Drs. Ali H. Mesiwala and Grant D. Shifflett participate in the pivotal two-level study of the safety and effectiveness of the Orthofix M6-C™ artificial cervical disc compared to anterior cervical discectomy and fusion.
NEWPORT BEACH, Calif., Nov. 28, 2023 /PRNewswire/ – DISC Surgery Center of Newport Beach (“DISC”), committed to supporting research vital to the field of spine care, has announced its participation in a clinical trial to artificial disc replacement and is now enrolling qualified patients. Candidates may include patients between the ages of 18 and 75 who have been told they need cervical (neck) surgery at two consecutive levels (among other requirements).
Drs. Ali H. Mesiwala and Grant D. Shifflett – both board-certified, fellowship-trained spine surgeons at DISC – join other experts at approximately 30 clinical sites participating in this study across the country. The primary objective of the study is to evaluate the safety and effectiveness of the Orthofix M6-C™ artificial cervical disc (already FDA-approved for single-level surgery) in patients with contiguous symptomatic bilevel cervical radiculopathy, with or without umbilical cord compression. The results will then be compared with those in patients undergoing anterior cervical discectomy and fusion (ACDF).
Artificial disc replacement surgery is very similar to ACDF surgery. Both procedures remove the damaged disk. However, when the damaged disc is removed to replace the disc, the space between the vertebrae is filled with a specialized implant called an artificial disc, instead of a bone graft. The artificial disc is designed to restore the distance between the vertebrae while still allowing some movement.
With its track record as a national leader in outpatient spine and its team’s extensive experience performing advanced motion maintenance techniques, DISC is ideally positioned to participate in such research.
“The DISC Surgery Center in Newport Beach has placed more than 3,000 cervical discs since 2018 and we are well versed in the motion-preserving qualities of the surgery,” said Dr. Mesiwala. “I think it is important to stay actively involved in research to improve patient care, so I wanted to be part of a study that will improve our learnings and discoveries.”
Dr. Shifflett added, “As pioneers in minimally invasive spine surgery and techniques, we always welcome the opportunity to advance the field while informing the treatment options available to patients.”
Patients who would like to know if they are eligible for this study can visit https://www.discmdgroup.com/adr-clinical-study/.
About DISC Surgery Center in Newport Beach DISC Surgery Center in Newport Beach is a purpose-built outpatient clinic focused on providing patients with the safest, most advanced minimally invasive spine surgery, orthopedic sports medicine, total joint replacement and pain management. DISC is a subsidiary of TriasMD, a portfolio company of Chicago Pacific Founders, and also an official partner of Red Bull Athlete Performance Center. For more information, call 949-988-7800, visit www.discmdgroup.com or follow @DISCMD on Instagram.
Media contact:
Kristien Brada-Thompson
760-274-6393
369218@email4pr.com
Scanlan AT, Berkelmans DM, Vickery WM, Kean CO. An overview of the internal and external physiological demands of batting in cricket. Int J Sports Physiol Perform. 2016;11(8):987–97.
Article PubMed Google Scholar
Ali K, Khan MH. The effects of plyometric training on grass and clay on jumping, sprinting and agility in collegiate cricketers. Int J Biomed Adv Res. 2013;4(12):902–8.
Article Google Scholar
Medicine ACoS. American College of Sports Medicine Position Standard. Progression models in resistance training for healthy adults. Med Sci Sports Exercise. 2009;41(3):687–708.
Article Google Scholar
Grgic J, Schoenfeld BJ, Davies TB, Lazinica B, Krieger JW, Pedisic Z. Effect of resistance training frequency on gains in muscle strength: a systematic review and meta-analysis. Sports Med. 2018;48(5):1207–2020.
Article PubMed Google Scholar
Chu DA, Panariello RA. Jumping plyometrics: Sport-specific plyometrics: Baseball pitching. Nat Strength Cond Assn J. 1989; 11:81–5.
Article Google Scholar
Markovic G. Does plyometric training improve vertical jump height? A meta-analytic review. Br J Sports Med. 2007;41(6):349–55.
Article PubMed PubMed Central Google Scholar
Baechle TR, Earle RW. Basics of strength training and conditioning. 3rd edition. Human kinetics; 2008. p. 417.
Luebbers PE, Potteiger JA, Hulver MW, Thyfault JP, Carper MJ, Lockwood RH. Effects of plyometric training and recovery on vertical jump performance and anaerobic strength. J Strength Cond Res. 2003;17(4):704–9.
PubMed Google Scholar
MacDonald CJ, Lamont HS, Garner JC. A comparison of the effects of six weeks of traditional resistance training, plyometric training, and complex training on strength measurements and anthropometry. J Strength Cond Res. 2012;26(2):422–31.
Article PubMed Google Scholar
Thapa RK, Lum D, Moran J, Ramirez-Campillo R. Effects of complex training on the sprinting, jumping and change of direction ability of football players: a systematic review and meta-analysis. Front Psychol. 2021;11:627869.
Article PubMed PubMed Central Google Scholar
Baker D. Acute effect of alternating heavy and light resistance on power output during complex upper body strength training. J Strength Cond Res. 2003;17(3):493–7.
PubMed Google Scholar
French DN, Kraemer WJ, Cooke CB. Changes in dynamic exercise performance after a series of preconditioning isometric muscle actions. J Strength Cond Res. 2003;17(4):678–85.
PubMed Google Scholar
Fatouros IG, Jamurtas AZ, Leontsini D, Taxildaris K, Aggelousis N, Kostopoulos N, et al. Evaluation of plyometric exercise training, strength training and their combination on vertical jumping performance and leg strength. J Strength Cond Res. 2000;14(4):470–6.
Google Scholar
Ingle L, Sleap M, Tolfrey K. The effect of a complex training and detraining program on selected strength and power variables in early pubertal boys. J Sports science. 2006;24(9):987–97.
Article PubMed Google Scholar
Ebben WP, Jensen RL, Blackard DO. Electromyographic and kinetic analysis of complex training variables. J Strength Cond Res. 2000;14(4):451–6.
Google Scholar
Anant S, Choudhary R, Venugopal R. Effect of core training on anaerobic strength, explosiveness, repetitive strength and endurance of male players. Int Human Res J 2014;2(3):1–8.
Dallas GC, Pappas P, Ntallas CG, Paradisis GP, Exell TA. The effect of four weeks of plyometric training on the reactive strength index and leg stiffness is sport-dependent. J Sports Med Phys Fitness. 2020;60(7):979–84.
Article PubMed Google Scholar
Anant SK, Venugopal R. Effect of eight-week Swiss ball training on the core muscles of male players. Int J Mov Educ Soc Sci. 2015;3(2):53–5.
Army LA, Lambert J. A 20 m maximum multi-stage shuttle run test to predict $$\dot V$$ O2 max. Eur J Appl Physiol. 1982;49(1):1–12.
Article CAS Google Scholar
Lau C, Yu R, Woo J. Effects of a 12-week hatha yoga intervention on cardiorespiratory endurance, muscle strength and endurance and flexibility in Chinese adults in Hong Kong: a controlled clinical trial. Evid-based complement Alternat Med. 2015;2015:12. Article ID 958727. https://doi.org/10.1155/2015/958727.
Rahimi R, Behpur N. The effects of plyometric, weight and plyometric strength training on anaerobic strength and muscular strength Facta universitatis series. Physical Edu Sports. 2005;3(1):81–91.
Google Scholar
Ali K, Verma S, Ahmad I, Singla D, Saleem M, Hussain ME. Comparison of complex versus contrast training on steroid hormones and sports performance in male football players. J Chiropr Med. 2019;18(2):131–8.
Article PubMed PubMed Central Google Scholar
Gabriel DA, Kamen G, Frost G. Neural adaptations to resistance exercise. Sports Med. 2006;36(2):133–49.
Article PubMed Google Scholar
Freitas TT, Martinez-Rodriguez A, Calleja-Gonzalez J, Alcaraz PE. Short-term adaptations after complex training in team sports: a meta-analysis. PLoS One. 2017;12(6): e0180223.
Article PubMed PubMed Central Google Scholar
Hrysomallis C, Kidgell D. Effect of heavy dynamic resistance exercise on acute upper body strength. J Strength Cond Res. 2001;15(4):426–30.
CAS PubMed Google Scholar
Holm L, Reitelseder S, Pedersen TG, Dossing S, Petersen SG, Flyvbjerg A, et al. Changes in muscle size and MHC composition in response to resistance exercise with heavy and light loading intensity. J Appl. Physiol. 2008;105(5):1454–61.
Article CAS PubMed Google Scholar
Evans AK, Durham MP, Hodgkins TD, Sinclair DR, Adams KJ. Acute effects of bench press on power output during a subsequent ballistic bench throw. Med Sci Sports Exercise. 2001;33(5):S325.
Article Google Scholar
Ritchie D, Keogh JWL, Reaburn P, Bartlett JD. The use of one and four minutes of recovery when using the contrast method of resistance training does not negatively impact subsequent jump performance when concurrent training is involved. PeerJ. 2020;13(8):e10031. https://doi.org/10.7717/peerj.10031.PMID:33083124;PMCID:PMC7566756.
Article Google Scholar
McKendry J, Pérez-López A, McLeod M, Luo D, Dent JR, Smeuninx B, et al. Short rest between sets attenuates resistance exercise-induced increases in myofibrillar protein synthesis and intracellular signaling in young men. Exp Physiol. 2016;101(7):866–82.
Article CAS PubMed Google Scholar
Jensen RL. Kinetic responses during landings of plyometric exercises. In Proceedings of the XXVI Congress of the International Society of Biomechanics in Sports (Kwon, YH, Shim, J, Shim, JK, and Shin, IS, editors). 2008; 393–6.
Adams K, O’Shea JP, O’Shea KL, Climstein M. The effect of six weeks of squat, plyometric, and squat-plyometric training on energy production. J Applied Sports Sci Res. 1992;6(1):36–41.
CAS Google Scholar
Herrero J, Izquierdo M, Maffiuletti N, Garcia-Lopez J. Electromyostimulation and plyometric training effects on jumping and sprinting time. Int J Sport Med. 2006;27(07):533–9.
CHICAGO, Nov. 27, 2023 /PRNewswire/ — Stronger quadriceps muscles, compared to the hamstrings, may lower the risk of total knee replacement, according to research presented today at the annual meeting of the Radiological Society of North America (RSNA). Researchers said the findings could inform strength training programs for people with advanced knee arthritis.
Advanced knee osteoarthritis is a leading cause of pain and disability worldwide. In the US alone, 14 million adults have symptomatic knee osteoarthritis, and more than half of diagnosed patients are expected to eventually undergo total knee replacement surgery.
Although stronger muscle groups are generally thought to be associated with a lower rate of total knee replacements, their relative importance is not well established. Of particular importance is the relationship between the extensors and the hamstrings, the two main muscle groups in the knee.
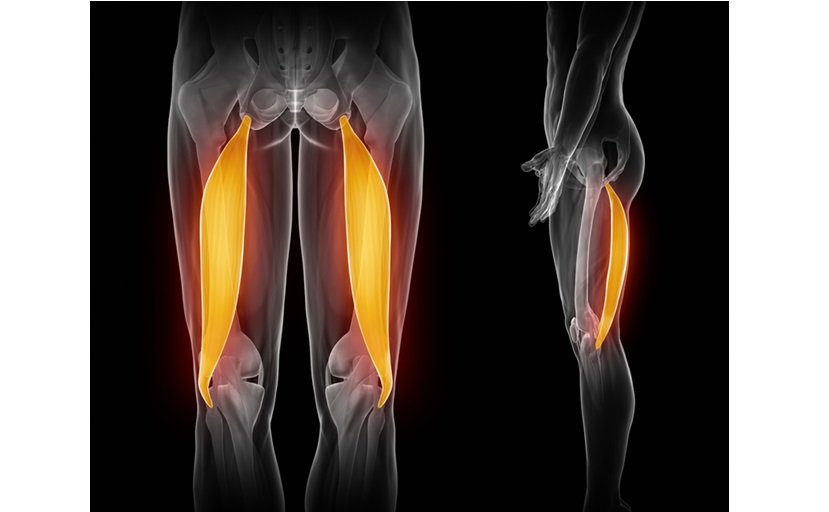
The extensors, the muscles at the front of the thigh, commonly called the quadriceps, are the strongest muscle group in the body and have a vital influence on walking, other activities and biomechanics. The muscles around the back of the thigh, known as the hamstrings, are responsible for the extension of the hip and flexion of the knee, making them equally essential for physical activity.
“The two muscle groups act as opposing forces, and the balance between them allows for a wide range of activities while protecting the knee joint,” says lead study author Upasana Upadhyay Bharadwaj, MD, of the University of California, San Francisco (UCSF). “An imbalance, among other factors, leads to a change in biomechanics, resulting in the progression of osteoarthritis.”
Dr. Upadhyay Bharadwaj and colleagues evaluated thigh muscle volume in 134 participants in the Osteoarthritis Initiative, a nationwide study sponsored by the National Institutes of Health. They compared 67 patients who underwent total knee replacement of one knee with 67 control participants who did not undergo knee replacement. The cases and controls were matched on variables such as age and gender.
The researchers obtained 3T MRI of the thigh at the time of surgery. They also evaluated MRI findings two years and four years before surgery. They used a previously trained deep learning model to segment and calculate the volumes of the muscles of the thigh – measurements that are difficult to calculate manually.
When comparing patients who had undergone total knee replacement with the control group, a higher ratio of quadriceps to hamstring volume was significantly associated with a lower likelihood of total knee replacement. Higher hamstring and gracilis volumes, a long, thin muscle on the inside of the thigh, were also associated with a lower likelihood of total knee replacement.
“Our research shows that in addition to strong individual muscles, larger extensor muscle groups – compared to hamstring muscle groups – are significantly associated with a lower likelihood of total knee replacement surgery within two to four years,” said Dr. Upadhyay Bharadwaj.
The study results have implications for both the interpretation of imaging studies and clinical management. The results suggest that training programs that strengthen the quadriceps in relation to the hamstrings may be beneficial.
“Although we assume that total muscle volume is important as a surrogate marker of muscle strength, the relationship, and therefore balance, between the extensor and hamstring muscles may be more important and significantly associated with a lower likelihood of total knee replacement,” Dr. Upadhyay Bharadwaj said.
Although the study focused on people with arthritis, the findings could also help inform strength training for a broader segment of the population.
“While these results are essential for targeted therapy in a population at risk for osteoarthritis, even the general public can benefit from our results by preventively incorporating appropriate strengthening exercises,” said Dr. Upadhyay Bharadwaj.
Co-authors are John A. Lynch, Ph.D., Gabby B. Joseph, Ph.D., and Thomas M. Link, MD, Ph.D.
Note: Copies of RSNA 2023 news releases and electronic images will be available online at RSNA.org/press23.
RSNA is an association of radiologists, radiation oncologists, medical physicists and related scientists who promote excellence in patient care and health care through education, research and technological innovation. The association is located in Oak Brook, Illinois. (RSNA.org)
Editor’s note: The data in these publications may differ from the data in the published abstract and the data actually presented at the meeting, as researchers continue to update their data up until the meeting. To ensure you are using the most current information, please call the RSNA Newsroom at 1-312-791-6610.
For patient-friendly information about musculoskeletal imaging, please visit RadiologyInfo.org.
SOURCE Radiological Society of North America (RSNA)
The pinnacle of minimally invasive surgical visualization, Summit™ is the first-of-its-kind 4K single-use surgical arthroscope designed to simplify endoscopy
MANCHESTER, NH, November 27, 2023–(BUSINESS WIRE)–Pristine Surgical, a medical device company committed to making endoscopy more efficient, consistent and safer, has accelerated the launch of its Summit™ 4K single-use surgical arthroscope – the first of its kind. After an overwhelmingly positive response during its limited market launch, Summit™ is now available to hospitals and ambulatory surgery centers across the United States.
“Summit™ is a fully integrated, single-use scope with 4K resolution that simplifies arthroscopic procedures and packs the latest in minimally invasive visualization technology into a sterile, cost-effective, ready-to-use package,” said Bryan Lord, CEO of Pristine Surgical. “I am pleased with the feedback we have received and we are excited to make this groundbreaking arthroscope available nationwide to help surgeons and their teams innovate their endoscopy suite.”
Summit™ is a brand new, 100% sterile 4K scope for every patient and is ready to use right out of the box, eliminating the time-consuming operating room set-up and tear-down process and device reprocessing required for reusable arthroscopes. It comes pre-installed with Pristine Connect™ software for seamless cloud-connected surgical image and video storage and automated inventory management.
“We developed Summit to address the challenges inherent in conventional surgical visualization – which relies on reusable arthroscopes that are becoming outdated, difficult and expensive to maintain, and prone to wear, damage and potential infections,” said Dr. Stephen J. Snyder, a pioneer in shoulder arthroscopy and Chief Medical Officer of Pristine Surgical. “It’s a major leap forward in an area that hasn’t changed much in my 40-plus years of practice, and when we saw the positive response and impact it had on our limited market launch, we were convinced that it was time to fully commercialize Summit.”
Summit integrates with a surgery center’s existing endoscopy tower, allowing ASCs to upgrade to 4K without major capital investments. It is delivered through a unique subscription scope business model and has transparent pricing to make this groundbreaking medical device cost-effective and practical. Through sustainability partnerships, Pristine Surgical will also offer recycling options to its customers.
Summit™ is available through select distributor partners in the United States. For more information or to learn how you can bring Summit to your facility, please contact info@pristinesurgical.com.
About pristine surgery
Pristine Surgical is a medical device company on a mission to simplify endoscopy. The company combines single-use endoscopes with cloud-based software to make minimally invasive visualization more efficient, consistent and safe. Pristine Surgical offers a subscription business model with transparent pricing and automated inventory management, delivering improved workflow and lower costs for the endoscopy suite. For more information, visit pristinesurgical.com or search for the company on LinkedIn.
Contacts
Dia Kalakonas
GM, Marketing Communications
Pristine surgical procedure
603-496-5493
dkalakonas@pristininesurgical.com
Higher concussion rates following COVID-19 infection in high school athletes.
Bullock GS, Emery CA, Nelson VR, etc. al, Br J Sports Med2023; [epub ahead of print]. two: 10.1136/brjsports-2022-106436.
Full text freely available
Take home message
Athletes who tested positive for a COVID-19 infection were more likely to suffer a concussion within 60 days of recovering from the infection than athletes who did not contract COVID-19.
Background
COVID-19 affects the respiratory, cardiovascular and nervous systems. In some cases, COVID-19 can lead to long-term consequences (e.g. impaired cognition). It is currently unknown whether COVID-19 infection affects the risk of sports-related concussions.
Study aim
Bullock and colleagues completed a prospective cohort study to compare concussion rates between high school athletes who recently tested positive for COVID-19 and those who did not.
Methods
The authors recruited athletes from high schools in six states. A certified athletic trainer recorded all cases of COVID-19 infection or concussion. If an athlete reported COVID-like symptoms or had an elevated temperature during a daily screening, the athletic trainer administered a COVID test. The research team also recorded when an athlete participated in a training or competition. The authors focused on the number of concussions within 60 days after an athlete returned to play following a COVID-19 infection. All data was recorded in the Players Health Rehab system, including demographic information, sports and illness data for all athletes.
Results
A total of 72,522 athletes participated in high school sports at the affected school during the 2020-2021 school year. Of these athletes, 430 had COVID-19 infections. Of the athletes with a COVID-19 infection, 32 had a concussion, and 1,241 athletes without COVID-19 had a concussion. An athlete with a history of COVID-19 was approximately 3 times more likely to suffer a concussion within 60 days of returning to play than an athlete without COVID-19.
Viewpoints
Overall, the authors found that prior COVID-19 infection increased the risk of concussion during the first 60 days after recovery from COVID-19. Therefore, the effects of a COVID-19 infection may linger after returning to play. Knowing whether this applies to other sports-related injuries would be interesting. Additionally, learning why these athletes are at greater risk for concussion (e.g., deconditioning, persistent symptoms) can help us develop prevention strategies and make informed decisions about when and how to release an athlete to play following a COVID-19 infection.
Clinical implications
Doctors should explain to patients with COVID-19 that they may experience lingering effects that predispose them to concussion. We need to help the patient make an informed decision about when to return to play after COVID-19 infection. Once an athlete returns, doctors should monitor these patients for concussions.
Questions for discussion
What other measures have you implemented in your clinical practice to monitor athletes after COVID-19 infection? Is a COVID-19 infection something you are currently documenting?
Written by Kyle Harris
Reviewed by Jeffrey Driban
related posts
COVID recovery may require injury prevention training!
Use of cardiovascular magnetic resonance (CMR) imaging for return to athletic activities after COVID-19 infection: an expert consensus document on behalf of the American Heart Association Council on Cardiovascular Radiology and Intervention (CVRI) Leadership and endorsed by the Society for Cardiovascular Magnetic Resonance (SCMR)
Adapted physical activity in subjects and athletes recovering from Covid-19: a position statement of the Società Italiana Scienze Motorie e Sportive
Cardiopulmonary Considerations for High School Athletes During the COVID-19 Pandemic: Update to the NFHS-AMSSM Guidelines
Knee Pain Symptoms and Causes: A Comprehensive Guide
Knee pain can be a bothersome issue that affects people of all ages. It may result from a number of factors, such as injuries like torn cartilage or ruptured ligaments, or medical conditions like arthritis, gout, and infections. Understanding the causes and symptoms of knee pain is essential for seeking timely and appropriate treatment to alleviate discomfort and prevent complications.
In this article, we will explore the various factors that contribute to knee pain and gain insights into different treatment approaches. We will also discuss risk factors and preventive measures to help maintain healthy knees and maintain overall well-being.
patellofemoral pain syndrome:
Understanding Patellofemoral Pain Syndrome
Category
Details
Definition
Pain between the kneecap (patella) and thighbone (femur) due to abnormal biomechanical forces
Common Causes
– Kneecap maltracking/dysfunction<br>- Overuse from sports<br>- Tight quadriceps, IT band, calves <br>- Weak hip and gluteal stabilizers
Contributing Factors
– High Q-angle anatomy<br>- Poor movement patterns<br>- Sudden load increases without adaptation
Affected Populations
– Athletes <br>- Young active adults<br>- Older adults with kneecap arthritis
Conservative Treatment
– Taping/bracing to improve tracking <br>- Targeted stretching & strengthening <br>- Movement pattern retraining
Key components of PFPS involve abnormal kneecap gliding, overloading tissue capacities through sports, and anatomical vulnerabilities. Conservative rehabilitation aims to correct the imbalances, while surgery is occasionally utilized for refractory cases to realign structures or halt arthritis progression.
Key Takeaways
Knee pain can be caused by injuries or medical conditions like arthritis and gout.
Timely diagnosis and treatment can alleviate discomfort and prevent complications.
Understanding risk factors and preventive measures helps maintain healthy knees.
Overview
Knee pain is highly prevalent and affects individuals of all age groups. It can stem from injuries such as torn cartilage or ruptured ligaments or be a result of medical conditions like arthritis, gout, and infections. Fortunately, most minor knee pain cases can be managed through self-care measures, while more severe cases may benefit from physical therapy, knee braces, or even surgical intervention. Our discussion will dive deeper into the complexities of knee pain, exploring muscles, joints, ligaments, tendons, and bones (tibia, patella, and femur) involved in the knee joint.
Symptoms
Recognizing the Signs
Knee pain can manifest in various ways depending on the underlying issue. Some common symptoms accompanying knee pain are:
Swelling and stiffness
Redness and a warm sensation
Weakness or instability
Audible popping or crunching sounds
Difficulty fully straightening the knee
Seeking Medical Attention
We encourage you to consult your doctor if you experience any of the following:
Inability to bear weight on your knee or a feeling of instability
Significant swelling of the knee
Limited extension or flexing of the knee
Visible deformities in your leg or knee
Fever, accompanied by redness, pain, and swelling in the knee
Severe knee pain associated with an injury
From Mayo Clinic to Your Inbox
We’re excited to provide you with the latest research advancements, health tips, current health topics, and advice on managing your health straight to your inbox. Sign up for free and stay informed with information tailored to your needs.
By signing up, we combine your email and website usage information with other details we have about you, ensuring the most relevant and helpful content is delivered to you. For Mayo Clinic patients, rest assured that your protected health information is treated with utmost care and used according to our privacy practices.
Remember, you have the option to opt-out of our email communications at any time by simply clicking the unsubscribe link provided in the email.
Causes of Knee Pain
Injuries Affecting the Knee
Knee injuries can involve various structures around the knee joint, such as ligaments, tendons, bursae, bones, and cartilage. Some common knee injuries are:
ACL injury: A tear in the anterior cruciate ligament, which connects the shinbone to the thighbone, often occurs in sports that require sudden directional changes like basketball or soccer.
Fractures: Knee bones, including the kneecap, may break due to falls or vehicle accidents. Osteoporosis can also lead to knee fractures from minor missteps.
Torn meniscus: The meniscus, the cartilage cushioning between the shinbone and thighbone, may tear if the knee is suddenly twisted while bearing weight.
Knee bursitis: Injuries may cause inflammation in the knee bursae, the fluid-filled sacs that enable smooth movement between tendons, ligaments, and the knee joint.
Patellar tendinitis: This refers to the irritation and inflammation of tendons attaching muscles to bones, particularly the patellar tendon connecting the kneecap and shinbone. It often occurs in runners, skiers, cyclists, and people involved in jumping sports.
Mechanical Issues
Mechanical problems causing knee pain include:
Loose body: Detached bone or cartilage fragments floating in the joint space can obstruct knee joint movement, akin to a pencil caught in a hinge.
Iliotibial band syndrome: Tightening of the iliotibial band, which extends from the hip to the outer knee, can cause rubbing against the thighbone. Distance runners and cyclists are prone to this condition.
Dislocated kneecap: The kneecap can slip out of place, typically to the knee’s outside. In some instances, the dislocation remains visible.
Hip or foot pain: Compensating for pain in the hips or feet by changing one’s gait can place extra stress on the knee joint, leading to pain.
Forms of Arthritis
Various types of arthritis can cause knee pain:
Osteoarthritis: This wear-and-tear condition results from the knee cartilage’s deterioration due to use and age.
Gout: Occurs when uric acid crystals accumulate in the joint, typically affecting the big toe but also the knee.
Pseudogout: Often mistaken for gout, this condition stems from calcium-containing crystals in the joint fluid. The knee is the most frequently affected joint.
Septic arthritis: An infection in the knee joint may lead to swelling, pain, redness, and fever. It can quickly damage the knee cartilage, requiring urgent medical attention.
Additional Issues
Patellofemoral pain syndrome (PFPS) refers to discomfort between the kneecap (patella) and underlying thighbone (femur). It involves abnormal forces transmitted through the patellofemoral joint which is the articulation between these two structures. PFPS commonly affects certain populations, especially athletes who overloaded their knees through repetitive overuse from sports.
The main culprit causing PFPS is maltracking or dysfunction of the kneecap as it glides up and down in a groove on the femur during knee bending. This maltracking indicates a biomechanical imbalance, often from tight muscles or anatomical misalignment pulling the cap sideways. This leads to increased pressures on the back of the patella and the adjacent cartilage, triggering pain.
PFPS frequently develops in young active adults, particularly females, who have naturally higher “Q angles” – an anatomical measurement of kneecap positioning. It also occurs in some older adults for whom the cartilage under the kneecap has worn away significantly due to arthritis, causing bone-on-bone grinding. These groups appear predisposed towards developing knee pain from the aftermath of abnormal patellofemoral mechanics.
Besides overuse from sports and vulnerable anatomy, other PFPS triggers involve sudden increases in loading too quickly. The muscles stabilizing the patella require adaptations to control loads safely. When demands exceed abilities, the kneecap tracking suffers. Additionally, poor movement patterns such as unbalanced squatting or jumping/landing with knock knees induces patellofemoral compression. Often tight quadriceps, IT bands and calves paired with weak hips/glutes contributes to dysfunction.
Several targeted interventions aim at conservatively realigning the patella, strengthening deficient stabilizers, restoring ideal tracking and alleviating compression forces causing PFPS. Using braces, taping, customized exercise corrections and gait pattern retraining are common initial tactics under therapist guidance to calm pain and prevents recurrences. In some cases of refractory PFPS or significant arthritis, surgical options to release or reshape overtightened tissues or resurface damaged articulations provide longer term solutions.
Prevention Strategies for Knee Ligament Injuries: Professional Tips
Knee ligament injuries are common among athletes and can be a frustrating setback for anyone who enjoys an active lifestyle. The knee joint is one of the largest and most complex joints in the body, making it vulnerable to various types of injuries. Understanding and identifying knee ligament injuries is crucial to prevent further damage and promote quick recovery.
The most common knee ligament injuries are the anterior cruciate ligament (ACL), medial collateral ligament (MCL), posterior cruciate ligament (PCL), and lateral collateral ligament (LCL). These injuries can occur due to direct trauma, such as contusions and strains, or from indirect trauma, such as sudden changes in direction. Symptoms of knee ligament injuries include pain, swelling, inflammation, and joint laxity. In this article, we will discuss five prevention strategies for knee ligament injuries to help maintain knee stability and prevent knee instability.
professional tips for prevention strategies to help avoid knee ligament injuries:
Category
Tips
Strength & Flexibility Training
– Emphasize hamstring, glute, quad, hip & core exercises<br>- Ensure muscle imbalances are addressed<br>- Use proper form/technique to prevent overstress
Movement Control & Balance
– Practice proper landing mechanics when jumping <br>- Enhance proprioception & body control<br>- Integrate deceleration drills
Equipment & Environment
– Wear supportive & appropriate footwear <br>- Tape or brace vulnerable knees if needed <br>- Ensure safe, even playing surfaces
Loading & Recovery
– Follow loading guidelines for ramping up intensity<br>- Avoid aggressive pivoting until tissues adapted<br>- Schedule adequate rest periods between sessions
Body Composition & Nutrition
– Prevent muscle loss during injury layoffs<br>- Maintain healthy BMI year-round<br>- Support exercise recovery nutritionally
Mindset & Motivation
– Foster positive, confident mentality<br>- Set smaller achievable goal steps <br>- Enlist social support structure
The most effective ACL/knee ligament injury prevention programs take a comprehensive approach. Optimizing strength, movement mechanics, loading, and nutrition helps create resilience. Confidence in knee stability paired with caution towards unsafe mechanics allows for safer progression. Expert guidance tailoring programs is key for best injury deterrence.
Key Takeaways
Understanding the anatomy of the knee joint and identifying knee ligament injuries can promote quick recovery.
Direct and indirect trauma can cause knee ligament injuries, leading to pain, swelling, inflammation, and joint laxity.
Understanding and Identifying Knee Ligament Injuries
Knee ligament injuries are common among athletes and individuals who engage in physical activities that require jumping, pivoting, or sudden changes in direction. In this section, we will discuss the common types and causes of knee ligament injuries, how to identify symptoms and diagnose the injury, treatment and rehabilitation options, and the role of sex and age in knee ligament injuries.
Common Types and Causes
The most common types of knee ligament injuries are the anterior cruciate ligament (ACL) and medial collateral ligament (MCL) injuries. The ACL is usually injured during non-contact activities such as landing after a jump or sudden stops and changes in direction. On the other hand, the MCL is usually injured from a direct blow to the outer side of the knee, such as when playing football or hockey.
Symptoms and Diagnosis
The symptoms of knee ligament injuries include pain, swelling, bruising, and instability. The diagnosis of knee ligament injuries is usually made through a physical exam and imaging tests such as MRI or X-rays. It is important to seek medical attention if you experience any of these symptoms.
Treatment and Rehabilitation
The treatment and rehabilitation of knee ligament injuries depend on the severity of the injury. Treatment options include rest, ice, compression, and elevation (RICE), physical therapy, and surgery. Rehabilitation includes exercises to improve range of motion, strength, and mobility. It is important to follow the guidance of a physical therapist or orthopedic surgeon to ensure proper recovery.
Role of Sex and Age
Research shows that females are more prone to knee ligament injuries than males due to differences in anatomy, form, and hormones such as estrogen and relaxin. Additionally, age plays a role in knee ligament injuries, with individuals over 50 years old being at a higher risk due to decreased muscle strength and flexibility.
Sports and Injuries
Knee ligament injuries are common in sports that require sudden stops and changes in direction such as soccer, basketball, and football (soccer). Injury prevention programs that include warm-up, neuromuscular training, and proprioception exercises can reduce the frequency of knee ligament injuries by up to 50%. Coaches and athletes should also prioritize proper technique, posture, and fatigue management to prevent knee ligament injuries.
In conclusion, knee ligament injuries are common among athletes and individuals who engage in physical activities. Understanding the common types and causes of knee ligament injuries, identifying symptoms and diagnosing the injury, and following proper treatment and rehabilitation options can help prevent long-term damage. Coaches, athletes, and individuals should prioritize injury prevention programs and proper technique to reduce the frequency of knee ligament injuries.
Prevention Strategies for Knee Ligament Injuries
When it comes to knee ligament injuries, prevention is key. Here are some effective strategies that we recommend:
Strengthening and Conditioning
Strengthening and conditioning exercises can help improve muscle strength and endurance, which can help reduce the risk of knee ligament injuries. Exercises that target the hips, ankles, and core can be particularly effective in improving stability and reducing the risk of injury.
Injury Prevention Programs
Injury prevention programs can be an effective way to reduce the risk of knee ligament injuries. These programs typically include a combination of warm-up exercises, neuromuscular training, and strength and conditioning exercises. They can be particularly effective for athletes who participate in high-risk sports, such as soccer, basketball, and football.
Importance of Compliance and Frequency
Injury prevention strategies are only effective if they are followed consistently and frequently. Compliance with injury prevention programs is essential for reducing the risk of knee ligament injuries. It is important to follow the program as prescribed and to make sure that exercises are performed correctly and with good form.
In conclusion, preventing knee ligament injuries requires a combination of strategies that target strength, stability, and flexibility. Injury prevention programs that incorporate warm-up exercises, neuromuscular training, and strength and conditioning exercises can be particularly effective. However, compliance with these programs is essential for success. By following these strategies, we can help reduce the risk of knee ligament injuries and keep athletes healthy and active.
Rehabilitation Exercises for Knee Ligaments: Strengthening and Recovery Techniques
As physical therapists, we often see patients with knee ligament injuries. Knee ligaments are strong bands of tissue that connect the thighbone to the shinbone and provide stability to the knee joint. Injuries to knee ligaments can result in pain, swelling, and decreased range of motion. Rehabilitation exercises for knee ligaments can help improve joint stability, reduce pain, and restore function.
Understanding Knee Ligament Injuries is important for developing an effective rehabilitation plan. There are four main ligaments in the knee joint: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). ACL and PCL injuries are more common in athletes and can occur during sports that involve sudden stops, changes in direction, or jumping. MCL and LCL injuries can result from a direct blow to the knee or from twisting the knee. Depending on the severity of the injury, surgery may be required to repair or reconstruct the damaged ligament.
In this article, we will discuss 6 Rehabilitation Exercises for Knee Ligaments that can help improve joint stability, reduce pain, and restore function. These exercises are designed to strengthen the muscles that support the knee joint and improve biomechanical function. By following a structured rehabilitation program, patients can improve their recovery and return to their daily activities faster.
Key Takeaways
Knee ligament injuries can result in pain, swelling, and decreased range of motion.
There are four main ligaments in the knee joint: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL).
Rehabilitation exercises for knee ligaments can help improve joint stability, reduce pain, and restore function.
Understanding Knee Ligament Injuries
Knee ligament injuries are common among athletes and individuals who engage in physical activities. These injuries can be caused by a wide range of factors, including trauma, overuse, and sports-related injuries. The most common types of knee ligament injuries include anterior cruciate ligament (ACL) injuries, medial collateral ligament (MCL) injuries, and posterior cruciate ligament (PCL) injuries.
Causes and Types of Injuries
ACL injuries are typically caused by a twisting motion or a direct blow to the knee. MCL injuries, on the other hand, are often caused by a direct blow to the outside of the knee. PCL injuries are usually the result of a direct blow to the front of the knee or a hyperextension injury.
Ligament injuries can be classified as either partial or complete tears. Partial tears involve damage to a portion of the ligament, while complete tears involve a complete separation of the ligament from the bone. Overuse injuries, such as tendinitis, can also occur in the knee.
Diagnosis and Assessment
Diagnosis of knee ligament injuries involves a physical examination, imaging tests, and other diagnostic procedures. Physical examination involves assessing the knee for pain, swelling, and instability. Imaging tests such as magnetic resonance imaging (MRI), radiographs, and ultrasound can also be used to assess the extent of the injury.
Treatment Options
Treatment options for knee ligament injuries depend on the severity of the injury. Nonoperative treatment may involve rest, ice, compression, and elevation (RICE), physical therapy, and immobilization. Operative treatment may involve surgery, such as arthroscopy or ACL reconstruction.
Post-Injury Challenges
Post-injury challenges may include pain, swelling, and instability. Rehabilitation is essential for restoring full function and reducing the risk of future injuries.
Understanding the Rehabilitation Process
Rehabilitation is an essential part of the recovery process for knee ligament injuries. The rehabilitation process involves a series of exercises and other interventions designed to improve muscle strength, proprioception, and joint stability.
Specific Rehabilitation Exercises
Specific rehabilitation exercises may include exercises to improve muscle strength, such as knee flexion and extension exercises, as well as exercises to improve proprioception, such as balance training.
Role of Imaging in Rehabilitation
Imaging tests such as MRI and radiographs can be used to assess the extent of the injury and monitor progress during rehabilitation.
Rehabilitation Exercises for Knee Ligament Recovery
Exercise
Description
Target Area
Passive Range of Motion
Gentle movements of knee by therapist/device to improve flexion/extension early post-injury without overstressing
Restore mobility; reduce stiffness
Quad Sets
Contract quad muscles by pushing knees down into floor/table when in sitting/lying position
Activate quads; prevent atrophy
Straight Leg Raises
Tighten quads to lift straight leg up off floor/bed, keep knee locked
Strengthen quads; knee stabilization
Hip Abduction/Adduction
Move legs outward/inward against resistance or body weight
Strengthen hip muscles supporting knee
Calf Raises
Raise up onto ball/toes of foot, lower with control
Strengthen calves; improve balance/proprioception
Wall Sits
Slide down wall until knees/hips at 90 degree angle, hold position
Strengthen quads; improve endurance
Terminal Knee Extensions
Sit with resistance band around foot, fully straighten knee
Regain full extension range of motion
Hamstring Curls
Flex knees to pull heels toward buttress against resistance band
Strengthen hamstrings; decelerate knee extension
Balance Board/Wobble Board
Stand with knee slightly bent on unstable surface
Enhance balance and knee proprioception
Mini-Squats
Perform slight squatting motion within pain-free range of motion
Regain quad control; restore movement pattern
The exact exercises and progressions are tailored by physical therapists depending on injury specifics, graft type, and post-surgical timeline. The goal is to restore strength, mobility, proprioception and movement control safely based on healing constraints
In conclusion, knee ligament injuries are common among athletes and individuals who engage in physical activities. Proper diagnosis, treatment, and rehabilitation are essential for restoring full function and reducing the risk of future injuries.
Anterior cruciate ligament (ACL) reconstruction is a common surgical procedure for individuals who have suffered a torn ACL. While outcomes have improved dramatically, knee pain and re-injury continue to be concerns during the recovery process. Recent advances in rehabilitation protocols and biomechanical research are shedding light on optimal recovery strategies.
Knee pain following ACL reconstruction arises due to multiple interrelated biomechanical and physiological factors. The initial trauma of surgery triggers an inflammatory response which can lead to fluid buildup, swelling, and stiffness, resulting in pain with movement. This acute inflammatory phase usually lasts 6-8 weeks. Concurrently, muscular imbalances around the knee joint develop, most notably quadriceps inhibition and weakness. The quadriceps muscles play a crucial role in stabilizing the knee joint. When weakened and inhibited after surgery, abnormal forces are transmitted through the joint, exacerbating pain and dysfunction. Finally, biomechanical alterations including asymmetric gait patterns and improper landing mechanics cause further pain. A careful evaluation of all these contributing trigger points through a full physical therapy examination is key to pinpointing the optimal treatment approach.
Causes of Knee Pain
Knee pain following ACL reconstruction arises due to multiple interrelated biomechanical and physiological factors. The initial trauma of surgery triggers an inflammatory response which can lead to fluid buildup, swelling, and stiffness, resulting in pain with movement.
Inflammation
This acute inflammatory phase usually lasts 6-8 weeks.
A 2022 study found that altered walking biomechanics were present even 2 years after surgery, especially in females (Smith et al). These persistent abnormalities highlight the need for rehabilitation focused on normalizing movement patterns.
Effective knee pain management requires a multifaceted rehabilitation program tailored to the individual’s specific deficits and dysfunctions. The priority initially is controlling inflammation through ice, compression, medication, and activity modification. Once pain and swelling have been reined in, restoring full knee mobility is essential for reducing stiffness and dysfunction. Gentle manual therapy techniques and range of motion exercises facilitate this process. As mobility improves, muscular imbalances must be addressed through targeted stretching and progressive strength training, focused especially on reactivating the quadriceps. Finally, movement pattern retraining helps ingrain proper mechanics. Areas to emphasize include squatting, lunging, walking gait, running, jumping and landing. The goal is to eliminate any asymmetries or compensations that could lead to abnormal forces through the joint. Throughout this process, communication with the care team is key to calibrate the program to avoid flare-ups while still stimulating progress.
Anti-inflammatory medications
Ice, compression, elevation
Restoring range of motion
Eliminating muscle imbalances
Normalizing movement patterns
2: Rehabilitation Phases and Focus Areas
Phase
Timing
Goals
Inflammation & Early ROM
0-2 weeks
– Manage swelling/pain<br>- Regain mobility
Intermediate ROM & Early Strengthening
3-6 weeks
– Improve quad strength<br>- Single leg stability
Advanced Strengthening & Neuromuscular Control
6-12 weeks
– Running mechanics<br>- Multi-plane agility
Return to Sport
4+ months
– Sport-specific training<br>- Confidence in knee function
Muscular Imbalances
Concurrently, muscular imbalances around the knee joint develop, most notably quadriceps inhibition and weakness. The quadriceps muscles play a crucial role in stabilizing the knee joint. When weakened and inhibited after surgery, abnormal forces are transmitted through the joint, exacerbating pain and dysfunction.
Biomechanical Changes
Finally, biomechanical alterations including asymmetric gait patterns and improper landing mechanics cause further pain. A careful evaluation of all these contributing trigger points through a full physical therapy examination is key to pinpointing the optimal treatment approach.
Managing Knee Pain
Rehabilitation Program
Effective knee pain management requires a multifaceted rehabilitation program tailored to the individual’s specific deficits and dysfunctions.
Early Phase
The priority initially is controlling inflammation through ice, compression, medication, and activity modification. Once pain and swelling have been reined in, restoring full knee mobility is essential for reducing stiffness and dysfunction. Gentle manual therapy techniques and range of motion exercises facilitate this process.
Later Phase
As mobility improves, muscular imbalances must be addressed through targeted stretching and progressive strength training, focused especially on reactivating the quadriceps.
Movement Retraining
Finally, movement pattern retraining helps ingrain proper mechanics. Areas to emphasize include squatting, lunging, walking gait, running, jumping and landing. The goal is to eliminate any asymmetries or compensations that could lead to abnormal forces through the joint. Throughout this process, communication with the care team is key to calibrate the program to avoid flare-ups while still stimulating progress.
Optimizing Long-Term Outcomes
Preventing Re-Injury
Due to the high risk of retear after ACL reconstruction, prevention of re-injury is paramount during recovery. Gradually building up strength and then progressing activity in a controlled manner based on specific objective criteria allows tissues to heal while regaining function.
As the graft incorporation stretches beyond 6 months, impact activities can be cautiously integrated. However, pivoting sports may need to wait 9 months or more. Maintaining quadriceps and core strength and allowing the full return of power and agility prior to discharge from therapy ensures the knee can withstand demands of sport. Sticking to activity guidelines, along with smart training periodization can optimize recovery even years after ACL surgery.
Unraveling the Mystery Behind Knee Discomfort: A Comprehensive Guide to Knee Pain Causes
Introduction
Knee pain is a common ailment that can significantly impact mobility and quality of life. Understanding the underlying causes of knee pain is crucial for effective treatment and prevention.
In this comprehensive guide, we will delve into the various causes of knee pain, exploring the biomechanics of the knee joint and the role of surrounding muscles and ligaments. We will discuss common knee pain conditions, diagnostic tests, and treatment options for specific knee pain causes.
Biomechanics of the Knee Joint
The knee joint is a complex structure that bears significant weight and facilitates movement. It consists of the thigh bone (femur), shinbone (tibia), kneecap (patella), and various ligaments, tendons, and cartilage.
Ligaments: Strong bands of connective tissue that connect bones and provide stability to the joint.
Tendons: Connect muscles to bones and transmit the force generated by muscle contraction.
Cartilage: Cushions the bones and prevents friction within the joint.
Common Knee Pain Conditions
Patellofemoral pain syndrome (PFPS): Pain caused by misalignment of the kneecap in the groove of the thigh bone.
Gout: Medication to reduce inflammation and prevent gout attacks.
Conclusion
Knee pain can arise from various causes, affecting individuals of all ages and activity levels. Understanding the underlying causes of knee pain is essential for proper diagnosis, treatment, and prevention. By consulting a healthcare professional and following their recommendations, you can effectively manage knee pain, improve mobility, and maintain overall joint health.
Common Knee Pain Conditions and Treatment Options
Condition
Treatment
Patellofemoral pain syndrome (PFPS)
Rest, ice, compression, elevation (RICE), strengthening exercises, and physical therapy.
Anterior cruciate ligament (ACL) tear
Surgical reconstruction of the ACL.
Meniscal tear
Rest, pain management, or surgical repair, depending on severity.
Osteoarthritis
Weight management, exercise, pain relievers, and joint injections.
Rheumatoid arthritis
Medication to manage inflammation and slow joint damage.
Gout
Medication to reduce inflammation and prevent gout attacks.