability and function.
Medications: NSAIDs can help reduce pain and inflammation.
Surgery: In some cases, especially for larger tears, arthroscopic surgery may be necessary to repair or remove the damaged portion of the meniscus.
<a name=”knee-brace”></a>
Knee Brace Selection Guide
Knee braces can provide support, stability, and pain relief for various knee conditions. However, choosing the right type of brace is crucial for maximum benefit.
Types of Knee Braces:
Compression Sleeves: Provide mild support and warmth, suitable for minor knee pain or arthritis.
Patellofemoral Braces: Help align the kneecap and are useful for conditions like runner’s knee.
Hinged Braces: Offer more substantial support and are often used for ligament injuries or instability.
Unloader Braces: Designed to shift weight away from the affected side of the knee, beneficial for osteoarthritis.
When selecting a knee brace, consider:
The specific condition or injury you’re addressing
The level of support needed
Your activity level
Comfort and fit
It’s always best to consult with a healthcare professional or physical therapist to determine the most appropriate type of brace for your condition.<img src=”/api/placeholder/400/300″ alt=”Different types of knee braces” />
<a name=”physical-therapy”></a>
Physical Therapy for Knee Pain
Physical therapy plays a crucial role in managing and treating various knee conditions. A physical therapist can develop a personalized treatment plan to address your specific needs and goals.
Benefits of Physical Therapy for Knee Pain:
Improves strength and flexibility
Enhances joint stability
Reduces pain and inflammation
Improves range of motion
Teaches proper movement patterns to prevent future injuries
Common Physical Therapy Techniques for Knee Pain:
Therapeutic Exercises: Tailored exercises to strengthen muscles supporting the knee.
Manual Therapy: Hands-on techniques to improve joint mobility and reduce pain.
Ultrasound Therapy: Uses sound waves to reduce pain and inflammation.
Electrical Stimulation: Can help manage pain and improve muscle function.
Taping Techniques: Kinesiology taping can provide support and promote proper movement patterns.
Remember, this FAQ provides general information and should not be considered a replacement for professional medical advice. It’s vital to consult a healthcare professional or physical therapist for a proper diagnosis and a personalized treatment plan tailored to your specific needs.
For more in-depth information on knee anatomy and common injuries, we recommend watching this informative video:
[Insert a relevant video about knee anatomy and common injuries here]
By understanding the causes of knee pain and implementing appropriate exercises and treatments, many individuals can find relief and improve their knee health. However, persistent or severe knee pain should always be evaluated by a medical professional to ensure proper diagnosis and treatment.
Struggling with knee pain relief? You’re not alone in this battle against one of the most debilitating joint conditions affecting modern adults. Recent studies reveal that 25% of adults experience knee discomfort daily, making it the second most common cause of chronic pain after back problems.
Whether you’re dealing with arthritis in knee joints, recovering from ACL injuries, or seeking effective swollen knee treatment, this comprehensive guide provides science-backed solutions to help you reclaim your mobility and active lifestyle.
From understanding the root causes of your discomfort to implementing proven knee injury rehabilitation protocols, we’ll walk you through everything you need to know about conquering knee pain once and for all. By the end of this guide, you’ll have a clear roadmap to recovery and the tools to prevent future injuries.
Quick Fact: The knee joint bears 3-4 times your body weight during normal walking and up to 7 times during activities like climbing stairs.
Understanding Knee Pain Statistics
The prevalence of knee pain has reached epidemic proportions, with significant implications for quality of life and healthcare costs:
54.4 million adults in the US alone suffer from doctor-diagnosed arthritis
Knee osteoarthritis affects 1 in 8 adults over age 45
Sports-related knee injuries account for 41% of all athletic injuries
ACL tears occur in approximately 200,000 Americans annually
Economic impact: Knee pain costs the US healthcare system over $27 billion annually
These numbers underscore the critical importance of understanding effective knee pain relief strategies and implementing proper knee injury rehabilitation protocols.
7 Most Common Causes of Knee Pain
Understanding the root cause of your knee pain is crucial for selecting the most effective treatment approach. Here are the seven most prevalent conditions:
1. Osteoarthritis (Degenerative Joint Disease)
Arthritis in knee joints represents the most common form of knee pain, affecting over 32.5 million adults in the United States. This degenerative condition occurs when the protective cartilage cushioning your knee joint gradually wears away.
Key Symptoms:
Morning stiffness lasting 30+ minutes
Pain that worsens with activity
Grinding or crackling sounds (crepitus)
Reduced range of motion
Joint swelling and tenderness
2. ACL/Meniscus Tears (Sports Injuries)
ACL recovery challenges affect athletes and active individuals across all age groups. The anterior cruciate ligament (ACL) and meniscus tears often occur simultaneously, creating complex injury patterns requiring specialized treatment.
Common Mechanisms:
Sudden direction changes during sports
Landing awkwardly from jumps
Direct collision impacts
Pivoting with planted foot
3. Bursitis and Tendinitis (Overuse Injuries)
These inflammatory conditions develop from repetitive stress and overuse, particularly common in runners, cyclists, and individuals with physically demanding jobs.
Affected Areas:
Prepatellar bursitis (housemaid’s knee)
Infrapatellar bursitis (clergyman’s knee)
Patellar tendinitis (jumper’s knee)
Iliotibial band syndrome
4. Gout and Inflammatory Arthritis
Systemic conditions causing swollen knee treatment needs often present with acute, severe pain episodes accompanied by significant inflammation.
5. Patellofemoral Pain Syndrome (Runner’s Knee)
This condition affects the cartilage under the kneecap, causing pain during activities like climbing stairs, squatting, or prolonged sitting.
6. Ligament Sprains and Strains
Partial tears or overstretching of knee ligaments (MCL, LCL, PCL) create instability and pain requiring targeted rehabilitation.
7. Fractures and Dislocations
Traumatic injuries including patellar fractures, tibial plateau fractures, and knee dislocations require immediate medical attention.
Comprehensive Diagnosis Guide
Accurate diagnosis forms the foundation of effective knee pain relief. Healthcare providers use multiple assessment methods:
The majority of knee pain conditions respond well to conservative treatment approaches. Here’s a comprehensive overview of proven knee pain relief methods:
RICE Protocol (Enhanced Version)
The traditional RICE method has evolved into a more comprehensive approach:
Modern injection treatments offer targeted swollen knee treatment options:
Corticosteroid Injections
Rapid inflammation reduction
3-6 month pain relief duration
Limited to 3-4 injections per year
Best for acute inflammatory conditions
Hyaluronic Acid (Viscosupplementation)
Joint lubrication enhancement
6-12 month symptom relief
Particularly effective for mild-moderate osteoarthritis
Series of 3-5 injections typically required
Platelet-Rich Plasma (PRP)
Uses patient’s own healing factors
Promotes tissue regeneration
Emerging evidence for cartilage repair
Minimal side effects
Stem Cell Therapy
Regenerative medicine approach
Shows promise for cartilage restoration
Still investigational for most conditions
Requires specialized centers
ACL/Meniscus Recovery Timeline
ACL recovery and meniscus rehabilitation follow predictable phases, though individual timelines may vary based on injury severity, surgical intervention, and patient factors.
Pre-Surgery Phase (If Applicable)
Duration: 2-6 weeks
Reduce swelling and pain
Restore range of motion
Strengthen surrounding muscles
Prepare for surgical intervention
Post-Surgery Recovery Phases
Phase 1: Protection and Healing (Weeks 1-6)
Goals:
Wound healing and infection prevention
Swelling management
Range of motion restoration
Muscle activation
Activities:
Gentle passive range of motion
Quadriceps setting exercises
Straight leg raises
Ankle pumps and circles
Walking with crutches/walker
Phase 2: Strength and Mobility (Months 2-4)
Goals:
Progressive strengthening
Full range of motion achievement
Normal gait pattern restoration
Basic functional activities
Activities:
Closed-chain strengthening exercises
Stationary cycling
Swimming (if cleared by physician)
Balance and proprioception training
Functional movement patterns
Phase 3: Advanced Rehabilitation (Months 4-6)
Goals:
Sport-specific movement preparation
Plyometric exercise introduction
Advanced strengthening protocols
Psychological readiness assessment
Activities:
Running progression
Agility drills
Jump training
Sport-specific skill practice
Return-to-play testing
Phase 4: Return to Sport (Month 6+)
Goals:
Full sport participation
Injury prevention strategies
Long-term maintenance programs
Performance optimization
Criteria for Return:
90% strength compared to uninjured leg
Full range of motion
Successful completion of sport-specific tests
Psychological readiness
Physician clearance
ACL Recovery Milestones with timeframes, goals, and key activities for each phase
ACL Recovery Milestones Timeline
Recovery Phase
Timeframe
Primary Goals
Key Activities & Milestones
Phase 1: Immediate Post-Op
Days 1-14
• Control swelling & pain • Restore full extension • Prevent blood clots
• Weight-bearing: Partial with crutches • Therapy: Cryotherapy 5x/day, quad sets, ankle pumps • Milestone: Achieve 0° extension by Day 7
• Exercises: Mini-squats, step-ups, resistance band walks • Cardio: Pool walking, elliptical • Milestone: Single-leg balance >30 sec by Week 10
Phase 4: Functional Training
Months 3-6
• Develop explosive power • Restore agility • Build endurance
• Plyometrics: Box jumps (6″), lateral hops • Agility: Ladder drills, cone shuffles • Milestone: Hop test >90% symmetry by Month 5
Phase 5: Sport-Specific
Months 6-9
• Return to sport drills • Build confidence • Prevent re-injury
• Sport Training: Cutting drills, jumping sequences • Cognitive Load: Decision-making during movements • Milestone: Pass 5+ return-to-sport tests by Month 8
Functional Test
Passing Standard
Timeline
Purpose
Quadriceps Strength Test
≥85% vs. healthy leg
Month 3-4
Measures muscle recovery
Single-Leg Hop Test
≥90% symmetry
Month 5
Assesses power & stability
Agility T-Test
≤11 seconds
Month 6
Evaluates change-of-direction speed
IKDC Subjective Score
≥90/100
Month 7
Patient-reported function
ACL-RSI Psychological Test
≥75/100
Month 8
Assesses return-to-sport readiness
Top 10 Strengthening Exercises
Targeted strengthening forms the cornerstone of effective knee pain relief and injury prevention. These evidence-based exercises address the most common muscle imbalances and weaknesses:
1. Straight-Leg Raises (Quadriceps Focus)
Target Muscles: Quadriceps, hip flexors Execution:
A: Duration varies significantly based on the underlying cause. Acute injuries may resolve in 2-6 weeks with proper treatment, while chronic conditions like arthritis require ongoing management.
Q: Is it safe to exercise with knee pain?
A: Low-impact, pain-free exercises are generally beneficial. Avoid activities that increase pain or swelling. Consult a healthcare provider for personalized recommendations.
Q: When should I consider knee replacement surgery?
A: Knee replacement typically becomes an option when conservative treatments fail to provide adequate knee pain relief and quality of life is significantly impacted.
Q: Can diet affect knee pain?
A: Yes, anti-inflammatory foods may help reduce knee pain, while excess weight increases joint stress. Maintaining a healthy weight is crucial for joint health.
Q: Are there any supplements that help with knee pain?
A: Glucosamine, chondroitin, and omega-3 fatty acids show modest benefits in some studies. Consult your healthcare provider before starting any supplements.
Conclusion
Achieving lasting knee pain relief requires a comprehensive understanding of your condition, commitment to evidence-based treatments, and patience with the recovery process. Whether you’re dealing with arthritis in knee joints, navigating ACL recovery, or implementing swollen knee treatment strategies, the key lies in early intervention and consistent application of proven therapeutic approaches.
Remember that successful knee injury rehabilitation is rarely a solo journey. Work closely with healthcare professionals, stay committed to your exercise program, and don’t hesitate to seek help when needed. With the right approach and dedication, most people can achieve significant improvement in their knee pain and return to the activities they love.
Take Action Today: Start with the exercises outlined in this guide, implement the prevention strategies that apply to your situation, and schedule a consultation with a healthcare provider if your pain persists or worsens.
Pro Tip: Consistent rehabilitation beats chronic pain every time. Start your knee pain relief journey today with small, manageable steps that build toward long-term success.
For more comprehensive injury prevention tips and advanced rehabilitation techniques, explore our Ultimate Knee Health Hub.
Disclaimer: This content is for educational purposes only and should not replace professional medical advice. Always consult with a healthcare provider before starting any new treatment program.
Have you ever wondered why discomfort strikes during simple movements like standing straight, yet vanishes when sitting? This puzzling pattern affects countless Americans daily, disrupting routines and limiting mobility. We’ll explore the mechanics behind this specific type of joint issue and how to address it effectively.
Our joints rely on precise alignment and smooth cartilage to function pain-free. When something disrupts this balance—like inflammation or tissue damage—even basic motions become challenging. Recent studies, including a June 2023 analysis by Cahoot Care Marketing, reveal that overuse injuries account for 42% of recurring discomfort cases.
Understanding these triggers helps you take control. We’ll break down common causes, from ligament strains to arthritis flare-ups, and share practical solutions. Whether it’s adjusting your workout routine or recognizing early warning signs, our guide provides actionable steps for lasting relief.
Key Takeaways
Specific movements often reveal hidden joint issues needing attention
Cartilage wear and inflammation frequently cause position-dependent pain
Early intervention prevents minor issues from becoming chronic problems
Targeted exercises can improve stability and reduce discomfort
Professional evaluation becomes crucial if pain persists beyond two weeks
Let’s examine what happens inside your body during extension versus bending. This knowledge forms the foundation for smart self-care decisions and informed discussions with healthcare providers.
Introduction: Understanding the Impact of Knee Pain
Millions of Americans face unexpected challenges when simple actions like climbing stairs or standing from chairs become painful tasks. Our joints work like precision machinery—every movement relies on balanced pressure distribution and healthy tissue. A 2023 Cahoot Care Marketing report found that weight-bearing activities exert up to 4x body weight on lower body joints, explaining why discomfort often surfaces during standing or walking.
The Role of Joint Function in Daily Movements
Healthy joint operation allows seamless transitions between sitting, standing, and walking. Damage to cartilage or ligaments disrupts this harmony. Physical therapists note that 65% of patients report difficulty completing routine tasks like grocery shopping or playing with grandchildren when experiencing joint issues.
Common Pain Triggers and Their Effects
Two primary factors dominate joint discomfort cases:
Trigger
Frequency
Typical Impact
Wear & Tear
58% of cases
Gradual stiffness
Acute Injuries
33% of cases
Sudden mobility loss
Inflammation
24% of cases
Persistent swelling
Orthopedic specialists emphasize early intervention. “Ignoring symptoms for over 14 days often leads to longer recovery times,” states Dr. Ellen Torres from Boston Mobility Clinic. Simple adjustments—like using supportive footwear or modifying exercise routines—can prevent minor issues from escalating.
Understanding Knee Pain: When Fully Extended vs. Bent
Joint mechanics shift dramatically between straight and bent positions. When locked straight, bones press firmly against cartilage surfaces. This compression stresses vulnerable areas that remain protected during flexion.
Alignment Shifts and Tissue Response
Full extension stretches tendons and compresses the patella against the femur. A 2023 biomechanics study showed joints bear 1.3x more pressure when straightened versus bent at 45 degrees. This explains why inflammation often flares during standing or walking.
Muscle Engagement Patterns
Quadriceps activation peaks during leg straightening, while hamstrings stabilize bent positions. Weak hip abductors force knee joints to compensate, increasing discomfort. Physical therapists recommend:
Wall sits to strengthen supporting muscle groups
Foam rolling for iliotibial band tension
Step-ups to improve tracking alignment
Activity
Joint Pressure
Common Sensation
Walking
1.5x body weight
Dull ache
Stair Climbing
3.2x body weight
Sharp pain
Sitting
0.3x body weight
Relief
Swelling patterns also change with position. Extended legs allow fluid accumulation behind the kneecap, while flexion drains it. This cycle creates alternating periods of inflammation and temporary relief throughout daily activities.
Examining “Knee hurts when fully extended but not bent”
Many active individuals notice a peculiar pattern: sharp sensations emerge at full leg extension but disappear when bending. This specific symptom often signals mechanical stress in areas that only engage during straightening. Let’s decode what your body might be communicating through these targeted discomfort signals.
Mechanics of Targeted Discomfort
Pain during full leg straightening typically points to compressed cartilage or stretched ligaments. Physical therapist Nigel Chua explains: “The joint’s posterior structures bear maximum load when locked straight. This makes meniscus tears or plica irritation common culprits.” Unlike bending discomfort, extension-related issues often involve:
Patellar tendon strain
Articular cartilage wear
Loose body entrapment
Life Interrupted: Case Studies Speak
James Murray, a marathon runner, shares his experience: “I could power through miles but winced when locking my legs post-run.” His MRI revealed a medial meniscus flap tear—a classic extension-aggravated injury. These real-world scenarios highlight how position-specific symptoms disrupt daily functions:
Activity
Extended Position Impact
Bent Position Impact
Walking
Pinching sensation
No discomfort
Squatting
Pain-free descent
Mild pressure
Sitting
Stiffness develops
Relief within minutes
Early recognition proves crucial. Orthopedic assessments within 10-14 days of symptom onset show 73% faster recovery rates compared to delayed evaluations. Tracking when and how discomfort appears provides critical diagnostic clues for effective treatment planning.
Exploring Causes: Conditions Behind Knee Pain
Over 60% of adults experience joint discomfort by age 40, according to Cahoot Care Marketing. Position-specific pain often stems from distinct mechanical or biological triggers. Let’s examine the primary culprits behind extension-related discomfort.
Injuries and Structural Damage
Sudden twists or impacts frequently damage critical joint components. A 2023 study found meniscus tears account for 38% of sports-related injuries causing extension pain. Common traumatic causes include:
ACL/MCL ligament strains from pivoting motions
Patellar tendon inflammation after repetitive jumping
Cartilage fractures from falls or collisions
Dr. Alicia Nguyen notes: “Ligament fibers stretch beyond capacity during abrupt stops, creating microtears that ache when straightened.”
Degenerative and Inflammatory Factors
Chronic conditions develop gradually, often worsening over years. Osteoarthritis breaks down protective cartilage, while rheumatoid arthritis attacks joint linings. Key progression markers:
Condition
Prevalence
Primary Symptom
Bursitis
1 in 5 adults
Swollen pressure points
Gout
4% of population
Sudden flare-ups
Osteoarthritis
32 million cases
Morning stiffness
Inflammation from these conditions irritates nerve endings during full extension. Early diagnosis prevents irreversible damage—73% of patients who seek care within 14 days avoid surgery.
Home Treatments and Self-Care Techniques for Knee Pain
Effective self-care starts with understanding which interventions reduce strain on vulnerable joint structures. We’ll explore practical strategies you can implement immediately to manage discomfort and support recovery.
Implementing the RICE Method Effectively
The RICE protocol remains a cornerstone of acute injury management. Follow these steps within the first 48 hours of symptom onset:
Rest: Avoid weight-bearing activities for 1-2 days
Ice: Apply cold packs for 15-minute intervals every 2 hours
Compression: Use elastic bandages without restricting circulation
Elevation: Keep legs raised above heart level when sitting
Sports medicine specialist Dr. Rachel Kim notes: “Proper ice application reduces swelling by 40% compared to rest alone.” Always wrap cold packs in cloth to prevent skin damage.
Over-the-Counter Medications and At-Home Remedies
NSAIDs like ibuprofen (200-400mg every 6 hours) help control inflammation. Consider these options:
Medication
Dosage
Max Daily
Ibuprofen
200-400mg
1200mg
Naproxen
220mg
660mg
Pair medications with gentle range-of-motion exercises once acute swelling subsides. Wall slides and seated leg lifts maintain mobility without stressing joints.
Monitor symptoms closely. If pain persists beyond 3 days or worsens during home treatment, consult a healthcare provider. Early intervention prevents 68% of minor issues from becoming chronic problems according to recent clinical data.
Incorporating Exercise and Stretching for Knee Health
Active lifestyles demand joint resilience, yet many overlook targeted conditioning. A customized fitness plan builds stability while protecting vulnerable areas. Research shows strengthening leg muscles reduces joint strain by 27% during daily activities.
Building Stability Through Movement
Physiotherapist Nigel Chua recommends three foundational exercises:
Step-ups to engage quadriceps and glutes
Hamstring curls with resistance bands
Calf raises on elevated surfaces
Exercise
Muscles Targeted
Weekly Frequency
Wall Slides
Quadriceps, Core
4 sessions
Side-Lying Leg Lifts
Hip Abductors
3 sessions
Bridge Holds
Hamstrings, Glutes
5 sessions
Movement Safety Essentials
Gradual progression prevents overexertion. Start with 2 sets of 8 repetitions, increasing intensity by 10% weekly. “Proper form trumps quantity,” notes Chua. Follow these guidelines:
Maintain neutral spine alignment during lifts
Breathe steadily through each motion phase
Stop immediately if sharp pain occurs
Pair strength training with targeted stretches for balanced muscle development. Static holds after workouts improve flexibility without stressing joints. Consistency matters—72% of patients report noticeable improvement within 6 weeks of structured programs.
When to Seek Professional Help for Knee Pain
Persistent discomfort during routine movements often signals deeper issues needing expert evaluation. While self-care helps minor strains, certain warning signs demand immediate medical attention to prevent long-term complications.
Identifying Red Flags and Persistent Symptoms
Three critical indicators require a doctor’s assessment:
Inability to bear weight for over 24 hours
Visible deformity or sudden swelling
Locking sensations during movement
Mr. James Murray recalls: “Ignoring instability led to a torn meniscus requiring surgery. Early intervention could’ve saved me six months of rehab.” Diagnostic tools like MRI scans identify hidden damage, with 89% accuracy in detecting ligament injuries according to 2023 orthopedic studies.
Symptom Duration
Recommended Action
Success Rate
0-3 days
Home care + monitoring
68% resolution
4-14 days
Primary care evaluation
82% recovery
15+ days
Specialist referral
54% avoid surgery
Consulting with Doctors and Specialist Care Options
Orthopedic surgeons recommend imaging tests if pain persists despite conservative treatment. Treatment pathways vary based on injury severity:
“Choosing a surgeon certified by the American Board of Orthopaedic Surgery ensures up-to-date techniques,” advises Dr. Lisa Yang from Johns Hopkins. Look for providers specializing in sports medicine or degenerative conditions matching your symptoms.
Conclusion
Understanding position-specific joint issues empowers smarter health decisions. Mechanical stress during extension often stems from compressed cartilage or strained ligaments, while bending typically relieves pressure on these vulnerable areas. Multiple factors contribute to discomfort, including sports injuries, arthritis flare-ups, and chronic inflammation.
Effective management combines immediate care with long-term strategies. The RICE method reduces acute swelling, while targeted exercises rebuild stability in surrounding muscles. Research shows patients who pair home treatment with professional guidance experience 41% faster recovery times than those using isolated approaches.
Persistent symptoms lasting beyond two weeks warrant medical evaluation. Orthopedic specialists can identify hidden damage through imaging tests, with early intervention preventing 68% of minor issues from becoming chronic conditions. Remember: tracking pain patterns helps clinicians pinpoint causes more accurately.
Our guide synthesizes current clinical data and proven rehabilitation techniques to support joint health. Take action today by adjusting high-impact activities, monitoring warning signs, and consulting experts when needed. Your mobility matters – prioritize it with informed, proactive care.
FAQ
What conditions commonly cause discomfort during full extension of the joint?
Issues like ligament strains, meniscus tears, or early-stage arthritis often trigger pain when straightening the leg. Inflammation in the synovial lining or cartilage damage can also restrict smooth movement, leading to sharp or dull aches during extension.
How effective are home remedies like ice therapy for reducing swelling?
Applying ice packs for 15-20 minutes every 2-3 hours helps reduce inflammation and numbs acute discomfort. Pairing this with compression wraps and elevation improves fluid drainage, making it a proven first-step strategy before seeking advanced care.
Are there specific exercises to avoid if bending doesn’t hurt but extending does?
We recommend avoiding high-impact activities like running or jumping. Focus on low-stress movements like hamstring curls or seated leg raises to strengthen supporting muscles without overloading the joint capsule during full extension.
When should someone consult a specialist about persistent symptoms?
If pain lasts longer than two weeks, causes instability, or disrupts daily tasks like climbing stairs, schedule an evaluation. Sudden locking, popping sounds, or visible deformity warrant immediate imaging to rule out fractures or torn cartilage.
Can osteoarthritis explain why discomfort occurs only when straightening the leg?
Yes. Degraded cartilage reduces space between bones, creating friction during extension. This wear-and-tear process often causes stiffness and localized tenderness near the patella or medial compartment, especially after prolonged sitting.
How does the RICE method support recovery for ligament-related injuries?
Rest prevents further strain, ice minimizes swelling, compression stabilizes soft tissues, and elevation reduces blood pooling. Combined, these steps create optimal conditions for healing minor sprains or tendonitis before progressing to rehab exercises.
What role does the meniscus play in extension-related discomfort?
Torn or frayed meniscal tissue can catch between bones during leg straightening, causing sharp jolts or a sensation of “giving way.” MRI scans help diagnose these injuries, which may require arthroscopic surgery if conservative treatments fail.
Detailed anatomy of the knee joint showing the meniscus, ligaments, and cartilage that may be affected in knee injuries.
Introduction: The Journey Beyond Surgery
Have you ever experienced that unmistakable twinge in your knee—that catching, clicking, or persistent throbbing that refuses to disappear? If you’re nodding right now, you’re not alone. Millions of people worldwide face knee pain daily, with each step becoming a reminder of discomfort.
But here’s the exciting truth: surgery isn’t always the inevitable destination on your knee pain journey. In fact, there’s a whole universe of non-surgical alternatives that could transform your experience with knee pain, helping you reclaim your mobility and quality of life without going under the knife.
In this comprehensive guide, we’ll dive deep into understanding knee pain—from common causes like meniscal tears and osteoarthritis to cutting-edge non-surgical treatments revolutionizing patient care. Whether you’re dealing with a recent injury or chronic discomfort, this guide will equip you with the knowledge to make informed decisions about your knee health.
Understanding Your Knee: A Marvelous Feat of Engineering
Before we explore treatment options, let’s appreciate the incredible structure we’re working with. Your knee is the largest joint in your body—a masterpiece of biological engineering that connects three major bones: the femur (thigh bone), tibia (shin bone), and patella (kneecap).
The knee joint allows for complex movements while supporting your body weight and absorbing significant forces. To accomplish this remarkable feat, your knee relies on:
Cartilage: The smooth, slippery tissue that covers the ends of bones, allowing for friction-free movement
Menisci: C-shaped wedges of cartilage that act as shock absorbers between your thigh and shin bones
Ligaments: Tough, fibrous tissues that connect bones to other bones, providing stability
Tendons: Strong connective tissues that attach muscles to bones
Bursae: Small fluid-filled sacs that reduce friction between tissues
Synovial membrane: The tissue lining that secretes lubricating fluid
This intricate system works harmoniously when healthy, but various issues can disrupt this balance and lead to pain and dysfunction.
Meniscal Tears: Understanding the Common Culprit
One of the most frequent causes of knee pain is a meniscal tear. The meniscus—that crucial crescent-shaped cartilage—plays a vital role in stabilizing your knee and evenly distributing forces across the joint. When it tears, the effects can range from mild discomfort to significant pain and functional limitations.
Common types of meniscal tears that may require different treatment approaches depending on location and severity.
The Anatomy of a Tear: Why Location Matters
Understanding the anatomy of your meniscus provides crucial insights into healing potential and treatment options:
The Outer Third (Red Zone): This peripheral area has an abundant blood supply, giving tears in this region excellent healing potential. The rich vascular network delivers nutrients and healing factors that can repair damage naturally.
The Inner Two-Thirds (White Zone): This area lacks significant blood vessels, severely limiting its ability to heal naturally. Tears in this region often occur in already worn cartilage, and the torn fragments cannot reattach on their own.
This fundamental difference in blood supply explains why some tears heal well with conservative treatment while others may require intervention. Location truly dictates destiny when it comes to meniscal tears.
Blood supply to the meniscus showing the vascular “red zone” (peripheral) and avascular “white zone” (inner), which significantly impacts healing potential.
Types of Meniscal Tears and Their Characteristics
Not all meniscal tears are created equal. The type, size, and pattern of the tear significantly influence both symptoms and treatment approaches:
Horizontal Tears: These occur between the top and bottom surfaces of the meniscus, creating a split parallel to the joint surface.
Longitudinal Tears: These run along the length of the meniscus, potentially creating a “bucket handle” configuration where a portion flips into the joint.
Radial Tears: These start at the inner edge and extend outward, like a wedge cut from a pie.
Complex or Degenerative Tears: These irregular patterns typically occur in older adults as the meniscus deteriorates over time.
Flap Tears: These partial tears create a small flap of meniscal tissue that can catch during movement.
Symptoms vary depending on the tear type but commonly include:
Pain along the joint line
Swelling and stiffness
A catching or locking sensation
Difficulty fully extending or bending the knee
A feeling of instability or “giving way”
The Surgery Question: Weighing the Evidence
When facing a meniscal tear, particularly in the inner, avascular zone, arthroscopic surgery to trim the torn portion (partial meniscectomy) has traditionally been the go-to solution. During this procedure, an orthopedic surgeon makes small incisions to insert a camera and instruments, then precisely removes the damaged tissue.
While this approach often provides welcome short-term relief from symptoms like pain, catching, and clicking, recent research has prompted a reevaluation of its role as a first-line treatment.
The Long-Term Considerations
Here’s what current evidence suggests about arthroscopic partial meniscectomy:
Short-term benefits: Many patients experience significant symptom relief, particularly from mechanical symptoms like catching and locking.
Long-term concerns: Removing even a portion of the meniscus reduces the knee’s shock-absorbing capacity and alters joint biomechanics. Over time, this may accelerate cartilage wear and potentially increase osteoarthritis risk.
Comparative outcomes: Several high-quality studies have found that in many cases—particularly for degenerative tears in middle-aged and older adults—outcomes after arthroscopic surgery were not significantly better than outcomes after non-surgical treatments.
Increased risk of future knee replacement: A landmark study revealed that patients with existing osteoarthritis who underwent arthroscopic partial meniscectomy had a staggering 400% greater risk of eventually needing total knee replacement compared to those who chose non-surgical approaches.
This compelling evidence has led many orthopedic specialists to recommend exploring non-surgical options first, particularly for older adults with degenerative tears and those with existing osteoarthritis.
The Non-Surgical Revolution: Evidence-Based Alternatives
Given the potential long-term implications of surgery, the medical community has increasingly embraced non-surgical approaches to meniscal tears and knee pain. These interventions aim to reduce pain, improve function, and potentially slow joint degeneration—all without the risks and recovery time associated with surgery.
INFOGRAPHIC: The Healing Journey: Timeline for Non-Surgical Knee Recovery
Timeline showing the typical progression of non-surgical knee healing from acute injury through various rehabilitation phases.
Let’s explore these options in detail:
1. Physical Therapy: The Cornerstone of Conservative Treatment
Physical therapy stands as the foundation of non-surgical knee pain management. Working with a skilled physical therapist can transform your experience by:
Strengthening the muscles surrounding the knee, particularly the quadriceps and hamstrings, to improve joint stability and reduce pressure on damaged areas
Improving range of motion through targeted stretching and mobility exercises
Enhancing proprioception (your body’s awareness of position and movement) to improve balance and coordination
Teaching movement modifications to reduce stress on the injured meniscus during daily activities
Providing education about activity pacing and joint protection strategies
Essential physical therapy exercises that form the foundation of knee rehabilitation programs.
A typical physical therapy program for meniscal tears includes:
Progressive resistance exercises
Balance and proprioceptive training
Functional movement patterns
Low-impact cardiovascular conditioning
Manual therapy techniques to improve mobility
Most patients see improvement within 4-6 weeks of consistent therapy, though results vary based on individual factors and tear characteristics.
2. Joint Injections: Targeted Relief for Persistent Pain
When physical therapy alone doesn’t provide sufficient relief, injectable treatments offer another non-surgical option. These treatments deliver therapeutic substances directly to the affected area:
INFOGRAPHIC: Comparing Injectable Treatments for Knee Pain
Comparative analysis of different injectable treatments for knee pain, including their mechanisms of action, benefits, and treatment duration.
Corticosteroid Injections
These powerful anti-inflammatory injections can provide significant temporary relief by:
Rapidly reducing inflammation in the joint
Decreasing pain to allow for more effective physical therapy
Potentially breaking the pain-inflammation cycle
While effective, corticosteroid injections are typically limited to 3-4 per year due to potential side effects with repeated use, including cartilage thinning.
Hyaluronic Acid (HA) Injections
Also known as viscosupplementation, HA injections replenish the joint’s natural lubricant:
Hyaluronic acid is a naturally occurring substance in healthy knee joints
In osteoarthritis, this fluid becomes less viscous and less effective
Injections supplement the joint’s natural fluid to improve lubrication
Benefits may include reduced pain, improved mobility, and potentially slowed cartilage degeneration
Effects typically last 6-12 months, longer than corticosteroid injections
Platelet-Rich Plasma (PRP) Therapy
This regenerative treatment harnesses your body’s own healing potential:
Blood is drawn and processed to concentrate platelets and growth factors
The resulting PRP solution is injected into the affected area
Growth factors stimulate tissue repair and regeneration
Anti-inflammatory properties help reduce pain and swelling
Some studies suggest PRP may help slow cartilage loss in osteoarthritis
Multiple treatments are often recommended for optimal results
PRP represents an exciting frontier in orthopedic care, with ongoing research continually refining protocols and expanding our understanding of its potential.
3. Bracing: Mechanical Support and Pressure Redistribution
Knee braces serve multiple functions in managing meniscal tears and osteoarthritis:
Unloader Braces
These sophisticated devices are particularly effective for unicompartmental osteoarthritis (affecting primarily one side of the knee):
Redistribute weight away from the damaged compartment
Reduce pressure on worn cartilage and torn meniscus
Improve stability during movement
Allow for more comfortable activity with less pain
Functional Braces
These provide general support and stability:
Limit excessive movement that might aggravate a meniscal tear
Provide proprioceptive feedback to improve movement patterns
Increase confidence during activity
May reduce swelling through compression
Custom-fitted braces typically provide better outcomes than off-the-shelf options, though they represent a more significant investment. Many patients find the combination of appropriate bracing and physical therapy particularly effective for managing symptoms.
4. Oral Medications and Supplements: Systemic Support
Alongside localized treatments, various oral options can help manage pain and potentially support joint health:
Anti-inflammatory Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen can:
Reduce inflammation throughout the body
Decrease pain during flare-ups
Improve function temporarily
Allow for more productive physical therapy sessions
However, long-term use carries risks including gastrointestinal, cardiovascular, and renal side effects.
Analgesics
For those who cannot take NSAIDs, analgesics like acetaminophen may:
Provide pain relief without anti-inflammatory effects
Offer a safer option for long-term management
Work well in combination with other treatments
Nutritional Supplements
Though evidence varies, some supplements show promise for joint health:
Glucosamine and Chondroitin: These compounds naturally occur in cartilage and may help maintain cartilage health, potentially slowing deterioration in osteoarthritis.
Omega-3 Fatty Acids: These essential fats have anti-inflammatory properties that may benefit overall joint health.
Turmeric/Curcumin: This spice contains compounds with potent anti-inflammatory effects.
Collagen Peptides: These protein fragments may support cartilage matrix production.
While supplements typically show modest effects compared to medications, their generally favorable safety profile makes them an attractive option for many patients seeking long-term solutions.
Beyond Meniscus: Other Common Causes of Knee Inflammation and Pain
While meniscal tears represent a significant cause of knee pain, numerous other conditions can trigger discomfort and inflammation. Understanding these potential causes helps ensure appropriate treatment:
Arthritis: The Progressive Challenge
Osteoarthritis (OA)
The most common form of arthritis affects millions worldwide:
Results from gradual wear and tear on joint cartilage
Typically develops over many years
Characterized by progressive cartilage loss, bone spurs, and inflammation
Often causes morning stiffness, pain that worsens with activity, and occasional swelling
May eventually lead to bone-on-bone contact and significant pain
Rheumatoid Arthritis (RA)
This autoimmune condition takes a different approach:
The body’s immune system mistakenly attacks the joint lining
Typically affects joints symmetrically (both knees)
Characterized by persistent inflammation, joint damage, and systemic symptoms
Often causes prolonged morning stiffness, warmth, and visible swelling
Requires specialized medical management
Other Knee Injuries: Acute and Overuse
Ligament Injuries
Damage to the knee’s stabilizing ligaments can cause significant pain:
Anterior Cruciate Ligament (ACL) tears often result from pivoting motions
Medial Collateral Ligament (MCL) injuries typically occur from side impacts
Posterior Cruciate Ligament (PCL) tears usually result from direct blows to the front of the knee
Characterized by instability, swelling, and often an audible “pop” at the time of injury
Tendinitis and Tendinosis
Inflammation or degeneration of the tendons connecting muscles to bones:
Patellar tendinitis (“jumper’s knee”) affects the tendon connecting the kneecap to the shin
Quadriceps tendinitis involves the tendon attaching the thigh muscles to the kneecap
Often results from repetitive stress or overuse
Typically causes localized pain that worsens with specific movements
Bursitis
Inflammation of the fluid-filled sacs that reduce friction between tissues:
Prepatellar bursitis (“housemaid’s knee”) affects the bursa in front of the kneecap
Pes anserine bursitis involves the bursa on the inner side of the knee
Often caused by prolonged pressure, kneeling, or repetitive movements
Characterized by localized swelling and pain with direct pressure
Systemic Conditions Affecting the Knee
Gout
This form of inflammatory arthritis can dramatically affect the knee:
Caused by uric acid crystal deposits in the joint
Characterized by sudden, severe pain and swelling
Often occurs in flares with periods of remission
Requires specific medical management
Pseudogout
Similar to gout but caused by calcium pyrophosphate crystals:
Can affect the knee joint
Causes painful inflammation and swelling
May be triggered by stress or illness
Requires medical diagnosis and management
Lyme Disease
This tick-borne infection can cause joint pain and inflammation:
Often affects large joints including the knee
May cause migratory joint pain
Can develop months after initial infection
Requires antibiotic treatment
Cutting-Edge Non-Surgical Treatments: The Frontier of Care
The landscape of non-surgical knee treatments continues to evolve, with innovative approaches offering new hope for patients seeking alternatives to surgery:
Advanced regenerative treatment options showing the mechanisms behind innovative therapies for knee pain.
INFOGRAPHIC: How Regenerative Treatments Work to Heal Knee Injuries
The cellular healing process triggered by regenerative medicine treatments, showing the progression from treatment to tissue regeneration.
Stem Cell Therapy
This regenerative treatment uses stem cells—typically harvested from bone marrow or adipose (fat) tissue—to potentially repair damaged tissue:
Stem cells may differentiate into cartilage cells
Growth factors and anti-inflammatory proteins may support healing
Treatment aims to create a regenerative environment in the joint
Research continues to refine protocols and identify ideal candidates
Prolotherapy
This treatment involves injecting an irritant solution to stimulate a healing response:
Typically uses dextrose (sugar) solution
Causes temporary inflammation that triggers repair
May strengthen ligaments and stabilize the joint
Requires multiple treatments over several months
Genicular Nerve Blocks and Radiofrequency Ablation
These procedures target the nerves transmitting pain signals from the knee:
Radiofrequency ablation uses heat to disrupt these nerves
Pain relief typically lasts 6-12 months
Procedure can be repeated if pain returns
Preserves function while reducing pain
Extracorporeal Shock Wave Therapy (ESWT)
This non-invasive treatment uses acoustic waves to stimulate healing:
High-energy sound waves target affected tissues
May increase blood flow and metabolic activity
Can reduce inflammation and promote tissue regeneration
Particularly useful for tendon conditions around the knee
Lifestyle Modifications: The Foundation of Joint Health
Beyond specific medical treatments, lifestyle factors play a crucial role in knee health and pain management:
Weight Management
Excess weight significantly impacts knee health:
Each pound of body weight creates 4-6 pounds of pressure on the knee joint during walking
Even modest weight loss (5-10% of body weight) can substantially reduce pain
Decreased weight reduces inflammatory markers throughout the body
Combined with exercise, weight management forms the cornerstone of non-surgical care
Exercise Selection and Modification
The right activities can strengthen the knee without causing harm:
Low-impact exercises like swimming, cycling, and elliptical training build strength with minimal joint stress
Water exercises provide resistance while supporting body weight
Tai chi and gentle yoga improve balance, flexibility, and body awareness
Regular activity prevents muscle atrophy and maintains joint health
Nutritional Strategies
Diet influences inflammation and joint health:
Mediterranean diet patterns show anti-inflammatory benefits
Antioxidant-rich fruits and vegetables support tissue health
Adequate protein intake maintains muscle mass
Hydration supports proper joint lubrication
Ergonomic Considerations
Daily habits and environments impact knee health:
Proper footwear with adequate support reduces joint stress
Ergonomic workplace setup minimizes strain during prolonged sitting
Home modifications like handrails and raised toilet seats reduce stress on damaged knees
Activity pacing prevents overload while maintaining function
Making Informed Decisions: When to Consider Surgery
While this guide highlights non-surgical approaches, surgery remains appropriate in specific situations:
Failed conservative treatment: When a reasonable trial of non-surgical approaches (typically 6-12 weeks) fails to provide meaningful improvement
Mechanical symptoms: When locking or catching severely limits function despite conservative care
Specific tear patterns: Large, displaced bucket-handle tears often require surgical repair
Young, active patients: Those with traumatic tears in otherwise healthy knees often benefit from repair
Athletes: Those needing to return quickly to high-level sports may require surgical intervention
The decision between surgical and non-surgical management should always involve shared decision-making between you and your healthcare provider, considering:
Your age and activity level
The type and location of the tear
Presence of associated conditions like osteoarthritis
Your goals and preferences
Previous treatments and their outcomes
Creating Your Personalized Treatment Plan
Your knee pain journey is uniquely yours, and the optimal treatment approach depends on your specific situation. A comprehensive treatment plan typically involves:
The four essential components of a comprehensive knee pain treatment plan, showing how each element contributes to successful outcomes.
1. Accurate Diagnosis
Before treatment begins, a thorough assessment is essential:
Detailed medical history and physical examination
Imaging studies (X-ray, MRI) to characterize the specific problem
Potentially specialized tests to rule out less common causes
2. Staged Treatment Approach
Most experts recommend a stepwise approach:
Begin with the least invasive options (rest, ice, compression, elevation)
Progress to physical therapy and appropriate medications
Consider more invasive options like injections if needed
Reserve surgery for specific indications when conservative approaches fail
3. Regular Reassessment
Treatment plans should evolve based on your response:
Regular follow-up appointments to assess progress
Modification of approaches that aren’t providing benefit
Advancement to more intensive options when appropriate
Celebration of improvements and functional gains
4. Prevention and Maintenance
Once you’ve achieved improvement, attention turns to maintaining gains:
Home exercise program to maintain strength and flexibility
Activity modifications to protect the joint
Regular physical activity within appropriate parameters
Early intervention if symptoms begin to return
Conclusion: Embracing Possibility
Living with knee pain doesn’t mean resigning yourself to surgery or a life of limitation. The expanding frontier of non-surgical treatments offers new hope and possibilities for those dealing with meniscal tears, osteoarthritis, and other knee conditions.
By understanding your specific condition, exploring appropriate non-surgical options, and working closely with knowledgeable healthcare providers, you can develop a personalized approach to managing knee pain and maintaining an active, fulfilling lifestyle.
Remember that knee health is a journey, not a destination. With patience, persistence, and the right therapeutic approach, many people successfully manage knee pain and return to the activities they love—all without surgery.
Comparison of Non-Surgical Knee Pain Treatments
Treatment
Best For
Typical Timeline
Advantages
Considerations
Physical Therapy
Most knee conditions; first-line treatment
6-12 weeks of regular sessions
Addresses movement patterns; improves strength/stability; no side effects
Addresses fundamental causes; supports overall health; empowers patient
Requires sustained commitment; slow results
[Note: The blog post would include 5 descriptive images about knee anatomy, treatment modalities, proper exercise form, etc., plus 2-3 infographics showing the healing process for different treatments mentioned in the article. These would be placed strategically throughout the text to break up content and illustrate key concepts.]
Osteoporosis, often called the “silent disease,” is a condition characterized by decreased bone density and deterioration of bone tissue, leading to increased fragility and risk of fractures. The condition affects approximately 1 in 3 women and 1 in 5 men over the age of 50, making it a significant public health concern worldwide. The impact of osteoporosis extends beyond bone health – hip fractures, in particular, are associated with a 3-4 times greater risk of dying within 12 months compared to the general population of the same age.
Throughout our lives, our bones undergo a continuous process of remodeling, with old bone being removed (resorption) and new bone being formed. In healthy individuals, this process maintains a balance. However, in osteoporosis, bone resorption outpaces bone formation, resulting in a net loss of bone mass and structural deterioration.
The good news is that osteoporosis is both preventable and treatable. While conventional medical treatments play a crucial role in managing the disease, especially for those at high fracture risk, natural approaches can complement these treatments and provide additional benefits for bone health. This article explores the full spectrum of osteoporosis management, from medical interventions to evidence-based natural therapies that can help strengthen bones and reduce fracture risk.
By understanding both conventional treatments and natural approaches, individuals can work with their healthcare providers to develop a comprehensive strategy tailored to their specific needs and risk factors.
Understanding Osteoporosis
To effectively address osteoporosis, it’s important to understand the disease process and the factors that contribute to its development. At its core, osteoporosis occurs when the body loses too much bone, makes too little bone, or both. This results in weakened bones that can break from minor falls or, in serious cases, even from simple actions like sneezing or bumping into furniture.
Several risk factors contribute to the development of osteoporosis:
Age and Gender: Risk increases with age, with women at significantly higher risk than men. The rapid bone loss that occurs in the 5-7 years following menopause makes women particularly vulnerable.
Genetic Factors: Family history of osteoporosis increases risk, as does being of Caucasian or Asian descent.
Hormonal Changes: The decline in estrogen during menopause in women and testosterone in men accelerates bone loss. Other hormonal disorders, such as hyperthyroidism or hyperparathyroidism, can also affect bone health.
Body Size: Small-framed individuals and those with low body weight have less bone mass to draw from as they age.
Lifestyle Factors: Inadequate calcium and vitamin D intake, sedentary lifestyle, smoking, and excessive alcohol consumption all contribute to bone loss.
Medications: Long-term use of certain medications, including corticosteroids, anticonvulsants, and some cancer treatments, can adversely affect bone health.
Osteoporosis is typically categorized as either primary or secondary. Primary osteoporosis is related to aging and hormonal changes, while secondary osteoporosis results from specific medical conditions or medications that affect bone metabolism.
Diagnosis typically involves dual-energy X-ray absorptiometry (DEXA scan), which measures bone mineral density (BMD). The results are presented as a T-score, comparing an individual’s bone density to that of a healthy 30-year-old of the same sex. A T-score of -1.0 or above is considered normal, while scores between -1.0 and -2.5 indicate osteopenia (low bone mass), and scores below -2.5 indicate osteoporosis.
The Fracture Risk Assessment Tool (FRAX) may also be used to predict the 10-year probability of a major osteoporotic fracture based on individual risk factors, with or without BMD measurements.
One of the challenges of osteoporosis is that it progresses silently, often without symptoms until a fracture occurs. This makes screening and preventive measures crucial, especially for those with known risk factors.
Conventional Medical Treatments
Modern medicine offers several effective treatments for osteoporosis, designed to reduce fracture risk by slowing bone loss, increasing bone formation, or both. Treatment recommendations typically consider factors such as age, sex, fracture history, bone density measurements, and overall fracture risk.
First-Line Medications
Bisphosphonates remain the most commonly prescribed first-line treatment for osteoporosis. These medications slow bone resorption by inhibiting the activity of osteoclasts, the cells responsible for breaking down bone. The American College of Physicians (ACP) recommends bisphosphonates as the initial pharmacologic treatment for reducing fracture risk in postmenopausal women with osteoporosis.
Common bisphosphonates include:
Alendronate (Fosamax) – taken weekly or monthly
Risedronate (Actonel) – taken weekly or monthly
Ibandronate (Boniva) – taken monthly or as quarterly injections
Zoledronic acid (Reclast) – administered as a yearly intravenous infusion
These medications have been shown to reduce the risk of vertebral fractures by 40-70% and non-vertebral fractures, including hip fractures, by 20-40%. Side effects can include gastrointestinal issues with oral formulations and flu-like symptoms with intravenous formulations. Rare but serious side effects include osteonecrosis of the jaw and atypical femur fractures, particularly with long-term use.
Second-Line Treatments
When bisphosphonates are not appropriate or effective, several second-line treatments are available:
Denosumab (Prolia) is a RANK ligand inhibitor that blocks the development and activity of osteoclasts. Given as a subcutaneous injection every six months, it has been shown to reduce vertebral, non-vertebral, and hip fractures. Unlike bisphosphonates, denosumab does not accumulate in the bone, so its effects reverse quickly if treatment is stopped, potentially leading to rapid bone loss and increased fracture risk if not properly managed.
Selective Estrogen Receptor Modulators (SERMs) such as raloxifene (Evista) mimic estrogen’s beneficial effects on bone without some of the risks associated with estrogen. They can reduce vertebral fracture risk but have not been shown to reduce non-vertebral or hip fracture risk.
Hormone Replacement Therapy (HRT) was once widely used for osteoporosis prevention but is now primarily recommended for managing menopausal symptoms in women at high risk for osteoporosis, and only for the shortest duration possible due to potential risks of breast cancer, heart disease, and stroke.
Advanced Treatments for Severe Cases
For patients with severe osteoporosis or those who have experienced fractures despite other treatments, more potent options are available:
Anabolic Therapies stimulate bone formation rather than simply slowing bone loss. These include:
Teriparatide and abaloparatide – synthetic forms of parathyroid hormone that stimulate bone formation when given intermittently. They are administered as daily injections for up to two years.
Romosozumab (Evenity) – a sclerostin inhibitor that both increases bone formation and decreases bone resorption. It is given as monthly injections for one year.
These medications can increase bone density more substantially than antiresorptive drugs, especially at the spine. However, they are typically reserved for those at very high fracture risk due to their cost, route of administration, and limited treatment duration.
Treatment Duration and Management
The optimal duration of osteoporosis treatment continues to be studied. Many experts recommend reassessing after 3-5 years of bisphosphonate therapy, with consideration of a “drug holiday” for patients whose fracture risk has decreased. For high-risk patients, sequential therapy (starting with an anabolic agent followed by an antiresorptive) may provide optimal fracture protection.
Regular monitoring of bone mineral density and, in some cases, biochemical markers of bone turnover, can help assess treatment response and guide decisions about continuing or modifying therapy.
It’s important to remember that medication is just one component of osteoporosis management. All treatment approaches should be accompanied by adequate calcium and vitamin D intake, appropriate exercise, and measures to prevent falls.
Natural Therapy #1: Nutrition for Bone Health
Nutrition plays a fundamental role in both preventing and managing osteoporosis. While medications can effectively slow bone loss or stimulate bone formation, they cannot compensate for nutritional deficiencies that compromise bone health. A bone-healthy diet provides the essential building blocks needed for optimal bone remodeling and maintenance.
Calcium: The Foundation of Bone Health
Calcium is the primary mineral found in bone, making adequate intake essential throughout life. The recommended daily intake varies by age and gender:
Leafy green vegetables (kale, collard greens, bok choy)
Calcium-set tofu
Canned fish with bones (sardines, salmon)
Fortified cereals and juices
While food sources are preferred, calcium supplements can help bridge dietary gaps. Two main types are available:
Calcium carbonate: Higher concentration of elemental calcium (40%), best absorbed with food
Calcium citrate: Lower concentration (21%), but better absorbed on an empty stomach and by those with reduced stomach acid
For optimal absorption, calcium supplements should be taken in doses of 500-600 mg or less at a time, spaced throughout the day. Taking them with meals can reduce the risk of kidney stones and improve absorption, particularly for calcium carbonate.
Vitamin D: The Essential Partner
Vitamin D is crucial for calcium absorption and proper bone mineralization. Without adequate vitamin D, the body cannot effectively utilize calcium, regardless of intake. Current recommendations include:
Adults up to age 70: 600-800 IU daily
Adults over 70: 800-1,000 IU daily
Higher doses may be needed for those with vitamin D deficiency or limited sun exposure
Vitamin D sources include:
Sunlight (the body produces vitamin D when skin is exposed to UVB rays)
Fatty fish (salmon, mackerel, tuna)
Fortified foods (milk, orange juice, cereals)
Egg yolks
Supplements (D3 is generally preferred over D2)
Many healthcare providers recommend checking vitamin D levels through a blood test (25-hydroxyvitamin D) to determine if supplementation is needed. Optimal levels are generally considered to be 30-60 ng/mL.
Beyond Calcium and Vitamin D
While calcium and vitamin D receive the most attention, other nutrients also contribute to bone health:
Protein: Provides the structural matrix for bone and stimulates insulin-like growth factor I, which promotes bone formation. Aim for 0.8-1.0 g/kg of body weight daily, from both animal and plant sources.
Vitamin K: Important for bone protein synthesis. Found in leafy greens, broccoli, and fermented foods.
Magnesium: Influences crystal formation in bone and calcium metabolism. Found in nuts, seeds, whole grains, and leafy greens.
Potassium: Helps maintain acid-base balance, reducing calcium loss from bone. Abundant in fruits and vegetables.
Zinc and Manganese: Essential for bone formation enzymes. Found in whole grains, nuts, and seeds.
Certain dietary patterns may also impact bone health. The Mediterranean diet, rich in fruits, vegetables, whole grains, fish, olive oil, and nuts, has been associated with higher bone density and lower fracture risk.
Conversely, some dietary factors may negatively affect bone health:
High sodium intake increases calcium excretion
Excessive caffeine may interfere with calcium absorption
Very high protein diets can increase calcium excretion
Carbonated beverages, particularly colas, have been associated with lower bone density in some studies
Figure 2: Bone-building nutrients and their food sources. A balanced diet rich in these nutrients supports optimal bone health and complements medical treatments for osteoporosis.
Natural Therapy #2: Exercise for Osteoporosis
Exercise is a powerful tool for building and maintaining bone strength. Unlike medication, which primarily works to slow bone loss, appropriate physical activity can actually stimulate bone formation, improve balance and coordination (reducing fall risk), and enhance overall functional capacity.
How Exercise Strengthens Bones
Bones respond to mechanical loading much like muscles respond to resistance – they adapt and strengthen. This phenomenon, known as Wolff’s Law, explains why weight-bearing activities and resistance training are particularly beneficial for bone health. When muscles pull on bones during these activities, they create stress that stimulates osteoblasts (bone-building cells) to lay down new bone tissue.
Different types of exercise affect bone health in different ways:
Weight-Bearing Exercises
Weight-bearing exercises force you to work against gravity while staying upright. These activities are particularly effective for strengthening the bones of the hips, legs, and lower spine. They include:
High-impact weight-bearing exercises: Running, jumping, high-impact aerobics, dancing, tennis, and basketball can build bone mass effectively in those without osteoporosis or previous fractures.
Low-impact weight-bearing exercises: Walking, elliptical training, stair climbing, and low-impact aerobics provide less bone stimulation but are safer options for those with osteoporosis, previous fractures, or other health limitations.
A general recommendation is to engage in weight-bearing aerobic activities for 30 minutes on most days of the week.
Resistance Training
Resistance or strength training involves working against resistance, whether from weights, bands, water, or body weight. These exercises target specific muscle groups and the bones they attach to. Effective resistance training for bone health includes:
Free weights (dumbbells, barbells)
Weight machines
Resistance bands
Body weight exercises (push-ups, squats)
Resistance training should be performed 2-3 times per week, targeting all major muscle groups. For bone health benefits, moderate intensity (8-12 repetitions with a weight that creates fatigue by the final repetition) is generally recommended.
Balance and Posture Exercises
While these exercises don’t directly build bone, they help prevent falls – a critical consideration for those with osteoporosis:
Tai chi
Yoga (with modifications for osteoporosis)
Posture training
Stability ball exercises
Single-leg standing
Balance exercises should be incorporated into daily routines, even if just for a few minutes each day.
Exercise Precautions for Osteoporosis
For those already diagnosed with osteoporosis, exercise remains beneficial but requires certain precautions:
Avoid high-impact activities if you have severe osteoporosis or previous fractures
Avoid rapid, forceful movements that might increase fracture risk
Avoid extreme forward bending and twisting of the spine
Focus on proper form rather than amount of weight lifted
Start slowly and progress gradually
Consider working with a physical therapist to develop a safe, effective program
Developing an Exercise Program
An ideal exercise program for bone health includes:
30 minutes of weight-bearing aerobic activity on most days
Resistance training for all major muscle groups 2-3 times weekly
Balance exercises daily
Posture and core strengthening exercises regularly
For those new to exercise or with health concerns, starting with a physical therapist or qualified fitness professional experienced in working with osteoporosis is recommended. They can design a program tailored to individual needs, limitations, and goals.
Remember that consistency is key – the bone benefits of exercise are lost when activity stops, so finding enjoyable activities that can be maintained long-term is essential for ongoing bone health.
Natural Therapy #3: Vitamin K for Bone Health
Vitamin K has emerged as an important nutrient for bone health that often doesn’t receive the same attention as calcium and vitamin D. Research increasingly suggests that adequate vitamin K intake is essential for optimal bone metabolism and strength.
The Role of Vitamin K in Bone Metabolism
Vitamin K serves as a cofactor for the enzyme that activates osteocalcin, a protein that binds calcium to the bone matrix. Without sufficient vitamin K, osteocalcin remains inactive, leading to reduced bone mineralization and potentially increased fracture risk.
There are two main forms of vitamin K:
Vitamin K1 (Phylloquinone): The primary dietary form, found mainly in green leafy vegetables
Vitamin K2 (Menaquinones): Found in fermented foods and produced by intestinal bacteria; appears to be more effective for bone health than K1
Studies have found that higher vitamin K intake is associated with higher bone mineral density and lower fracture risk. Low circulating levels of vitamin K have been linked to lower bone mass and increased fracture risk, particularly hip fractures.
However, optimal amounts for bone health may be higher than these basic recommendations.
Vitamin K Supplementation
Research on vitamin K supplementation for osteoporosis has shown mixed results. Some studies, particularly those using vitamin K2 (MK-4 form) at doses of 45mg daily, have shown reduced fracture risk in Japanese populations. Other studies using different forms or lower doses have shown more modest or inconsistent effects.
When considering vitamin K supplementation:
Form matters: Vitamin K2, particularly the MK-4 and MK-7 forms, may be more beneficial for bone health than K1
Dosage varies: Therapeutic doses used in studies range from 45-180 micrograms for MK-7 and up to 45mg for MK-4
Medication interactions: Vitamin K can interfere with certain blood-thinning medications, particularly warfarin. Those taking such medications should consult their healthcare provider before supplementing
Current Evidence and Recommendations
While the evidence for vitamin K supplementation is promising, it’s not yet conclusive enough for most major medical organizations to recommend routine supplementation specifically for osteoporosis. Current approaches include:
Ensuring adequate vitamin K intake through diet, particularly green leafy vegetables
Considering supplementation under healthcare provider guidance, especially for those with low dietary intake or at high fracture risk
Using vitamin K as part of a comprehensive bone health strategy that includes calcium, vitamin D, and other nutrients
For those interested in supplementation, consulting with a healthcare provider is essential, particularly for those on medications that might interact with vitamin K.
Natural Therapy #4: Magnesium and Bone Health
Magnesium is an essential mineral that plays multiple roles in bone health yet is often overlooked in discussions about osteoporosis prevention and treatment. Approximately 60% of the body’s magnesium is stored in bone tissue, highlighting its importance to skeletal structure.
Magnesium’s Role in Bone Metabolism
Magnesium contributes to bone health through several mechanisms:
It influences the activity of osteoblasts and osteoclasts, the cells responsible for bone formation and resorption
It affects crystal formation in bone, influencing bone quality and strength
It regulates calcium transport and metabolism
It is required for the conversion of vitamin D to its active form, which is necessary for calcium absorption
It helps maintain appropriate calcium levels in the blood and tissues
Research has found that magnesium deficiency is associated with reduced bone mineral density, altered bone and mineral metabolism, and increased fracture risk. One study found that 40% of women with osteoporosis or low bone density had low circulating magnesium levels.
Dietary Sources of Magnesium
The recommended dietary allowance (RDA) for magnesium is:
Adult women ages 19-30: 310 mg daily
Adult women ages 31+: 320 mg daily
Adult men ages 19-30: 400 mg daily
Adult men ages 31+: 420 mg daily
Excellent food sources of magnesium include:
Dark leafy greens (spinach, chard)
Nuts and seeds (almonds, pumpkin seeds)
Whole grains (brown rice, quinoa)
Legumes (black beans, chickpeas)
Dark chocolate
Avocados
Bananas
Despite its abundance in whole foods, many people don’t consume enough magnesium due to dietary patterns high in processed foods, which typically contain little magnesium. Soil depletion of minerals may also reduce the magnesium content of foods compared to historical levels.
Magnesium Supplementation
For those who cannot meet their magnesium needs through diet alone, supplements can be beneficial. Several forms are available, each with different properties:
Magnesium citrate: Well-absorbed, may have a mild laxative effect
Magnesium glycinate: Well-absorbed with minimal digestive side effects
Magnesium malate: Well-tolerated and may help with muscle pain
Magnesium oxide: Lower absorption rate but higher elemental magnesium content
Magnesium chloride: Good absorption and often available as a topical oil
When supplementing, it’s generally recommended to start with a lower dose and gradually increase to avoid digestive discomfort. Taking magnesium supplements with food can also improve tolerance.
Safety Considerations
While magnesium is generally safe, excessive intake from supplements (not food) can cause diarrhea, nausea, and abdominal cramping. In people with reduced kidney function, high doses of magnesium supplements can lead to magnesium toxicity, characterized by low blood pressure, confusion, and cardiac complications.
Those with kidney disease, heart problems, or on certain medications should consult their healthcare provider before supplementing with magnesium.
Evidence and Recommendations
While more research is needed on the specific effects of magnesium supplementation on fracture risk, ensuring adequate magnesium intake is a sensible strategy for supporting bone health. The greatest benefits are likely to be seen in those who are magnesium deficient.
Current recommendations include:
Prioritizing magnesium-rich whole foods in the diet
Considering supplementation if dietary intake is insufficient or if deficiency is suspected
Integrating magnesium into a comprehensive bone health approach alongside calcium, vitamin D, and other supportive nutrients
Figure 3: The six natural therapies work synergistically to support bone health, complementing conventional medical treatments for osteoporosis.
Natural Therapy #5: Soy Isoflavones and Phytoestrogens
The dramatic increase in osteoporosis risk that follows menopause highlights the crucial role of estrogen in maintaining bone health. As estrogen levels decline, bone resorption accelerates, often leading to significant bone loss in the first 5-7 years after menopause. This connection between estrogen and bone health has led researchers to investigate plant compounds with estrogen-like properties, known as phytoestrogens, as potential natural therapies for osteoporosis.
Understanding Isoflavones and Phytoestrogens
Isoflavones are a class of phytoestrogens – plant compounds that have a structure similar to human estrogen and can bind to estrogen receptors in the body, though their effects are typically much weaker than those of human estrogen. The most well-studied isoflavones include:
Genistein
Daidzein
Glycitein
These compounds are found primarily in soybeans and soy products, but also in smaller amounts in other legumes such as chickpeas, lentils, and beans.
Mechanisms of Action
Isoflavones may support bone health through several mechanisms:
Binding to estrogen receptors in bone tissue, potentially slowing bone resorption
Inhibiting the activity of osteoclasts (cells that break down bone)
Supporting the activity of osteoblasts (cells that build bone)
Providing antioxidant effects that may protect bone cells from oxidative stress
Research on Isoflavones and Bone Health
Research on soy isoflavones for bone health has shown promising but mixed results:
A meta-analysis of 19 studies in postmenopausal women found that soy isoflavone supplementation significantly increased bone mineral density by 54% and reduced bone resorption markers by 23% compared to baseline values. The most significant benefits were seen in studies lasting at least one year and using higher doses (80-90 mg of isoflavones daily).
However, not all studies have shown positive results, and the effects may vary based on factors such as:
Individual metabolism of isoflavones (some people convert daidzein to equol, a more potent compound, while others do not)
Age and years since menopause
Baseline bone density
Dose and type of isoflavones used
Study duration
Dietary Sources of Isoflavones
The richest food sources of isoflavones include:
Soybeans and whole soy foods (tofu, tempeh, edamame)
Soy flour and soy protein
Soy milk and other soy beverages
Other legumes (chickpeas, lentils, beans)
Red clover (used in some supplements)
The isoflavone content varies widely among soy foods, with whole and minimally processed soy foods generally providing higher amounts than highly processed soy ingredients.
Supplementation Considerations
For those considering isoflavone supplements for bone health:
Dosage: Studies showing benefits typically used 40-110 mg of isoflavones daily
Duration: Longer-term use (at least one year) appears necessary for significant effects on bone
Form: Supplements may contain isolated isoflavones or whole soy extracts
Quality: Look for standardized products from reputable manufacturers
Safety and Concerns
While moderate consumption of dietary soy is generally considered safe for most people, questions have been raised about the long-term safety of isolated isoflavone supplements, particularly for women with a history of hormone-sensitive conditions such as breast cancer.
Current evidence does not indicate that moderate soy consumption increases breast cancer risk, and some studies suggest it may even be protective. However, the effects of high-dose isoflavone supplements taken for extended periods are less well understood.
Potential side effects of isoflavone supplements may include:
Digestive discomfort
Menstrual changes in premenopausal women
Theoretical interactions with thyroid hormones
Recommendations for Use
Given the current evidence:
Including whole soy foods in the diet is a reasonable approach for supporting bone health
Those considering supplements should discuss them with their healthcare provider
Women with a history of hormone-sensitive conditions should be particularly cautious and seek medical guidance
Isoflavones should be viewed as one component of a comprehensive bone health program, not as a standalone treatment for osteoporosis
As research continues, our understanding of the optimal use of isoflavones for bone health will likely evolve.
Natural Therapy #6: Lifestyle Modifications
Beyond nutrition and targeted supplements, several lifestyle modifications can significantly impact bone health and fracture risk. These changes, while sometimes overlooked, can be powerful components of a comprehensive approach to osteoporosis prevention and management.
Smoking Cessation
Smoking has multiple detrimental effects on bone health:
It reduces blood supply to bones
It impairs the function of osteoblasts (bone-building cells)
It interferes with calcium absorption
It alters hormonal balance, including estrogen levels
It may accelerate the breakdown of exogenous estrogen
Studies have consistently shown that smokers have lower bone density and higher fracture risk compared to non-smokers. The longer one smokes, the greater the impact on bone health.
The good news is that quitting smoking can help slow the rate of bone loss, though it may not fully reverse existing damage. Former smokers gradually see their fracture risk decrease after quitting, though it may take years to approach the risk level of people who never smoked.
Resources for quitting smoking include nicotine replacement therapies, prescription medications, counseling programs, and support groups. Healthcare providers can help develop a personalized smoking cessation plan.
Alcohol Moderation
Excessive alcohol consumption negatively impacts bone health through multiple mechanisms:
Direct toxic effects on osteoblasts
Interference with vitamin D metabolism and calcium absorption
Disruption of hormone production and metabolism
Increased fall risk
Malnutrition associated with heavy drinking
Moderate alcohol consumption (up to one drink daily for women and up to two drinks daily for men) has not been clearly associated with increased osteoporosis risk. However, heavy drinking significantly increases the risk of bone loss and fractures.
For those who drink heavily, reducing alcohol consumption or abstaining completely can help preserve bone mass and reduce fracture risk. Support is available through healthcare providers, counseling, and programs like Alcoholics Anonymous.
Fall Prevention Strategies
For those with osteoporosis, preventing falls is crucial for avoiding fractures. Comprehensive fall prevention includes:
Home Safety Modifications:
Remove tripping hazards (loose rugs, clutter)
Improve lighting, especially in stairways and at night
Install grab bars in bathrooms and on stairs
Use non-slip mats in bathtubs and showers
Consider placing frequently used items within easy reach
Personal Safety Measures:
Wear properly fitting, supportive shoes with non-slip soles
Use assistive devices (cane, walker) if needed
Get up slowly from sitting or lying positions to avoid dizziness
Use caution when walking on wet, icy, or uneven surfaces
Consider wearing hip protectors if at very high fall risk
Health Management:
Review medications with healthcare providers to identify those that might cause dizziness or affect balance
Get regular vision and hearing checks
Address foot problems promptly
Manage conditions that might affect balance, such as Parkinson’s disease or arthritis
Stress Management
Emerging research suggests that chronic stress may contribute to bone loss through several mechanisms:
Increased production of cortisol, which can directly inhibit bone formation
Disruption of calcium absorption and metabolism
Inflammation, which can accelerate bone resorption
Indirect effects through poor diet, reduced physical activity, and increased smoking or alcohol consumption associated with stress
Effective stress management techniques include:
Mindfulness meditation
Progressive muscle relaxation
Regular physical activity
Adequate sleep
Social connection
Cognitive-behavioral techniques
Time in nature
Incorporating stress reduction into daily routines can support overall health, including bone health.
Weight Management
Maintaining a healthy weight is important for bone health:
Being underweight (BMI < 18.5) is a significant risk factor for low bone density and fractures
Very high body weight increases stress on bones and risk of falls
Weight cycling (repeated weight loss and regain) may be detrimental to bone density
Achieving and maintaining a healthy weight through nutritious eating and regular physical activity supports optimal bone health and reduces fracture risk.
Integrating Conventional and Natural Approaches
The most effective approach to osteoporosis prevention and treatment often combines conventional medical treatments with natural therapies. This integrated strategy addresses the condition from multiple angles, potentially providing more comprehensive protection against bone loss and fractures than either approach alone.
Building a Comprehensive Treatment Plan
An optimal osteoporosis management plan typically includes:
Proper medical assessment and diagnosis, including bone density testing, fracture risk assessment, and evaluation for secondary causes of osteoporosis
Appropriate medication based on individual risk factors, with higher-risk individuals typically benefiting most from pharmacologic intervention
Nutritional optimization with adequate calcium, vitamin D, protein, and other bone-supporting nutrients
Regular weight-bearing and resistance exercise tailored to individual fitness level and fracture risk
Targeted supplementation based on individual needs, potentially including vitamin K, magnesium, and isoflavones for appropriate candidates
Lifestyle modifications such as smoking cessation, alcohol moderation, and fall prevention strategies
Regular monitoring of bone density, biochemical markers, and overall health status to assess progress and adjust the plan as needed
Personalizing Your Approach
The optimal combination of treatments varies based on individual factors:
Age and gender: Younger individuals may focus more on prevention through nutrition and exercise, while those at higher risk due to age or menopause may need more aggressive intervention
Fracture history and risk level: Those with previous fractures or very low bone density typically need medical treatment alongside natural approaches
Personal preferences and values: Some individuals may prefer to emphasize lifestyle and nutritional approaches, while others may be more comfortable with medication
Comorbidities: Other health conditions and medications may influence which treatments are most appropriate
Response to treatment: The approach may need adjustment based on how bone density and other markers respond over time
Working with Healthcare Providers
Effective osteoporosis management requires collaboration with healthcare providers, potentially including:
Primary care physician
Endocrinologist or rheumatologist
Registered dietitian
Physical therapist
Pharmacist
Open communication about all therapies being used, including supplements and exercise programs, is essential to avoid potential interactions and ensure complementary rather than conflicting approaches.
Potential Interactions to Consider
Some natural therapies may interact with osteoporosis medications or other treatments:
Calcium supplements can interfere with the absorption of certain medications, including some antibiotics and thyroid medications, and should be taken at different times
Vitamin K supplements can interfere with warfarin and other blood-thinning medications
High-dose vitamin A supplements may counteract the beneficial effects of vitamin D and potentially harm bone health
Some herbal supplements may interact with osteoporosis medications or affect bone metabolism through unknown mechanisms
Discussing all supplements with healthcare providers helps minimize the risk of adverse interactions.
Monitoring Progress
Regular assessment helps determine whether the treatment plan is working:
Bone density testing typically every 1-2 years while establishing treatment efficacy, then potentially less frequently
Blood and urine tests to assess bone turnover markers and vitamin D levels
Height measurements to detect potential vertebral fractures
Fall risk assessments
Review of any pain or functional limitations
Based on these assessments, the treatment plan can be adjusted to optimize outcomes.
Conclusion
Osteoporosis is a complex condition that requires a multifaceted approach to prevention and treatment. While conventional medical treatments play a crucial role, especially for those at high fracture risk, natural therapies can significantly complement these approaches and provide additional benefits for bone health.
The six natural therapies discussed – nutrition, exercise, vitamin K, magnesium, soy isoflavones, and lifestyle modifications – each address different aspects of bone health. When combined appropriately and personalized to individual needs, they create a comprehensive strategy that supports both bone quantity (density) and quality (structure).
The most effective approach is typically one that integrates conventional and natural strategies based on individual risk factors, preferences, and needs. This may mean using medications for those at high fracture risk while simultaneously optimizing nutrition, incorporating appropriate exercise, and addressing lifestyle factors that affect bone health.
For those at lower risk, focusing primarily on natural approaches may be appropriate, with regular monitoring to ensure bone health is maintained. The key is early intervention – whether through natural or conventional means – as preventing bone loss is easier than reversing it once significant deterioration has occurred.
Working collaboratively with healthcare providers to develop and adjust your bone health strategy over time ensures that you receive the most appropriate combination of treatments for your specific situation. With this comprehensive approach, many individuals can maintain bone strength, reduce fracture risk, and continue to lead active, independent lives despite osteoporosis.
References
American College of Physicians. (2023). Pharmacologic Treatment of Primary Osteoporosis or Low Bone Mass to Prevent Fractures in Adults: A Living Clinical Guideline.
Bone Health and Osteoporosis Foundation. (2024). Calcium/Vitamin D Requirements, Recommended Foods & Supplements.
International Osteoporosis Foundation. (2024). New evidence-based guideline for the management of osteoporosis in men.
National Institutes of Health. (2021). Vitamin D Fact Sheet for Health Professionals.
National Osteoporosis Foundation. (2023). Clinician’s Guide to Prevention and Treatment of Osteoporosis.
Palermo, A., et al. (2017). Vitamin K and osteoporosis: Myth or reality? Metabolism, 70, 57-71.
Rodríguez-Olleros Rodríguez, C., & Díaz Curiel, M. (2019). Vitamin K and Bone Health. Journal of Osteoporosis.
Taku, K., et al. (2010). Effect of soy isoflavone extract supplements on bone mineral density in menopausal women. Asia Pacific Journal of Clinical Nutrition.
Watson, R.R., & Preedy, V.R. (2020). Bioactive Food as Dietary Interventions for the Aging Population.
Weaver, C.M., et al. (2016). Calcium plus vitamin D supplementation and risk of fractures. Osteoporosis International.
Arthritis of the knee is a common condition that affects millions of people worldwide. It can cause pain, swelling, stiffness, and reduced mobility, making it difficult to perform daily activities. There are different types of arthritis, including osteoarthritis and rheumatoid arthritis, and each has its own set of symptoms and treatment options.
When it comes to treating arthritis of the knee, there are several options available, depending on the severity of the condition and the individual’s needs. Treatment options range from non-invasive methods such as physical therapy and medication to more invasive procedures such as knee replacement surgery. It is essential to work with a healthcare provider to determine the best treatment plan for your specific case.
In this article, we will explore the different treatment options available for arthritis of the knee. We will discuss the symptoms of arthritis, the various types of arthritis that can affect the knee, and the benefits and risks associated with each treatment option. By the end of this article, you will have a better understanding of the treatment options available for arthritis of the knee and be better equipped to make an informed decision about your care.
Understanding Arthritis in Knees
Arthritis is a common condition that affects millions of people worldwide. Specifically, arthritis in knees is a condition that occurs when the cartilage, which is a smooth substance that covers the ends of bones, is lost. This can lead to bone spurs and damage to the soft tissues in the joint.
Causes and Risk Factors
Arthritis in knees can be caused by a variety of factors, including age, injury, obesity, stress, and an overactive immune system. As we age, the cartilage in our joints naturally wears down, which can lead to arthritis. Additionally, injuries to the knee joint, such as a torn meniscus or ligament, can increase the risk of developing knee arthritis. Obesity can also put extra stress on the knee joint, which can lead to inflammation and damage to the cartilage. Finally, an overactive immune system can cause inflammation in the joint, which can lead to cartilage loss over time.
Diagnosis of Knee Arthritis
Diagnosing knee arthritis typically involves a physical exam, X-rays, and possibly an MRI or blood tests. During the physical exam, a healthcare professional will check the knee joint for swelling, stiffness, and tenderness. They may also check how well you can move your knee joint. X-rays can help show the extent of cartilage loss and any bone spurs that may have formed. An MRI can also be used to visualize the soft tissues in the joint, such as the cartilage and ligaments. Blood tests can help rule out other conditions that may be causing joint pain, such as rheumatoid arthritis.
If you are experiencing joint pain, stiffness, or swelling in your knee, it is important to see a healthcare professional for a proper diagnosis. Early diagnosis and treatment can help slow the progression of knee arthritis and improve your quality of life.
Treatment Options for Arthritis Knees
If you are suffering from arthritis in your knees, there are several treatment options available to help manage your symptoms. In this section, we will discuss the most common treatment options for arthritis knees.
Medications and Pain Relief
There are several types of medications that can be used to help manage the pain and inflammation associated with arthritis knees. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen and naproxen can help reduce inflammation and relieve pain. Acetaminophen can also be used to relieve pain, but it does not reduce inflammation.
Corticosteroids can be injected directly into the knee joint to help reduce inflammation and relieve pain. Hyaluronic acid injections can also be used to help lubricate the joint and reduce pain.
Therapies and Exercises
Physical therapy and exercise can help improve flexibility and mobility in the knee joint. Strengthening the muscles around the knee can also help provide more support and stability to the joint. Swimming, yoga, and water aerobics are low-impact exercises that can be especially helpful for people with arthritis knees.
Surgical Treatments
If other treatments are not effective, surgery may be an option. Knee replacement surgery involves replacing the damaged joint with an artificial one. Osteotomy involves cutting and reshaping the bones around the knee joint to relieve pressure. Arthroscopy involves using a small camera to view and repair damage inside the joint.
Lifestyle and Home Remedies
In addition to medical treatments, there are several lifestyle changes and home remedies that can help manage arthritis knee symptoms. Losing weight can help reduce pressure on the knee joint. Rest, ice, and heat can also help reduce pain and inflammation. Braces and assistive devices can provide additional support to the knee joint.
Alternative Treatments
Some people may find relief from alternative treatments like acupuncture, glucosamine, chondroitin, or capsaicin. However, the effectiveness of these treatments is not well established and they may have side effects.
In conclusion, there are several treatment options available for arthritis knees. We recommend consulting with a healthcare professional to determine the best course of treatment for your individual needs.
Frequently Asked Questions
What exercises are recommended to alleviate knee arthritis symptoms?
Exercise is an essential part of managing knee arthritis. Low-impact exercises such as walking, cycling, and swimming can help reduce pain and stiffness. Strengthening exercises can also help support the knee joint and improve mobility. We recommend consulting with a physical therapist to develop an exercise plan that is tailored to your specific needs.
What non-surgical remedies are available for bone-on-bone knee pain?
While bone-on-bone knee pain is a severe form of knee arthritis, several non-surgical remedies can help alleviate symptoms. These include weight loss, physical therapy, and the use of assistive devices such as braces or shoe inserts. In some cases, corticosteroid injections can also help reduce inflammation and pain.
How can one manage daily life with osteoarthritis of the knee?
Managing daily life with osteoarthritis of the knee involves making lifestyle changes to reduce pain and improve mobility. This includes maintaining a healthy weight, engaging in regular exercise, and avoiding activities that aggravate knee pain. Assistive devices such as canes or walkers can also help reduce stress on the knee joint.
Is it common for arthritis knee pain to extend to other areas of the leg?
Arthritis knee pain can sometimes radiate to other areas of the leg, such as the hips or ankles. This is because the knee joint is connected to other joints and muscles in the leg. However, if you experience severe or sudden pain in other areas of the leg, it is essential to consult with a healthcare provider to rule out other underlying conditions.
What are the latest advancements in non-surgical knee treatments as of 2023?
As of 2023, several non-surgical knee treatments have shown promise in treating knee arthritis. These include regenerative therapies such as platelet-rich plasma (PRP) and stem cell injections. These therapies aim to promote the body’s natural healing processes and may help reduce inflammation and pain in the knee joint.
Are there effective treatments for knee arthritis that can prevent the need for knee replacement?
While knee replacement surgery is often the last resort for severe knee arthritis, several effective treatments can help prevent the need for surgery. These include weight loss, physical therapy, and the use of assistive devices such as braces or shoe inserts. In some cases, corticosteroid injections or regenerative therapies such as PRP or stem cell injections can also help reduce pain and inflammation in the knee joint.
Knee pain can be a debilitating condition that affects many individuals. Whether it’s due to an injury, arthritis, or other underlying causes, finding the right doctor is crucial for effective treatment. In this article, we will explore the key aspects of understanding knee pain, choosing the right doctor, diagnostic procedures, and treatment options.
Key Takeaways
Understanding the anatomy of the knee is essential in identifying the source of knee pain.
Common causes of knee pain include injuries, arthritis, and overuse.
Finding a knee pain specialist who is experienced in treating your specific condition is important for effective care.
Imaging tests such as X-rays and MRIs can help diagnose the cause of knee pain.
Rehabilitation and physical therapy play a crucial role in the recovery process after knee surgery.
Understanding Knee Pain
Anatomy of the Knee
When we consider the complexity of the human body, the knee is a remarkable structure. It’s not just a simple hinge joint; it’s a sophisticated system that allows for a wide range of motion while supporting the body’s weight. The knee comprises four main components: bones, cartilage, ligaments, and tendons.
The bones form the framework and include the femur (thigh bone), tibia (shin bone), and patella (kneecap). The cartilage, particularly the meniscus, acts as a cushion and helps the bones glide smoothly over each other. Ligaments connect bones to bones, providing stability, while tendons connect muscles to bones, allowing us to move our legs with ease.
Understanding the anatomy of the knee is crucial for identifying the source of pain and determining the appropriate treatment. Here’s a quick overview of the key structures:
Femur: The upper leg bone that articulates with the knee.
Tibia: The lower leg bone forming the lower part of the knee joint.
Patella: Also known as the kneecap, it protects the knee joint.
Meniscus: Two crescent-shaped cartilage pieces that cushion and stabilize the knee.
Ligaments: Including the ACL, PCL, MCL, and LCL, they provide knee stability.
Tendons: Such as the patellar tendon, they connect muscles to the bones.
Remember, maintaining knee health is essential for mobility and overall well-being. Regular exercise and avoiding excessive strain can help preserve knee function.
Common Causes of Knee Pain
Understanding the common causes of knee pain is crucial in identifying the underlying issues. In many cases, overuse or injury to the knee can lead to pain and discomfort. Additionally, conditions such as osteoarthritis and rheumatoid arthritis are known to contribute to knee pain. It’s important to note that factors like age, weight, and activity level can also play a significant role in the development of knee pain. Understanding these causes can help us make informed decisions about seeking medical attention and treatment for our knee pain.
Types of Knee Pain
We recognize that knee pain can manifest in various forms, each with its own set of challenges and implications for treatment. Broadly, knee pain can be categorized into acute, subacute, and chronic, depending on the duration and onset of symptoms. Acute knee pain often results from injuries such as ligament tears or fractures, and typically demands immediate attention.
Acute Knee Pain
Subacute Knee Pain
Chronic Knee Pain
For instance, chronic knee pain may develop over time due to conditions like osteoarthritis or tendinitis, and may require a different approach to management. It’s essential to identify the type of knee pain as it guides the subsequent diagnostic and therapeutic strategies.
Tip: Always consult with a healthcare professional to accurately diagnose the type of knee pain you’re experiencing, as this will significantly influence the effectiveness of your treatment plan.
Choosing the Right Doctor
Qualities to Look for in a Knee Pain Doctor
When we seek medical attention for knee pain, it’s crucial to find a doctor who not only has the expertise but also possesses certain qualities that can make a significant difference in our treatment experience. One of the primary qualities to look for is empathy. An empathetic doctor can provide a level of comfort and understanding that is invaluable during treatment. Additionally, we should look for a doctor who is communicative and transparent about diagnoses and treatment plans.
Another key quality is the doctor’s commitment to staying abreast of the latest medical advancements in knee pain treatment. This ensures that we have access to the most current and effective treatment options. Moreover, a good knee pain doctor should have a proven track record of success with patients suffering from similar conditions.
Here’s a list of qualities that are important when choosing a knee pain doctor:
Empathy and patient comfort
Clear communication and transparency
Up-to-date with medical research
Successful patient outcomes
Remember, the relationship with your knee pain doctor is a partnership. It’s essential to choose someone who you feel comfortable with and who supports your journey to recovery.
Finding a Specialist
When we embark on the journey to find the best knee pain specialist, it’s crucial to consider the type of doctor that will best suit our needs. Orthopedic surgeons are often the go-to specialists for knee pain, as they focus on the musculoskeletal system. However, depending on the cause and severity of the knee pain, we might also consider seeing a rheumatologist for inflammatory conditions, or a physiatrist for rehabilitation and pain management.
To streamline our search, we can create a list of potential specialists based on referrals, insurance coverage, and proximity. Here’s a simple process we can follow:
Gather referrals from primary care physicians, friends, or family members.
Verify the doctor’s credentials and specialization through medical boards or professional directories.
Check if the specialist is covered by our insurance plan.
Consider the location of the clinic for convenience and accessibility.
Tip: Always verify the specialist’s experience with your specific knee condition before scheduling an appointment.
Once we have a list of potential specialists, we can further narrow down our choices by considering factors such as the doctor’s communication style, patient reviews, and the range of treatments they offer. It’s important to feel confident in our choice, as the right specialist will not only provide expert care but also guide us through the recovery process with compassion and understanding.
Evaluating Doctor’s Experience
When evaluating a doctor’s experience, we prioritize patient outcomes as a key metric. Our focus is on understanding the success rates of previous treatments and the overall satisfaction of patients under the doctor’s care. This data is crucial in making informed decisions about the doctor’s expertise and ability to deliver effective treatments.
In addition, we consider the number of procedures performed by the doctor, as it provides insight into their level of experience and proficiency in handling various knee pain conditions. This quantitative measure offers valuable information about the doctor’s familiarity with different treatment modalities and their capability to address complex cases.
Furthermore, it is important to note that the length of practice is a significant factor in evaluating a doctor’s experience. A doctor with extensive experience is likely to have encountered a wide range of knee pain scenarios, thereby honing their diagnostic and treatment skills over time.
It is advisable to inquire about the doctor’s experience with specific knee pain conditions, as specialized expertise can greatly impact the quality of care and treatment outcomes.
Diagnostic Procedures
Physical Examination
When we seek medical attention for knee pain, the initial step is often a thorough physical examination. During this assessment, the doctor will evaluate the knee’s range of motion, stability, strength, and overall alignment. They may also check for signs of swelling, tenderness, or redness which can indicate inflammation or injury.
Palpation is a key component of the physical examination, where the doctor applies gentle pressure to different parts of the knee to identify any abnormalities or pinpoint the source of pain. It’s important to provide accurate feedback during this process to help the doctor make a correct diagnosis.
Here’s a brief overview of what to expect during a physical examination:
Observation of gait and posture
Assessment of joint mobility
Palpation of the knee structure
Evaluation of ligament integrity
Testing for meniscal damage
Tip: Be prepared to discuss the history of your knee pain, including any specific movements or activities that exacerbate the discomfort. This information is crucial for a comprehensive evaluation.
Imaging Tests for Knee Pain
After undergoing imaging tests for knee pain, we will receive a comprehensive report detailing the condition of our knee joint. This report will include information about any abnormalities, such as fractures, dislocations, or signs of arthritis. Additionally, the report may provide quantitative data on the extent of tissue damage, which can help guide the treatment plan. We can expect the report to be presented in a clear and organized manner, allowing us to understand the findings easily. If we have any questions or need further clarification, we should not hesitate to discuss the report with our doctor.
Laboratory Tests for Knee Pain
Laboratory tests play a crucial role in diagnosing the underlying causes of knee pain. These tests provide valuable insights into the presence of inflammatory markers, infection, and other systemic conditions that may contribute to knee discomfort. Interpreting the results of these tests requires a comprehensive understanding of the patient’s medical history and current symptoms. It is important to note that laboratory tests alone may not provide a definitive diagnosis, but they are an essential component of the diagnostic process. Collaboration between the patient, the doctor, and the laboratory professionals is key to ensuring accurate and meaningful results.
Implement a table for presenting structured, quantitative data. Ensure it’s succinct and formatted correctly in Markdown.
Use a bulleted or numbered list for less structured content, like steps, qualitative points, or a series of related items.
Treatment Options
Non-Surgical Treatments
Non-surgical treatments for knee pain are often the first line of defense in managing the condition. Physical therapy plays a crucial role in strengthening the muscles around the knee and improving flexibility. Additionally, anti-inflammatory medications may be prescribed to reduce pain and swelling. It’s important to note that these treatments are most effective when combined with lifestyle modifications, such as weight management and activity modification.
Implementing a table for presenting structured, quantitative data is not applicable in this context.
Use a bulleted or numbered list for less structured content, like steps, qualitative points, or a series of related items.
A personalized exercise program tailored to the individual’s needs
Use of supportive devices such as knee braces or orthotics
Application of ice or heat therapy to alleviate discomfort
It is essential to consult a qualified healthcare professional before starting any new treatment regimen. Each individual’s condition is unique, and personalized care is crucial for effective management of knee pain.
Surgical Interventions
When conservative treatments for knee pain do not yield the desired results, we may consider surgical interventions. These procedures are aimed at relieving pain, restoring function, and improving quality of life. The decision to proceed with surgery is made carefully, taking into account the individual’s specific condition, age, activity level, and overall health.
Surgical options vary depending on the diagnosis and severity of knee pain. Common surgeries include arthroscopy, partial or total knee replacement, and ligament reconstruction. Each procedure has its own set of indications, risks, and recovery times.
Tip: Always discuss the potential benefits and risks of surgery with your doctor to make an informed decision.
Here is a list of surgical interventions commonly performed for knee pain:
Arthroscopic surgery to repair or remove damaged cartilage
Partial knee replacement for cases where damage is limited to a particular area
Total knee replacement for severe arthritis or damage
ACL reconstruction to repair a torn anterior cruciate ligament
Osteotomy to realign bones and relieve pressure on the knee joint
Rehabilitation and Recovery
After undergoing knee surgery, the journey towards regaining full mobility and strength is paramount. We emphasize the importance of a structured rehabilitation program, which is tailored to the individual needs of each patient. Rehabilitation is not a one-size-fits-all process; it requires careful planning and adjustment based on the patient’s progress.
Recovery times can vary, and it’s crucial to set realistic goals and milestones. A typical rehabilitation program may include the following stages:
Initial rest and pain management
Gradual increase in movement and weight-bearing activities
Strength training and conditioning
Functional exercises to restore normal knee function
Tip: Always follow the guidance of your rehabilitation professionals to avoid setbacks and ensure the best outcome.
Monitoring progress is a key component of successful recovery. Patients should expect regular evaluations with their healthcare team to ensure that the rehabilitation plan remains effective and responsive to their healing journey.
Conclusion
In conclusion, finding the best knee pain doctor near you is a crucial step in managing and treating knee pain effectively. By considering factors such as expertise, experience, and patient reviews, individuals can make informed decisions when seeking medical care for their knee pain. It is essential to prioritize one’s health and well-being by seeking out a qualified and reputable knee pain doctor who can provide personalized and effective treatment options.
Frequently Asked Questions
What are the common symptoms of knee pain?
Common symptoms of knee pain include swelling, stiffness, redness, warmth, weakness, and instability in the knee.
How can I prevent knee pain?
To prevent knee pain, it’s important to maintain a healthy weight, exercise regularly, wear proper footwear, avoid sudden increases in physical activity, and use proper techniques during sports and exercise.
What are the non-surgical treatment options for knee pain?
Non-surgical treatment options for knee pain include physical therapy, medications, injections, bracing, and lifestyle modifications such as weight management and activity modification.
What are the common imaging tests used to diagnose knee pain?
Common imaging tests for diagnosing knee pain include X-rays, MRI (Magnetic Resonance Imaging), CT (Computed Tomography) scans, and ultrasound.
How long does it take to recover from knee surgery?
Recovery time from knee surgery varies depending on the type of surgery and individual factors. It can range from a few weeks to several months, and rehabilitation plays a crucial role in the recovery process.
What should I look for in a specialist for knee pain treatment?
When looking for a specialist for knee pain treatment, consider their experience, expertise in knee-related conditions, communication style, and their approach to personalized treatment plans.
Inverted knees, also known as genu recurvatum, is a condition where the knees bend backwards, causing discomfort and difficulty in movement. This article explores the anatomy, causes, symptoms, diagnosis, and treatment options for managing inverted knees.
Key Takeaways
Understanding the anatomy and causes of inverted knees is essential for effective treatment and management.
Physical therapy plays a crucial role in strengthening the muscles around the knee and improving flexibility.
Bracing and support devices can help stabilize the knee joint and reduce strain on the inverted knees.
Surgical treatment for inverted knees may involve realignment procedures and a comprehensive rehabilitation process.
Regular orthopedic evaluations are important for monitoring the progress of inverted knee treatment and addressing any potential complications.
Understanding Inverted Knees
Anatomy of Inverted Knees
Inverted knees, also known as genu varum, are characterized by an inward deviation of the knees. This condition can affect individuals of all ages, from children to adults. The alignment of the lower extremities plays a crucial role in weight-bearing and locomotion. Understanding the anatomy of inverted knees is essential for evaluating the impact of this condition on musculoskeletal function. The table below summarizes the key anatomical features of inverted knees:| Feature | Description || — | — || Femoral-Tibial Angle | The angle formed by the intersection of the femur and tibia. || Joint Space Width | The distance between the femur and tibia at the knee joint. || Patellar Alignment | The position of the patella in relation to the femur and tibia. |
Causes of Inverted Knees
We recognize that the etiology of inverted knees is multifaceted, often involving a combination of genetic and environmental factors. Genetic predisposition plays a significant role, as the condition can run in families. However, environmental influences, such as repetitive stress on the knees from certain sports or occupations, also contribute to the development of this condition.
Injuries and muscle imbalances are other critical factors that can lead to inverted knees. For instance, damage to the knee ligaments or muscles can alter leg alignment, causing the knees to invert. Additionally, muscle weakness, particularly in the muscles around the hips and thighs, can exacerbate this misalignment.
Genetic Predisposition
Repetitive Stress
Injuries and Muscle Imbalances
Muscle Weakness
Tip: Strengthening exercises for the hips and thighs can help in managing knee alignment and reducing the risk of inverted knees.
Symptoms of Inverted Knees
Inverted knees can cause discomfort and affect our daily activities. It’s important to pay attention to subtle changes in the alignment of the knees, such as inward pointing of the knees during standing or walking. These changes may indicate the presence of inverted knees and should be evaluated by a healthcare professional. Additionally, individuals with inverted knees may experience instability during physical activities, which can lead to further complications. It’s crucial to recognize these symptoms early and seek appropriate medical advice.
Diagnosing Inverted Knees
Physical Examination
Upon completion of the physical examination, we carefully analyze the patient’s gait, joint stability, and range of motion. Additionally, we assess for any signs of discomfort or pain during movement. This comprehensive evaluation informs our decision-making process and guides the development of a personalized treatment plan.
In some cases, imaging tests such as X-rays, MRIs, or CT scans may be utilized to further assess the alignment and condition of the knee joint. These diagnostic tools provide valuable insights into the structural integrity and any potential abnormalities.
Furthermore, the orthopedic evaluation involves a detailed assessment of the patient’s medical history, previous injuries, and lifestyle factors that may contribute to the condition. This holistic approach enables us to consider all relevant factors when determining the most effective course of action.
Lastly, it is important to note that the results of these diagnostic procedures are crucial in establishing a precise diagnosis and formulating an evidence-based treatment strategy.
Imaging Tests
In our assessment of inverted knees, we place significant emphasis on imaging tests. These tests provide us with a detailed view of the knee’s structure, allowing us to identify any abnormalities or underlying conditions that may be contributing to the inversion. Common imaging tests include X-rays, which can reveal bone deformities, and MRI scans, which offer a more comprehensive look at both bone and soft tissue.
Magnetic Resonance Imaging (MRI):* Provides detailed images of soft tissues such as ligaments, tendons, and cartilage.
X-ray:* Useful for detecting bone deformities and ruling out other conditions.
Ultrasound:* Can assess the soft tissue structures around the knee and their dynamic function.
Remember, the choice of imaging test will depend on the individual’s specific condition and the information required to formulate an effective treatment plan.
Orthopedic Evaluation
After the orthopedic evaluation, we carefully assess the patient’s range of motion, joint stability, and gait. Additionally, we may conduct specialized tests to evaluate ligament and tendon function. We prioritize a comprehensive approach to ensure accurate diagnosis and personalized treatment plans. This may involve collaborating with other healthcare professionals to gather a holistic view of the patient’s condition. In some cases, a table summarizing the results of the evaluation may be beneficial for tracking progress and informing treatment decisions.
Non-Surgical Treatment Options
Physical Therapy
Physical therapy plays a crucial role in the management of inverted knees. It is a comprehensive approach that focuses on improving strength, flexibility, and range of motion in the affected knees. Our team emphasizes the importance of personalized exercise regimens tailored to each patient’s specific needs. Additionally, we track progress through regular assessments to ensure that the therapy is yielding the desired results. Here’s a brief overview of the key components of physical therapy for managing inverted knees:
Strength Training: Targeted exercises to build muscle strength and stability around the knee joint.
Flexibility Exercises: Techniques to enhance the flexibility of the knee joint and surrounding muscles.
Range of Motion Activities: Controlled movements to improve the range of motion in the knee joint.
By incorporating these elements into our physical therapy programs, we aim to optimize the functional capacity of the knees and enhance overall mobility and comfort.
Bracing and Support
After discussing the benefits of bracing and support in managing inverted knees, we can see that these interventions play a crucial role in providing stability and reducing discomfort. Bracing helps to align the knee joint, while support aids in distributing weight more evenly. It’s important to note that the effectiveness of these interventions may vary depending on the severity of the condition and individual response. Additionally, a table comparing different types of braces and their features can provide valuable insights for patients and healthcare professionals alike. This table can include information on material, adjustability, and recommended usage. Furthermore, a bulleted list outlining the key considerations for selecting the appropriate brace can help patients make informed decisions. Remember, proper fitting and regular assessment are essential for optimal outcomes.
Pain Management
After exploring various non-surgical treatment options, we have found that physical therapy is an essential component of managing inverted knees. It focuses on strengthening the muscles around the knee joint and improving flexibility. Additionally, bracing and support can provide stability and reduce discomfort during physical activities. Pain management techniques, such as medication and ice therapy, are also crucial for alleviating discomfort and promoting mobility. Here’s a brief overview of the non-surgical treatment options:
Treatment Option
Description
Physical Therapy
Strengthens muscles and improves flexibility
Bracing and Support
Provides stability and reduces discomfort
Pain Management
Alleviates discomfort and promotes mobility
It’s important to note that these non-surgical treatment options may vary based on individual needs and the severity of the condition. Seeking professional guidance is essential for determining the most suitable treatment plan for each patient.
Surgical Treatment for Inverted Knees
Surgical Procedures
Surgical procedures for treating inverted knees are crucial for addressing severe cases. These procedures may include realignment osteotomy, soft tissue release, and ligament reconstruction. Each procedure is tailored to the individual’s specific condition and needs.
Realignment Osteotomy: This procedure involves cutting and repositioning the bone to correct the alignment of the knee joint.
Soft Tissue Release: This technique focuses on releasing tight or contracted soft tissues around the knee joint to improve mobility and function.
Ligament Reconstruction: This surgical intervention aims to repair or replace damaged ligaments, restoring stability and strength to the knee.
Tip: Post-surgery rehabilitation plays a vital role in optimizing outcomes. Adhering to the prescribed rehabilitation plan and closely following the guidance of healthcare professionals is essential for a successful recovery.
Rehabilitation Process
Following surgical intervention for inverted knees, we embark on a critical phase: the rehabilitation process. This journey is tailored to each individual’s needs, aiming to restore knee function and strength. We typically observe a phased approach, starting with gentle range-of-motion exercises and gradually incorporating strength training and functional activities.
In the initial weeks, patients may experience varying degrees of discomfort and swelling. It’s essential to adhere to the prescribed pain management plan and to monitor for any signs of complications. As we progress, we introduce more demanding exercises, always within the patient’s tolerance levels.
Rehabilitation Timeline:
Week 1-2: Gentle range-of-motion exercises, swelling control, and pain management.
Week 3-6: Gradual introduction of weight-bearing activities and strength exercises.
Week 7-12: Increased exercise intensity and functional training.
Remember, the path to recovery is not always linear. A client’s recovery from knee surgery was going well until a setback at week 10. Despite setbacks, overcoming them with the right strategies is possible.
We encourage patients to maintain open communication with their rehabilitation team, reporting any concerns or unusual symptoms immediately. It is through this collaborative effort that we can ensure the best possible outcome for our patients.
Potential Risks and Complications
After undergoing surgical treatment for inverted knees, it is important to be aware of the potential risks and complications that may arise. These can include infection, blood clots, and nerve damage. Additionally, there is a possibility of prolonged recovery time and the need for further interventions. It is crucial to closely follow post-operative care instructions and attend all scheduled follow-up appointments to monitor and address any issues that may arise. Vigilance and proactive communication with your healthcare provider are essential for ensuring a successful recovery.
Conclusion
In conclusion, the management of inverted knees presents a complex challenge, requiring a multifaceted approach that encompasses both conservative and surgical interventions. While physical therapy and orthotic devices play a crucial role in mitigating symptoms, surgical correction may be necessary in severe cases. The decision-making process should be guided by a thorough assessment of the individual’s condition, taking into account factors such as age, activity level, and overall health. Further research and advancements in medical technology are essential for enhancing the efficacy of treatment options for this condition.
Frequently Asked Questions
What are the common causes of inverted knees?
The common causes of inverted knees include genetics, muscle imbalances, and abnormal bone structure.
Can physical therapy help with inverted knees?
Yes, physical therapy can be beneficial for strengthening muscles, improving flexibility, and correcting alignment in inverted knees.
Are there non-surgical treatment options for managing inverted knees?
Yes, non-surgical treatment options include physical therapy, bracing, and pain management techniques.
What surgical procedures are available for treating inverted knees?
Surgical procedures such as osteotomy and realignment surgery may be recommended for severe cases of inverted knees.
What are the potential risks and complications of surgical treatment for inverted knees?
Potential risks and complications of surgical treatment include infection, blood clots, and nerve damage.
How long is the rehabilitation process after surgical treatment for inverted knees?
The rehabilitation process after surgical treatment can vary, but it typically involves physical therapy and gradual return to normal activities.




 in the human knee joint, rendered in highly realistic medical illustration style. The MCL is prominently featured in the center foreground, shown with its characteristic fan-like structure and attachments to the femur and tibia. The surrounding musculature, tendons, and bony landmarks are clearly visible, allowing for a comprehensive understanding of the MCL's anatomical context. The lighting is soft and directional, creating subtle shadows that enhance the three-dimensional form. The background is minimalist, with a plain, neutral color palette to avoid distractions and focus the viewer's attention on the MCL structure. The overall tone is educational and informative, suitable for use in a medical article on knee instability.")