Organized sports participation among children aged 6–17 years: United States, 2020
Black LI, Terlizzi EP, Vahratian A. National Center for Health Statistics (US). Publication date: 08/11/2022. Series: data overview; No. 441
https://stacks.cdc.gov/view/cdc/119026
Take home message
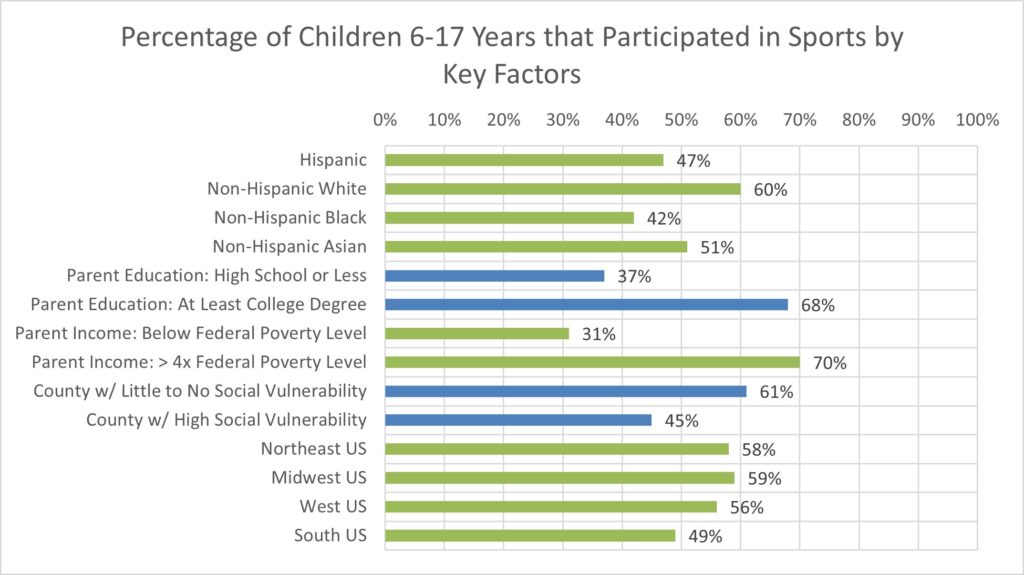
Sports participation was lower among racial and ethnic minority children, children whose parents had lower education or income, children living in counties with greater social vulnerability, and children living in the southern United States.
Background
Youth participation in sports is associated with better physical fitness and mental health. Understanding the differences in sports participation can help inform strategies to promote active lifestyles among children and adolescents, which positively impacts their physical and mental health.
Study aim
Black and colleagues completed an analysis of data from the 2020 National Health Interview Survey to describe disparities in sports participation in the United States.
Methods
The authors analyzed data from the 2020 National Health Interview Survey. This survey is a nationally representative household survey conducted throughout the year. Parents reported whether their child participated in a sports team or club or took sports lessons at school or in the community in the previous 12 months. The authors then collected data on household income as a percentage of the federal poverty level, race and Hispanic origin, geographic region (Northeast US, Midwest US, Southern US, or Western US), social vulnerability of a county, and urbanicity ( urban region). -national classification) of a province.
Results
About half (54%) of children aged 6 to 17 have played sports in the past twelve months (boys: 56%; girls: 52%). The authors reported: “Participation levels were lower among children from racial and ethnic minority groups, children whose parents had lower levels of education and family income, children living in counties with greater social vulnerability, and children living in the South.”
Viewpoints
The results of this letter provide a surprising snapshot of sports participation in the United States. While it is established that early sports participation can have a positive impact on an individual, significant differences still exist. These findings indicate that sports participation is strongly associated with socioeconomic status. Ultimately, a higher socio-economic status can ensure children’s access to sports. This is particularly reflected in the fact that lower parental education, lower parental income and lower geographical area of social vulnerability are all associated with lower participation. These findings complement data from the Athletic Training Locations and Services Database, which shows that these communities also have less access to athletic training services.
This data provided a unique snapshot of 2020, when many sports shut down in the spring due to the COVID-19 pandemic. The survey asked about sports participation over the past year, so it is unclear whether the pandemic could influence these results. Furthermore, not every community is recovering from the pandemic in the same way. The authors acknowledge that it will be essential to replicate these analyzes with data from the 2022 survey to better understand patterns of sports participation after many of the restrictions associated with the pandemic are relaxed/removed.
Clinical implications
Sports medicine professionals should advocate for increased access to sports through local recreation organizations, schools, and other organizations. In regions with high social vulnerability, we should encourage policymakers that investments in youth sports and physical activity can help improve community health.
Questions for discussion
What can we do as doctors to positively influence participation in team sports?
Written by: Kyle Harris
Review by: Jeffrey Driban
related posts
Asian Pacific Society of Cardiology Consensus Recommendations for Pre-Participation Screening in Young Competitive Athletes
A lasting impression: youth sports participation and healthy habits as adults
Previous participation in collision sports is associated with reduced quality of life
Lower socioeconomic status is associated with less access to athletic training services