Did you know that recent 2025 research found pain reduction from knee bracing after ACL reconstruction was nearly negligible, with a difference of just 0.08 on the pain scale? This highlights an important truth in 2026, the right hinged knee brace is less about quick pain relief and more about stability, confidence, and proper knee support.
Key Takeaways
Question
Answer
What is the best hinged knee brace for ACL support?
High-quality hinged braces like DonJoy Armor and Mueller Hinged Brace provide strong ligament stability for ACL injuries.
They can reduce strain, but full prevention depends on rehab and strength training.
Understanding ACL Injuries and Knee Stability
The ACL is one of the key ligaments that keeps your knee stable during movement. When it is injured, many people experience knee pain, instability, and a feeling that the knee might give out.
We often see that proper support during recovery can help people stay active safely. Hinged knee braces are designed to limit harmful motion while allowing controlled movement.
What Makes Hinged Knee Braces Effective for ACL Support
Hinged braces use metal or reinforced supports on each side of the knee. These hinges guide motion and prevent excessive twisting that can worsen injury.
In 2026, many designs focus on combining mobility with protection. This allows users to move naturally without increasing knee hurt or instability.
We selected these braces based on support level, comfort, and suitability for ACL recovery. Each option addresses different needs, from mild instability to post-surgical recovery.
1. DonJoy Armor Knee Brace
A high-performance brace designed for athletes and active users. It features anti-rotation straps and rigid support.
2. Mueller Hinged Knee Brace
A more affordable option with strong support for everyday use. It is commonly used for moderate knee pain and ligament injuries.
3. DonJoy FullForce ACL Brace
Lightweight yet supportive, ideal for sports and movement. It balances stability and flexibility.
4. Ossur Hinged Knee Brace
Known for comfort and anatomical fit. Suitable for long-term wear during recovery.
5. Shock Doctor Hinged Knee Brace
Provides compression and support for mild to moderate instability. Often used during activity.
A quick visual guide comparing the top 5 hinged knee braces for ACL support in 2026, highlighting features and ideal uses.
Did You Know?
Biomechanical data shows hinged knee bracing can reduce rotatory loads and ACL strain under specific conditions.
Choosing the right brace depends on your specific condition and activity level. Not every brace works the same for every knee.
We recommend considering the following:
Severity of ACL injury
Activity level
Comfort and fit
Doctor recommendations
When to Use a Hinged Knee Brace for Knee Pain
Hinged braces are most useful during movement and recovery phases. They are commonly used after ACL injuries or surgery.
They can also help when knee hurt occurs during walking, running, or sports. However, they should be part of a broader recovery plan.
Benefits and Limitations of Hinged Knee Braces
Hinged braces provide structure and support, but they are not a complete solution. Understanding both benefits and limits helps set realistic expectations.
Improved stability
Reduced risk of sudden movement
Support during activity
Limitations include limited impact on long-term strength or healing without proper rehab.
Did You Know?
Knee braces do not significantly affect thigh strength or range of motion up to 2 years after ACL reconstruction.
Common Knee Conditions That Benefit from Hinged Braces
Hinged braces are not limited to ACL injuries. They are also helpful in other knee conditions that affect stability.
Ligament injuries
Meniscus tears
Post-surgical recovery
Each condition may require a slightly different brace design and fit.
Tips for Wearing a Hinged Knee Brace Safely
Wearing your brace correctly is essential for getting the benefits. Poor fit or overuse can reduce effectiveness.
Ensure proper sizing
Avoid over-tightening
Follow medical advice
We always recommend consulting a healthcare professional if knee pain persists.
Hinged Knee Braces vs Other Knee Supports
Not all knee braces provide the same level of support. Hinged braces are typically used for more serious instability.
Brace Type
Best For
Hinged Brace
ACL and ligament injuries
Sleeve
Mild knee pain
Patellar Brace
Kneecap alignment
Conclusion
In 2026, hinged knee braces remain an important tool for managing ACL injuries and reducing knee pain during recovery. They provide stability and confidence, especially during movement.
At the same time, they work best when combined with proper rehabilitation and medical guidance. If your knee hurt persists or worsens, seeking professional advice is always the safest next step.
Our goal is to help you make informed decisions so you can support your knee health and return to daily activities with confidence.
Did you know that about 80.4% of people return to sport after ACL reconstruction, but only 54.6% reach their pre-injury level? Understanding ACL recovery and bracing is essential if your knee hurt or instability is holding you back.
Key Takeaways
Question
Answer
What is ACL recovery?
A structured process involving rest, rehab, and sometimes surgery to restore knee stability. Learn more in our ACL injury guide.
Do you need a knee brace after ACL surgery?
Not always, but bracing can support healing and reduce knee pain in early stages.
How long does recovery take?
Typically 6–12 months depending on severity and rehab consistency.
The ACL is one of the four major ligaments that stabilize the knee joint. When it tears, the knee becomes unstable, painful, and difficult to trust during movement.
ACL injuries often happen during sports that involve sudden direction changes. Many people feel a pop followed by swelling and immediate knee pain.
If untreated, instability can lead to long-term damage. This is why early diagnosis and proper recovery planning matter.
Common Symptoms During ACL Recovery
After injury or surgery, symptoms vary but often include swelling, stiffness, and reduced mobility. Many patients report that their knee hurt most during bending or weight-bearing.
Other signs include instability and difficulty returning to normal activities. These symptoms can overlap with other ligament injuries.
We often compare ACL symptoms with broader knee ligament injuries to better understand recovery challenges.
Phases of ACL Recovery Explained
Recovery typically progresses through stages, starting with swelling control and ending with return to sport. Each phase builds strength and stability in the knee.
Early rehab focuses on regaining motion. Later phases emphasize strength, balance, and confidence.
Phase 1: Pain and swelling control
Phase 2: Range of motion
Phase 3: Strength rebuilding
Phase 4: Functional training
Explore five essential facts about ACL recovery and bracing.
Do You Really Need a Knee Brace After ACL Surgery?
Knee braces are commonly used after ACL surgery to provide stability and protect the joint. However, not every patient needs one for the entire recovery period.
Some individuals benefit more from targeted rehab than prolonged bracing. The decision depends on your injury severity and activity level.
Did You Know?
Brace-free rehabilitation after ACL reconstruction showed similar outcomes to brace-based rehab at 1 year.
Modern ACL surgery often uses bioabsorbable screws. These help secure the graft while gradually dissolving over time.
This approach reduces the need for hardware removal. It also supports long-term healing of the knee joint.
When to Seek Help for Ongoing Knee Pain
If your knee hurt persists beyond expected recovery time, it may signal complications. Swelling, instability, or sharp pain should not be ignored.
We recommend early evaluation to prevent long-term damage. Addressing issues quickly improves outcomes.
Conclusion
ACL recovery and bracing require a balanced approach that combines protection, rehabilitation, and gradual return to activity. While braces can support healing, they are only one part of a complete recovery plan.
We encourage a structured rehab program, proper guidance, and patience. With the right strategy, most people can regain strength, reduce knee pain, and return to the activities they enjoy.
Knee ligaments are the unsung heroes of mobility, acting as strong fibrous connective tissues that bind bones together and provide crucial stability to your knee joint. When these ligaments weaken or become injured, everyday movements can become painful challenges. Fortunately, there are natural, non-invasive ways to strengthen these vital structures. This guide explores science-backed methods to strengthen knee ligaments naturally, helping you maintain mobility and prevent injuries without resorting to surgery or medications.
Understanding Knee Ligaments and Their Function
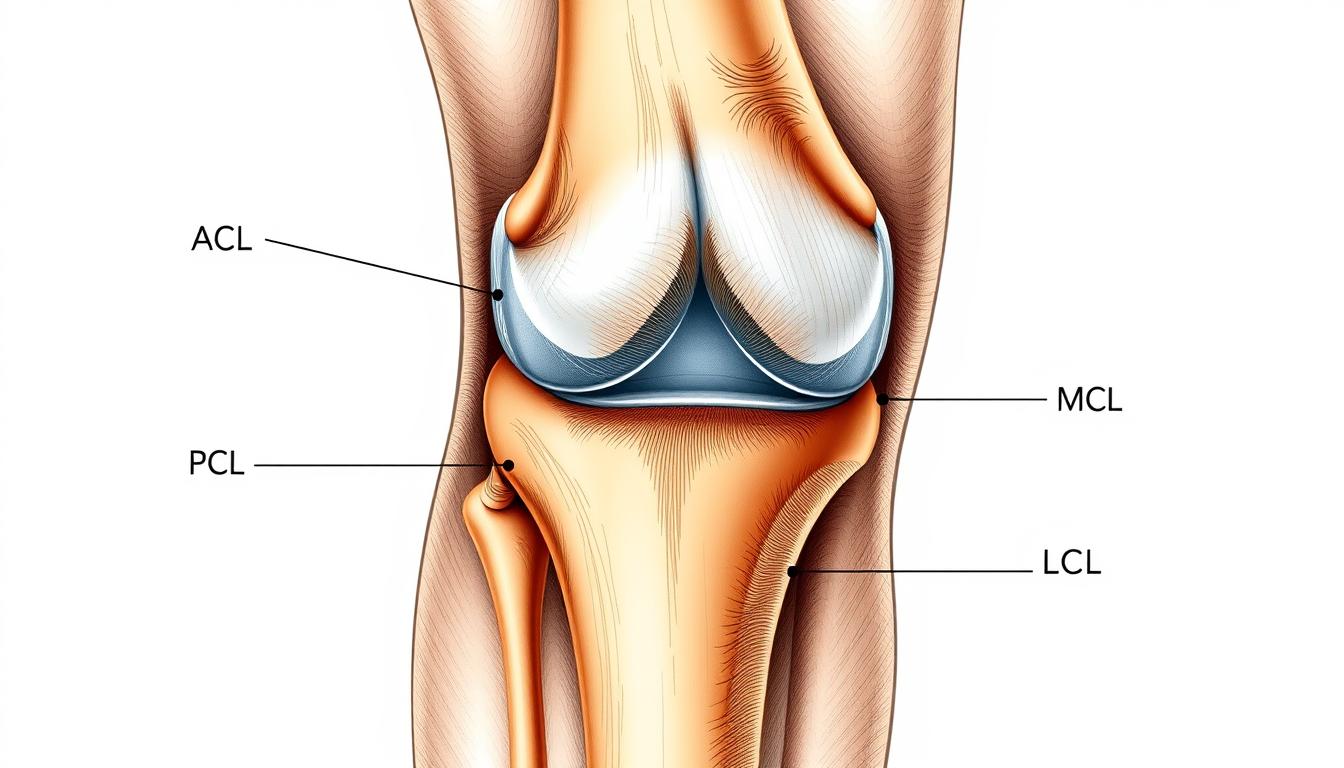
The four main ligaments of the knee provide stability in different directions.
Think of knee ligaments as nature’s stabilizing cables. Your knee has four main ligaments: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). Each plays a specific role in keeping your knee stable during different movements. When these ligaments are strong and healthy, they allow for smooth, pain-free motion while preventing excessive movement that could damage the joint.
Unlike muscles, ligaments have limited blood supply, which means they heal slowly after injury. This makes prevention and natural strengthening particularly important. By focusing on natural methods to strengthen knee ligaments, you can avoid the lengthy recovery times associated with ligament injuries and the potential complications of surgical interventions.
Targeted Exercises to Strengthen Knee Ligaments
The foundation of natural knee ligament strengthening lies in specific exercises that build the supporting muscles around the knee. Strong muscles take pressure off ligaments, providing better joint stability and reducing injury risk. Here are effective, low-impact exercises that research has shown to strengthen the knee complex:
1. Leg Lifts for Quadriceps Strength
Lie flat on your back on a comfortable surface.
Keep one leg straight and bend the other slightly at the knee.
Engage your core by pulling your belly button toward your spine.
Slowly lift the straight leg about 12 inches off the floor without bending the knee.
Hold for 5 seconds, then slowly lower.
Complete 3 sets of 10 repetitions for each leg.
This exercise strengthens the quadriceps, which are crucial for knee stability. A 2019 study in the Journal of Exercise Rehabilitation found that straight leg raises significantly improved knee function in patients with knee osteoarthritis.
2. Standing Hamstring Curls
Stand straight with feet hip-width apart, holding onto a chair or wall for balance.
Slowly bend one knee, bringing your heel toward your buttocks.
Keep your thighs aligned and knees close together.
Hold for 5 seconds at the top of the movement.
Lower slowly and repeat 10 times before switching legs.
Complete 3 sets for each leg.
This exercise targets the hamstrings, which work in tandem with the ACL to prevent forward sliding of the tibia (shin bone). Research published in the American Journal of Sports Medicine indicates that balanced hamstring-to-quadriceps strength ratios reduce ACL injury risk.
3. Wall Squats for Overall Knee Stability
Stand with your back against a wall, feet about 24 inches away from the wall.
Slowly slide your back down until your knees are bent at approximately 90 degrees.
Ensure your knees don’t extend past your toes.
Hold this position for 5-10 seconds.
Slowly slide back up to the starting position.
Repeat 10 times for 2-3 sets.
Wall squats build strength in multiple muscle groups that support the knee joint. A controlled environment reduces the risk of improper form that could stress ligaments.
4. Resistance Band Exercises
Resistance bands provide an excellent way to strengthen the muscles around the knee without putting excessive stress on the joint. The “monster walk” is particularly effective:
Place a resistance band just above your ankles or knees.
Stand with feet hip-width apart, knees slightly bent.
Step sideways while maintaining tension in the band.
Take 10-15 steps in one direction, then reverse.
Complete 3 sets in each direction.
A study in the Journal of Physical Therapy Science found that resistance band exercises significantly improved knee stability in patients with mild knee osteoarthritis by strengthening the hip abductors that support proper knee alignment.
Nutrition for Ligament Health
What you eat plays a crucial role in maintaining and strengthening knee ligaments. Certain nutrients are particularly important for ligament health:
Collagen-Rich Foods
Ligaments are primarily made of collagen, so consuming collagen-rich foods can help provide the building blocks needed for repair and strengthening. Include these in your diet:
Bone broth (simmered for at least 12 hours to extract collagen)
Chicken skin and cartilage
Fish with edible bones (sardines, salmon)
Pork or beef tendon
Vitamin C for Collagen Synthesis
Vitamin C is essential for collagen production. Without adequate vitamin C, your body cannot effectively create new collagen. Research published in the Journal of Biological Chemistry confirms vitamin C’s critical role in collagen synthesis. Include these vitamin C-rich foods:
Citrus fruits (oranges, grapefruits, lemons)
Bell peppers
Strawberries
Kiwi
Broccoli
Omega-3 Fatty Acids for Inflammation Control
Omega-3 fatty acids help reduce inflammation that can damage ligaments over time. A study in the Journal of the American College of Nutrition found that omega-3 supplementation reduced joint pain and increased grip strength in patients with rheumatoid arthritis. Good sources include:
Fatty fish (salmon, mackerel, sardines)
Walnuts
Flaxseeds and chia seeds
Algal oil (plant-based option)
Hydration for Ligament Function
Water makes up about 70% of ligament tissue. Dehydration can make ligaments less elastic and more prone to injury. Aim to drink at least 8 glasses of water daily, more if you’re active or in hot weather. A study in the Journal of Athletic Training found that even mild dehydration negatively affected joint proprioception, potentially increasing injury risk.
Lifestyle Adjustments for Stronger Knee Ligaments
Weight Management
Excess weight places additional stress on knee ligaments. Research published in Arthritis & Rheumatism found that for every pound of weight loss, there is a four-pound reduction in knee joint load. Maintaining a healthy weight through balanced nutrition and regular exercise significantly reduces strain on knee ligaments.
Proper Posture and Alignment
Poor posture doesn’t just affect your back—it changes how weight is distributed through your knees. Practice these alignment principles:
Keep knees in line with toes when squatting or climbing stairs
Avoid sitting with legs crossed for extended periods
Use proper form during all exercises
Consider consulting with a physical therapist for personalized posture correction
Appropriate Footwear
Shoes with proper support help maintain correct knee alignment. A study in the Journal of Foot and Ankle Research found that appropriate footwear can reduce knee adduction moment, a key factor in knee osteoarthritis progression. Look for shoes with:
Good arch support
Cushioning for shock absorption
Proper fit (not too tight or too loose)
Replacement every 300-500 miles if used for running
Avoiding High-Risk Activities
While staying active is important, certain activities place excessive stress on knee ligaments. Consider limiting or modifying:
Deep squats with heavy weights
High-impact activities on hard surfaces
Sudden direction changes in sports without proper training
Excessive downhill running
Instead, incorporate low-impact activities like swimming, cycling, or elliptical training that strengthen muscles without stressing ligaments.
Natural Supplements for Ligament Support
Certain supplements may help strengthen knee ligaments naturally. Always consult with a healthcare provider before starting any supplement regimen, especially if you have existing health conditions or take medications.
Turmeric (Curcumin)
Turmeric contains curcumin, a compound with powerful anti-inflammatory properties. A 2016 systematic review published in the Journal of Medicinal Food found that turmeric extract was as effective as ibuprofen for knee osteoarthritis pain. Typical dosage: 500-1000mg of curcumin daily, preferably with black pepper extract (piperine) to enhance absorption.
Ginger
Like turmeric, ginger has anti-inflammatory properties that may help reduce knee pain and improve function. Research in Arthritis & Rheumatism showed that ginger extract reduced pain and stiffness in people with osteoarthritis. Typical dosage: 250-500mg, 2-3 times daily.
Glucosamine and Chondroitin
These compounds are natural components of cartilage. While research results are mixed, some studies suggest they may help maintain joint health and reduce pain, particularly when taken together. A large-scale study called GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial) found that the combination helped people with moderate-to-severe knee pain. Typical dosage: 1500mg glucosamine and 1200mg chondroitin daily.
Collagen Supplements
Hydrolyzed collagen supplements may support ligament health. A 2017 review in the Journal of Sports Science & Medicine found that collagen peptide supplementation improved joint pain and function in athletes. Typical dosage: 10-15g daily.
Important: Supplements are not regulated as strictly as medications. Choose products from reputable manufacturers, and always discuss supplement use with your healthcare provider, especially if you have existing health conditions or take medications.
Precautions and When to Seek Professional Help
While natural methods can be effective for strengthening knee ligaments, it’s important to approach them with caution and know when professional help is needed.
Warning Signs That Require Medical Attention
Sudden, severe pain following an injury
Audible popping sound at the time of injury
Inability to bear weight on the affected leg
Visible deformity or significant swelling
Joint instability or feeling that the knee “gives way”
Pain that persists or worsens despite rest and home treatment
Avoiding Overexertion
When strengthening knee ligaments, more is not always better. Overexertion can lead to injury or worsen existing conditions. Follow these guidelines:
Start with low intensity and gradually increase
Allow 48 hours of recovery between strength training sessions for the same muscle groups
Listen to your body—pain beyond mild muscle soreness is a warning sign
Modify exercises if they cause pain
The Value of Professional Guidance
A physical therapist or sports medicine specialist can provide:
Personalized exercise programs based on your specific needs
Proper technique instruction to maximize benefits and prevent injury
Progressive advancement of exercises as your strength improves
Complementary treatments like manual therapy or taping techniques
Get Personalized Knee Strengthening Guidance
For a customized program tailored to your specific knee condition, consider consulting with a physical therapist who specializes in knee rehabilitation.
Creating a sustainable routine is key to strengthening knee ligaments naturally. Here’s a sample 8-week plan that incorporates all the elements discussed:
Weeks 1-2: Foundation Building
Exercise: 2-3 days per week of basic exercises (leg lifts, wall sits) with low repetitions
Nutrition: Begin incorporating collagen-rich foods and increase water intake
Lifestyle: Assess and correct posture during daily activities
Weeks 3-4: Progressive Development
Exercise: Increase to 3-4 days per week, add resistance band exercises
Nutrition: Add vitamin C-rich foods to enhance collagen synthesis
Supplements: Consider introducing one supplement (after consulting healthcare provider)
Weeks 5-6: Advancing Strength
Exercise: Increase repetitions and sets, add more challenging variations
Nutrition: Ensure balanced intake of all supportive nutrients
Lifestyle: Implement proper footwear and activity modifications
Weeks 7-8: Maintenance and Progress
Exercise: Full program 3-4 days per week with appropriate progression
Evaluation: Assess improvements in pain, stability, and function
Adjustment: Modify program based on progress and challenges
“Consistency, not intensity, is the key to strengthening knee ligaments naturally. Small, regular efforts yield greater results than occasional intense sessions.”
— Dr. Robert Wilson, Sports Medicine Specialist
Conclusion: The Path to Stronger Knee Ligaments
Strengthening knee ligaments naturally is a journey that combines targeted exercises, proper nutrition, lifestyle adjustments, and potentially beneficial supplements. By taking a comprehensive approach, you can improve knee stability, reduce pain, and enhance your overall quality of life without resorting to invasive procedures.
Remember that natural strengthening takes time—ligaments respond slowly to interventions due to their limited blood supply. Be patient with your progress and consistent with your efforts. Small improvements add up to significant changes over time.
Most importantly, listen to your body throughout this process. Pain is a signal that something isn’t right. If you experience persistent or worsening pain, consult with a healthcare professional for personalized guidance.
By implementing the science-backed methods outlined in this guide, you’re taking an important step toward healthier, stronger knee ligaments that will support your mobility and active lifestyle for years to come.
Ready to Start Your Knee Strengthening Journey?
Download our free printable exercise guide with detailed instructions and progress tracking tools.
How long does it take to strengthen knee ligaments naturally?
Ligaments respond more slowly than muscles due to their limited blood supply. Most people begin to notice improvements in knee stability and reduced pain after 6-8 weeks of consistent exercise and proper nutrition. However, significant strengthening may take 3-6 months of dedicated effort. Individual results vary based on age, overall health, and the current condition of your ligaments.
Can damaged knee ligaments heal completely without surgery?
Minor ligament sprains (Grade I and some Grade II injuries) can often heal without surgery through proper rest, rehabilitation exercises, and natural strengthening methods. However, complete tears (Grade III injuries) typically require surgical intervention. Always consult with a healthcare provider for proper diagnosis and treatment recommendations for ligament injuries.
Is it safe to strengthen knee ligaments naturally if I already have knee pain?
Mild to moderate knee pain can often improve with appropriate strengthening exercises. However, you should first get a proper diagnosis from a healthcare provider to understand the cause of your pain. They can recommend specific exercises that are safe for your condition. Never push through sharp or increasing pain during exercises, as this could indicate you’re causing further damage.
Did you know that the hormonal changes during pregnancy can affect the stability of your knee joints, potentially leading to long-term issues after childbirth? Many women experience changes in their bodies after giving birth, and one common issue is joint laxity. During pregnancy, hormones cause ligaments to relax, which can impact the stability of joints, including the knees.
Understanding postpartumknee issues is crucial for new mothers who want to safely return to their pre-pregnancy activities. We’ll explore how these changes occur and what can be done to manage knee instability.
Key Takeaways
Pregnancy hormones can cause knee joint instability.
Understanding postpartum knee changes is crucial for new mothers.
Managing knee instability is key to returning to pre-pregnancy activities.
Ligament laxity during pregnancy can lead to long-term knee issues.
New mothers can take steps to safely recover and strengthen their knee joints.
Understanding Postpartum Knee Ligament Laxity
After giving birth, women may experience knee ligament laxity, a condition characterized by loose ligaments in the knee joint. This condition is a result of the significant changes that occur in a woman’s body during pregnancy.
What Happens to Your Knee Joints After Pregnancy
During pregnancy, the body undergoes numerous changes to prepare for childbirth. One of these changes involves the release of hormones such as estrogen and relaxin, which increase flexibility and remodeling of collagen in the knees and other joints. As Dr. Jane Smith, an orthopedic specialist, notes, “The increased levels of these hormones can lead to ligament laxity, making the knee joint less stable.”
This instability can persist into the postpartum period, affecting women’s mobility and comfort.
Common Symptoms and Experiences
Many new mothers report feeling unstable in their knees when performing everyday activities like walking or climbing stairs. Common symptoms include feelings of “giving way” in the knee joint, clicking or popping sensations, and pain along the joint line or behind the kneecap.
As one new mother shared,
“I felt like my knee was going to give out on me every time I stood up with my baby.”
The intensity of these symptoms can vary widely among women, with some experiencing mild instability while others face significant functional limitations due to knee pain and laxity.
It’s essential for women to be aware of these symptoms and seek appropriate care to prevent long-term issues.
The Science Behind Pregnancy-Related Joint Changes
Understanding the science behind pregnancy-related joint changes is crucial for new mothers. During pregnancy, a woman’s body undergoes numerous transformations that affect various physiological systems.
Hormonal Influences on Ligament Structure
The hormone relaxin plays a significant role in pregnancy-related joint changes. It is produced by the ovaries and placenta during pregnancy and helps relax the pelvic muscles and ligaments, allowing for an easier childbirth. However, this increased ligament laxity can also affect other joints, including the knees.
As Dr. Sarah Jones, an obstetrician, notes,
“The effects of relaxin are not limited to the pelvic area; it can cause a general increase in ligament laxity, potentially leading to knee instability.”
This hormonal influence on ligament structure is a key factor in understanding postpartum knee ligament laxity.
Hormone
Effect on Ligaments
Impact on Knee Joint
Relaxin
Increased laxity
Potential instability
Progesterone
Relaxation of smooth muscle
Indirect effects on joint stability
Estrogen
Effects on collagen synthesis
Possible influence on ligament strength
Biomechanical Alterations During Pregnancy
As pregnancy progresses, significant biomechanical changes occur that directly impact knee joint loading and function. The growing uterus shifts a woman’s center of gravity forward, altering posture and creating compensatory changes in the lower extremity alignment.
Weight gain during pregnancy increases the load on weight-bearing joints, with the knees experiencing forces up to 3-4 times body weight during activities like stair climbing. Many pregnant women develop an increased lumbar lordosis (swayback) and anterior pelvic tilt, which changes the alignment of the entire lower kinetic chain, including the knees.
These postural adaptations, combined with ligamentous laxity, often lead to altered movement patterns that may persist into the postpartum period. Research shows that pregnant women often develop a wider stance and altered gait mechanics, including decreased stride length and increased double support time.
The combination of increased joint laxity and altered biomechanics creates a perfect storm for potential knee instability that can continue after delivery. Understanding these biomechanical changes is essential for developing effective rehabilitation strategies that address not just the knee joint itself but the entire kinetic chain.
Research Findings on 31. Postpartum Knee Ligament Laxity
Studies examining postpartum knee ligament laxity have provided valuable information on the differences between women experiencing their first pregnancy and those who have had multiple pregnancies. We will explore these findings in detail, shedding light on the current state of knowledge regarding this condition.
Key Studies and Their Conclusions
Research has identified that knee ligament laxity is a significant concern during and after pregnancy. A key study found that joints with increased laxity may not fully return to pre-pregnancy values after the first pregnancy. This suggests that the first pregnancy could be a critical period for establishing a new baseline of joint laxity for many women.
Some of the notable findings include:
First-time mothers often experience more dramatic changes in joint laxity during pregnancy.
Multiparous women may develop laxity more rapidly during subsequent pregnancies.
Some degree of joint laxity may persist after the first pregnancy.
Differences Between Primiparous and Multiparous Women
The differences in how knee ligament laxity manifests between primiparous and multiparous women are significant. We observe that:
Primiparous women showed increased anterior knee laxity postpartum.
Multiparous women demonstrated a different pattern, with less significant changes in anterior knee laxity.
Both groups showed decreased posterior and varus-valgus laxity postpartum, indicating some consistent recovery mechanisms.
Understanding these differences is crucial for developing targeted interventions and treatment plans that cater to the specific needs of women based on their pregnancy history. By acknowledging these variations, healthcare providers can offer more personalized care to women experiencing postpartum knee ligament laxity.
Timeline of Knee Joint Recovery After Childbirth
The postpartum period is marked by significant changes in knee joint laxity, with recovery being a prolonged process. As we explore the timeline of knee joint recovery after childbirth, it’s essential to understand the various stages involved.
First Trimester to Delivery
During pregnancy, particularly from the first trimester to delivery, the body undergoes substantial hormonal changes that affect ligament laxity. Hormonal influences, such as the increase in relaxin, lead to increased joint compliance. This period is crucial as it sets the stage for the postpartum recovery process.
Immediate Postpartum Period (0-6 Weeks)
In the immediate postpartum period, the body begins its natural recovery process. Although hormone levels start to normalize, significant changes in knee joint laxity can still be observed. Research indicates that at 4-5 months postpartum, many women still experience knee joint laxity.
Extended Recovery (3-5 Months)
The extended recovery period, spanning from 3 to 5 months postpartum, is critical for rehabilitation. It’s during this time that targeted strengthening exercises can significantly impact recovery. Studies have shown that by 19 weeks postpartum, many aspects of knee joint laxity decrease from early pregnancy levels.
Postpartum Period
Knee Joint Laxity Changes
0-6 Weeks
Initial recovery phase, hormone levels normalize
3-5 Months
Significant improvements in knee joint stability
4-5 Months
Noticeable decrease in knee joint laxity
Understanding the recovery timeline helps new mothers set realistic expectations and engage in appropriate rehabilitation strategies. By acknowledging that full tissue recovery takes months rather than weeks, women can better navigate their postpartum journey.
Assessing Your Knee Joint Health
Postpartum knee joint health assessment is a critical step in maintaining overall well-being after pregnancy. As your body recovers from childbirth, it’s essential to monitor your knee joint health to identify any potential issues early on.
Self-Evaluation Techniques
Begin by performing simple self-evaluation techniques to assess your knee joint health. Pay attention to any pain or discomfort in your knees during daily activities like carrying your baby, walking, or climbing stairs. Notice if you experience any swelling, catching, or locking of the knee joint.
You can also check for knee instability by performing gentle movements and assessing your ability to perform tasks without experiencing significant discomfort.
When to Seek Professional Assessment
If you experience persistent knee pain that doesn’t improve within 2-3 weeks of gentle self-management, it’s time to seek professional assessment. Other signs that warrant professional evaluation include significant swelling, catching, locking, or giving way of the knee joint during normal daily activities.
If you’re unable to perform essential caregiving tasks due to knee instability, consider consulting a healthcare provider.
Women with a history of previous knee injuries or surgeries should seek earlier professional guidance for any new postpartum knee symptoms.
A proper professional assessment should include evaluation of not just the knee joint itself but also hip strength, pelvic alignment, and foot mechanics.
Early intervention typically leads to faster resolution of symptoms, so don’t delay seeking help if you experience any concerning symptoms.
The Connection Between Pelvic Floor and Knee Stability
Understanding the link between pelvic floor dysfunction and knee instability is crucial for effective postpartum recovery. During pregnancy and childbirth, the body undergoes significant changes that can affect both the pelvic floor and knee joints.
The pelvic floor and knee joints are interconnected through the kinetic chain. When the pelvic floor is dysfunctional, it can lead to instability and affect the entire lower extremity, including the knees.
How Pelvic Floor Dysfunction Affects Knee Joints
Pelvic floor dysfunction can lead to issues such as incontinence and pelvic pain, but its effects can also be seen in the stability of the knee joints. Research has shown that women with pelvic floor dysfunction are more likely to experience knee instability due to altered biomechanics and muscle imbalances.
Integrated Approach to Recovery
An effective postpartum recovery program must address both pelvic floor rehabilitation and knee stability exercise. By integrating these two aspects, women can achieve better outcomes in terms of overall movement quality and lower extremity function. We recommend starting with restoring proper breathing patterns and pelvic floor activation, creating a foundation of core stability that supports proper knee alignment.
Women who follow this integrated rehabilitation approach typically report faster resolution of both pelvic floor symptoms and knee instability. This holistic strategy recognizes that the body functions as an interconnected system and that postpartum recovery must address these connections for optimal outcomes.
Early Postpartum Knee Support Strategies
During the early postpartum period, supporting our knee health is crucial for new mothers. The changes experienced during pregnancy and childbirth can affect knee stability, making it essential to adopt supportive strategies.
Proper Body Mechanics
Using proper body mechanics is vital for reducing stress on the knee joint. When rising from a sitting position, it’s helpful to scoot to the edge of the chair, position feet slightly behind knees, and use arm support to minimize shear forces on the knee.
When climbing stairs, leading with the stronger leg going up and the affected leg going down can reduce stress on unstable knees. This technique, often remembered by “up with the good,” can be particularly helpful in the early postpartum period.
Supportive Devices and Braces
Utilizing supportive devices or braces can provide additional stability for the knee. These tools can be especially useful during activities that challenge knee stability, such as walking on uneven surfaces or engaging in physical movement.
Daily Movement Modifications
Modifying daily movements can protect vulnerable knee joints while allowing for necessary activities and gradual strengthening. For example, adopting a slightly wider stance during standing activities can improve stability.
Take smaller, more controlled steps when walking to challenge knee stability less.
Be strategic about the timing of more demanding activities to avoid fatigue.
Consider rearranging your living space to minimize stair climbing if knee instability is significant.
By implementing these strategies, new mothers can protect their knee health during the postpartum recovery period, ensuring a stronger foundation for future physical activities.
Gentle Rehabilitation Exercises: Weeks 0-4
Gentle rehabilitation exercises are essential in the early stages of postpartum recovery. These exercises help in regaining strength and stability, particularly in the knee area, which is crucial for new mothers.
Isometric Strengthening Exercises
Isometric exercises are beneficial during the initial weeks as they don’t involve significant movement. For example, contracting the quadriceps muscles without moving the knee joint helps strengthen the surrounding muscles. This can be done by tightening the thigh muscles while keeping the leg straight.
Range of Motion Activities
Gentle range of motion activities help maintain flexibility. Simple actions like straightening and bending the knee, or rotating the ankle, can be performed. These activities should be done carefully to avoid straining the knee.
Proper Walking Techniques
Reestablishing proper walking mechanics is crucial. Start with short walks on level surfaces, focusing on quality over distance. Maintain a comfortable stride and engage your core gently with each step to support proper knee alignment. Focus on a heel-to-toe rolling motion and keep your knees in line with your toes to avoid excessive stress. Gradually increase walking duration while maintaining proper gaittechniques.
By incorporating these gentle rehabilitation exercises and proper walkingtechniques, new mothers can significantly improve their recovery during the first four weeks postpartum.
Progressive Strengthening: Weeks 5-12
Progressive strengthening between weeks 5 and 12 postpartum is crucial for enhancing knee stability and overall lower body strength. During this period, we can introduce more challenging exercises to our routine, focusing on core and lower body stability.
Core and Lower Body Stability Exercises
Exercises that target the core and lower body are essential for improving knee stability. Examples include squats, lunges, and leg press exercises. These exercises should be performed with proper form and technique to avoid putting unnecessary strain on the knee joint. We recommend starting with bodyweight exercises and gradually progressing to weighted exercises as tolerated.
Resistance Training Guidelines
When engaging in resistance training, it’s essential to follow specific guidelines to ensure safe and effective progression. Muscular strength tasks involving repetitions of 8-12 with weights as tolerated are recommended. This approach helps in strengthening the muscles around the knee without overloading the joint.
Monitoring Symptoms During Exercise
Careful monitoring of symptoms during this progressive phase is crucial. We should be aware of any increase in pain or symptoms and adjust our exercise program accordingly. The “24-hour rule” is a useful guideline: if pain or swelling increases during exercise or persists for more than 24 hours afterward, we should reduce the intensity or modify the exercise. Additionally, watching for signs of knee instability, such as the knee “giving way,” and monitoring for clicking, catching, or locking sensations in the knee joint can help identify potential issues early.
By being mindful of our body’s response to different types of exercise and activity, we can make informed decisions about our postpartum exercise program. Keeping a simple exercise journal can help track which activities provoke symptoms and which feel supportive, allowing for periodic adjustments to the program as needed.
Advanced Recovery: Months 3-6
As we progress into the 3-6 month postpartum period, our bodies continue to heal and adapt. This phase is critical for new mothers looking to return to their pre-pregnancy exercise routines or take up new activities. It’s essential to approach this period with a well-structured plan to ensure a safe and effective recovery.
Returning to Higher Impact Activities
When returning to higher impact activities, it’s crucial to do so gradually. This might involve starting with low-intensity versions of your chosen sport or exercise and gradually increasing the intensity. For instance, runners can begin with short distances and gradually increase their mileage. It’s also vital to monitor your body’s response to these new demands, particularly paying attention to any signs of knee joint laxity or discomfort.
Gradually reintroduce movement patterns specific to your chosen activity.
Begin with controlled movements at slow speeds before progressing to more complex drills.
Ensure proper form and technique to minimize the risk of injury.
Training Considerations
When developing a training plan, consider the following:
For court sports like tennis or basketball, start with lateral movement patterns before advancing to reactive agility drills.
Runners should focus on proper form and gradually increase distance before adding speed work.
Cyclists should ensure a proper bike fit and start with shorter rides.
For weightlifting or CrossFit, master perfect form with lighter loads before progressing to heavier weights.
It’s also beneficial to work with a coach or trainer who is familiar with postpartum return to sport to develop a customized progression plan. Remember to incorporate periodization in your training plan, allowing for recovery weeks to enable your tissues to adapt to the new demands.
Managing Pain and Discomfort
Knee pain following pregnancy is a common issue that requires thoughtful management to ensure a smooth recovery. We understand that managing postpartum knee pain effectively is crucial for new mothers to regain mobility and comfort.
Non-Pharmaceutical Approaches to Pain Relief
Non-pharmaceutical methods are often the first line of defense against postpartum knee pain. These can include gentle exercises, physical therapy, and the use of supportive devices. Proper body mechanics and daily movement modifications can also significantly reduce discomfort.
Gentle rehabilitation exercises tailored to the postpartum period can help strengthen the muscles around the knee.
Using supportive devices such as knee braces can provide additional stability.
When Medication May Be Appropriate
While non-pharmaceutical approaches are preferred, there are situations when medication may be necessary for managing postpartum knee pain. It’s essential to consult with a healthcare provider before taking any medication, especially if breastfeeding.
Medication Type
Use During Breastfeeding
Notes
Acetaminophen (Tylenol)
Generally considered safe
Effective for mild to moderate pain
Ibuprofen (NSAID)
Short-term use under medical guidance
Manages inflammation and pain
Topical Analgesics
Safe, with minimal systemic absorption
Provides localized pain relief
We must remember that pain medication should complement, not replace, appropriate rehabilitation exercises and activity modifications. Always take the lowest effective dose for the shortest duration necessary to manage symptoms.
Working with Healthcare Professionals
Collaborating with various healthcare providers is often the best approach to addressing postpartum knee problems. Managing postpartum knee laxity effectively requires a comprehensive care approach that addresses both the physical and emotional aspects of recovery.
Physical Therapy for Postpartum Knee Issues
Physical therapists play a crucial role in the assessment and rehabilitation of postpartum knee issues. They provide specialized exercises and interventions tailored to improve knee function and address related pelvic and core issues. A physical therapist can help new mothers regain strength and stability in their knees through targeted strengthening exercises and education on proper body mechanics.
Collaborative Care Approach
A collaborative care approach involving multiple healthcare providers often yields the best outcomes for postpartum knee issues. This team may include obstetricians or midwives for initial screening, primary care physicians to rule out serious pathology and manage medication, orthopedic specialists for complex cases, women’s health specialists for related issues like diastasis recti, lactation consultants to optimize breastfeeding positions, and mental health professionals to address any contributing mood disorders.
Obstetricians or midwives provide initial screening and referrals.
Primary care physicians help rule out serious pathology and coordinate care.
Physical therapists offer specialized assessment and rehabilitation.
Orthopedic specialists are consulted for complex cases or when conservative management isn’t effective.
Effective communication between these providers ensures comprehensive care addressing all aspects of postpartum recovery.
By working together, these healthcare professionals can provide a comprehensive treatment plan that addresses the unique needs of each new mother, promoting optimal recovery and long-term knee health for women.
Special Considerations for Athletic Mothers
As athletic mothers navigate their postpartum journey, they face unique challenges in returning to their sport. The process of regaining pre-pregnancy performance levels can be complex and varies significantly among individuals.
Modified Training Programs
Athletic mothers require modified training programs that account for the physiological changes that occurred during pregnancy. These changes can affect their performance and overall athletic capability.
When designing a postpartum training program, it’s essential to consider the following factors:
The impact of pregnancy on muscle strength and flexibility
The role of hormonal changes in ligament laxity
The need for gradual progression in intensity and volume
Training Component
Postpartum Considerations
Modification Strategies
Cardiovascular Endurance
Reduced aerobic capacity
Gradual increase in intensity and duration
Muscle Strength
Loss of muscle mass
Progressive resistance training
Flexibility and Mobility
Increased ligament laxity
Focus on gentle, controlled movements
Setting Realistic Performance Expectations
Setting realistic expectations is crucial for athletic mothers returning to sport after pregnancy. It’s essential to understand that returning to pre-pregnancy performance levels typically takes 9-12 months for most athletic women, with elite athletes sometimes requiring even longer.
Athletic mothers should focus on process goals, such as consistent training and proper form, rather than outcome goals, like specific times or competitive results. This approach helps in maintaining a positive and healthy mindset during the recovery period.
By acknowledging the changes in their body and adapting their training accordingly, women, including pregnant women, can navigate their postpartum journey with confidence and patience.
Preventing Future Joint Issues
As women continue their postpartum journey, it’s essential to consider strategies for preventing future joint issues. Pregnancy-related joint changes can have long-lasting effects, and understanding how to mitigate these effects is crucial for maintaining optimal joint health.
Long-Term Strengthening Strategies
Implementing long-term strengthening strategies can significantly reduce the risk of future joint problems. Establishing optimal knee and hip strength is particularly important, as this provides a buffer against the effects of pregnancy-related hormones on joint stability. Developing strong core and pelvic floor function is also vital, as these provide foundational stability that helps protect the knees during future pregnancies.
Some effective long-term strengthening strategies include:
Engaging in regular exercise that targets the core, hips, and knees
Incorporating activities that improve balance and coordination
Gradually increasing the intensity of workouts to challenge the muscles and joints
Exercise Type
Benefits
Examples
Core Strengthening
Improves stability, reduces risk of joint issues
Planks, bridges, pelvic tilts
Hip Strengthening
Enhances knee stability, improves mobility
Squats, lunges, leg press
Knee Strengthening
Supports knee joint, reduces pain risk
Leg extensions, leg curls, straight leg raises
Preparing for Subsequent Pregnancies
For women planning subsequent pregnancies, preparation is key to minimizing additional knee joint laxity and associated discomfort. Research suggests that joint laxity may develop more rapidly during second and subsequent pregnancies, making pre-pregnancy strengthening particularly important.
Preparing your body for subsequent pregnancies involves working with a physical therapist to identify and address any residual movement compensations from previous pregnancies. It’s also crucial to consider the timing between pregnancies, as full tissue recovery and strength rebuilding typically takes 12-18 months.
Embracing Your Postpartum Body and Its Capabilities
Embracing our postpartum body means recognizing its strength and resilience in the face of pregnancy and childbirth. The changes our body experienced during this period, including knee ligament laxity, are part of the normal physiological process of creating and nurturing new life.
As we journey through the postpartum period, it’s essential to shift our perspective from viewing postpartum body changes as “problems to fix” to seeing them as adaptations that served an important purpose in our journey to motherhood. We should appreciate the remarkable resilience of our body in its ability to gradually recover and adapt to new demands.
Celebrating functional victories, such as being able to play on the floor with our baby without knee pain, is more important than focusing solely on aesthetic or performance-based goals. Connecting with other postpartum women can validate our experience and provide perspective on the common challenges of physical recovery after childbirth.
Practicing self-compassion when progress feels slow or setbacks occur is vital, understanding that recovery is rarely linear and influenced by stress, sleep deprivation, and the demands of motherhood. We must recognize that some degree of change may be permanent, but this doesn’t diminish our body’s value or capability—it’s simply different than before.
By finding movement practices that bring us joy and help us connect positively with our body, we can foster a more positive body image. Remembering that our postpartum body tells the story of our strength and the miracle of creating new life, we can begin to see its changes as badges of honor rather than flaws to overcome.
FAQ
What is the typical timeline for knee joint recovery after childbirth?
The recovery timeline varies among women, but generally, knee joint stability improves within 3-5 months after delivery. However, some women may experience lingering issues that require continued support and exercise.
How do hormonal changes during pregnancy affect knee ligaments?
Hormonal fluctuations, particularly the increase in relaxin, can cause ligaments to become more elastic, leading to increased joint laxity and potentially affecting knee stability.
What are some common symptoms of knee joint issues during the postpartum period?
Women may experience pain, instability, or a feeling of “giving way” in the knee, especially during activities like walking or supporting their body weight.
Are there any specific exercises that can help support knee health during the postpartum period?
Gentle exercises like isometric strengthening, range of motion activities, and proper walking techniques can help promote knee stability and alleviate discomfort.
How can new mothers modify their daily activities to reduce strain on their knee joints?
Practicing proper body mechanics, using supportive devices or braces when needed, and making conscious movement modifications can help minimize stress on the knee joints.
When should I seek professional help for knee pain or instability?
If you experience persistent or severe knee pain, instability, or concerns about your knee health, it’s essential to consult with a healthcare professional for personalized guidance and support.
Can nutrition and hydration impact knee joint health during the postpartum period?
Yes, incorporating anti-inflammatory foods and staying hydrated can support joint health and potentially alleviate discomfort or pain.
Knee joint pain is a pervasive issue that affects individuals across all age groups and lifestyles. From athletes pushing their physical limits to older adults navigating the challenges of aging joints, knee pain can significantly impact daily activities and overall quality of life. Understanding the underlying causes of knee pain is crucial for accurate diagnosis and effective treatment. This comprehensive guide explores various mechanical problems, types of arthritis, and other potential causes, along with risk factors and diagnostic procedures.
[Image: An anatomical illustration of the knee joint, highlighting its complex structure including bones, cartilage, ligaments, and tendons, with labels pointing to common areas of pain.]
The knee, being one of the largest and most complex joints in the human body, is susceptible to a wide range of issues. Its intricate structure, comprising bones, cartilage, ligaments, and tendons, works in harmony to support our body weight and facilitate movement. However, this complexity also makes it vulnerable to various forms of injury and degeneration.
Mechanical Problems
Mechanical problems in the knee often result from injury or wear and tear on the joint’s components. These issues can cause pain, instability, and reduced range of motion.
Ligament Injuries
Ligaments are tough, elastic bands of tissue that connect bones to each other and provide stability to joints. The knee has four main ligaments, each susceptible to injury:
Anterior Cruciate Ligament (ACL)
Posterior Cruciate Ligament (PCL)
Medial Collateral Ligament (MCL)
Lateral Collateral Ligament (LCL)
[Image: A diagram showing the four main ligaments of the knee, with a side-by-side comparison of a healthy knee and one with a torn ACL.]
ACL Injuries
The ACL is one of the most commonly injured knee ligaments, especially among athletes. ACL tears often occur during activities that involve:
Sudden stops or changes in direction
Pivoting with the foot planted
Landing incorrectly from a jump
ACL injuries can range from mild sprains to complete tears. A characteristic “popping” sound often accompanies the injury, followed by rapid swelling and instability in the knee.
MCL Injuries
The MCL is frequently injured in contact sports or activities that involve quick changes in direction. MCL tears typically result from:
A direct blow to the outer part of the knee
Twisting or rotating the knee while the foot is planted
MCL injuries often cause pain and swelling on the inner side of the knee and may lead to instability when the knee is bent.
Meniscus Tears
The meniscus is a C-shaped piece of cartilage that acts as a cushion between the thighbone (femur) and shinbone (tibia). Each knee has two menisci:
Medial meniscus (inner side of the knee)
Lateral meniscus (outer side of the knee)
[Image: A cross-section view of the knee showing the location and shape of the menisci, with an example of a torn meniscus.]
Meniscus tears can occur due to:
Twisting or rotating the knee, especially when putting full weight on it
Aging and degenerative changes in older adults
Sports injuries, particularly in contact sports
Symptoms of a meniscus tear include:
Pain, especially when twisting or rotating the knee
Swelling and stiffness
Catching or locking of the knee
Difficulty fully straightening the knee
The severity of meniscus tears can vary, from minor tears that heal on their own to more severe tears that may require surgical intervention.
Patellar Tendinitis
Patellar tendinitis, also known as “jumper’s knee,” is an overuse injury affecting the tendon that connects the kneecap (patella) to the shinbone. This condition is common among athletes, especially those involved in sports that require frequent jumping.
[Image: An illustration showing patellar tendinitis, highlighting the inflamed patellar tendon and its connection to the kneecap and shinbone.]
Causes of patellar tendinitis include:
Repetitive stress on the patellar tendon
Sudden increases in training intensity or frequency
Inadequate rest between intense physical activities
Misalignment of the kneecap
Symptoms typically include:
Pain below the kneecap, especially during activities like jumping or climbing stairs
Tenderness when pressing on the affected area
Stiffness, particularly after periods of inactivity
If left untreated, patellar tendinitis can progress from an acute condition to a chronic problem, potentially leading to tendon degeneration and increased risk of rupture.
Arthritis
Arthritis is a common cause of knee pain, especially in older adults. There are several types of arthritis that can affect the knee joint, each with its unique characteristics and treatment approaches.
Osteoarthritis (OA)
Osteoarthritis is the most common form of arthritis affecting the knee. It’s a degenerative condition characterized by the breakdown of cartilage in the joint, leading to pain, stiffness, and reduced mobility.
[Image: A comparison of a healthy knee joint versus one affected by osteoarthritis, showing the cartilage breakdown, bone spurs, and narrowing of the joint space.]
Key features of osteoarthritis include:
Gradual onset of symptoms, typically developing over years
Pain that worsens with activity and improves with rest
Morning stiffness that typically lasts less than 30 minutes
Creaking or grinding sensation in the knee (crepitus)
Development of bone spurs (osteophytes)
Risk factors for developing knee osteoarthritis include:
Advanced age
Obesity
Previous joint injuries
Repetitive stress on the joint
Genetic predisposition
As osteoarthritis progresses, it can lead to significant pain and disability, potentially necessitating joint replacement surgery in severe cases.
Rheumatoid Arthritis (RA)
Rheumatoid arthritis is an autoimmune condition where the body’s immune system mistakenly attacks the synovial membrane, causing inflammation and joint damage. Unlike osteoarthritis, RA often affects both knees simultaneously.
[Image: An illustration comparing a normal knee joint to one affected by rheumatoid arthritis, highlighting synovial inflammation and joint erosion.]
Characteristics of rheumatoid arthritis in the knee include:
Symmetrical joint involvement (both knees often affected)
Pain, swelling, and warmth in the affected joints
Morning stiffness lasting more than an hour
Fatigue and general feeling of illness
Potential for joint deformity in advanced stages
RA is a systemic disease, meaning it can affect other parts of the body beyond the joints, including the skin, eyes, lungs, and blood vessels.
Gout and Pseudogout
Gout and pseudogout are types of arthritis caused by the deposition of crystals within the joint space.
Gout
Gout results from the accumulation of uric acid crystals in the joint. While it most commonly affects the big toe, knee involvement is not uncommon.
[Image: A microscopic view of uric acid crystals associated with gout, alongside an illustration of a gouty knee joint.]
Gout attacks are characterized by:
Sudden onset of severe pain, often occurring at night
Redness, warmth, and swelling in the affected joint
Extreme tenderness, even to light touch
Limited range of motion
Risk factors for gout include:
High levels of uric acid in the blood
Obesity
Excessive alcohol consumption
Diet high in purines (e.g., red meat, organ meats, some seafoods)
Certain medications (e.g., diuretics)
Pseudogout
Pseudogout, also known as calcium pyrophosphate deposition disease (CPPD), is caused by calcium pyrophosphate crystals forming in the joint.
Characteristics of pseudogout include:
Sudden attacks of pain and swelling, similar to gout
More common in older adults
Often affects larger joints like the knee
May be associated with other medical conditions or joint trauma
Both gout and pseudogout can lead to long-term joint damage if left untreated, emphasizing the importance of proper diagnosis and management.
Other Causes
While mechanical problems and arthritis are common culprits, several other conditions can cause knee joint pain.
Infections
Joint infections, also known as septic arthritis, can cause significant knee pain and require immediate medical attention.
[Image: An illustration showing a knee joint affected by septic arthritis, highlighting increased joint fluid and inflammatory changes.]
Causes of knee joint infections include:
Bacterial infections entering the joint through the bloodstream
Direct inoculation through injury or surgery
Spread from nearby infected tissues
Symptoms of a knee joint infection include:
Sudden onset of severe pain
Marked swelling and redness
Warmth around the joint
Fever and chills
Inability to bear weight on the affected leg
Prompt diagnosis and treatment with antibiotics and sometimes surgical drainage are crucial to prevent permanent joint damage.
Bone Tumors
While relatively rare, bone tumors can cause knee pain and swelling. These tumors can be benign (non-cancerous) or malignant (cancerous).
Types of bone tumors that can affect the knee include:
Osteochondromas: Benign bone tumors that typically develop in adolescents and young adults
Giant cell tumors: Usually benign but locally aggressive tumors
Osteosarcoma: A malignant bone cancer that can occur around the knee, especially in children and young adults
[Image: A series of X-ray or MRI images showing different types of bone tumors that can occur around the knee joint.]
Symptoms of bone tumors may include:
Persistent pain, often worse at night
Swelling or visible lump
Fractures due to weakened bone
Limited range of motion
Early detection and proper diagnosis are crucial for effective treatment of bone tumors.
Referred Pain
Sometimes, knee pain may not originate in the knee itself but can be referred from problems in other parts of the body, particularly the hip or lower back.
[Image: A diagram showing how pain from the hip or lower back can be referred to the knee, with nerve pathways highlighted.]
Characteristics of referred knee pain:
Pain patterns that don’t match typical knee injury or arthritis symptoms
Accompanying symptoms in the hip, lower back, or along the leg
Pain that doesn’t respond to typical knee treatments
Proper diagnosis of referred pain is essential to address the underlying cause and provide effective treatment.
Risk Factors
Several factors can increase an individual’s risk of developing knee joint pain. Understanding these risk factors can help in prevention and early intervention.
Age
As we age, the risk of developing knee pain increases due to:
Natural wear and tear on joint cartilage
Decreased muscle strength and flexibility
Higher likelihood of developing osteoarthritis
Accumulated effects of previous injuries
Gender
Gender can play a role in the development of knee pain:
Women are more prone to certain knee problems, such as patellofemoral pain syndrome
Hormonal changes, particularly during menopause, can affect joint health
Anatomical differences, such as wider hips in women, can affect knee alignment and stress
Obesity
Excess weight places additional stress on knee joints, significantly increasing the risk of knee pain and osteoarthritis.
Each pound of body weight exerts about 4 pounds of pressure on the knees when walking
Weight loss can dramatically reduce knee pain and slow the progression of osteoarthritis
[Image: An illustration showing how excess weight increases stress on the knee joint, with comparative figures for normal weight vs. obese individuals.]
High-Risk Activities
Certain activities and occupations can increase the risk of knee problems:
Jobs requiring repetitive knee stress (e.g., construction, carpet laying)
Activities involving frequent kneeling or squatting
While these activities don’t necessarily need to be avoided, proper training, technique, and protective equipment can help reduce the risk of knee injuries.
Diagnostic Procedures
Accurate diagnosis is crucial for effective treatment of knee joint pain. Healthcare providers use a combination of physical examination, imaging tests, and sometimes laboratory analysis to determine the underlying cause of knee pain.
Physical Examination
A thorough physical examination is the first step in diagnosing knee pain. The healthcare provider will:
Observe gait and standing posture
Palpate the knee to check for areas of tenderness, swelling, or warmth
Assess range of motion and stability
Perform specific tests to evaluate ligaments and menisci (e.g., McMurray test, Lachman test)
[Image: A series of photos demonstrating various physical examination techniques for knee assessment.]
Imaging Tests
Various imaging modalities can provide detailed information about the structures within and around the knee joint.
X-rays
X-rays are often the first imaging test performed. They can show:
Bone alignment
Joint space narrowing (indicative of cartilage loss)
Bone spurs (osteophytes)
Fractures
Magnetic Resonance Imaging (MRI)
MRI provides detailed images of soft tissues, including:
Ligaments and tendons
Cartilage and menisci
Bone marrow changes
[Image: Side-by-side comparison of a knee X-ray and MRI, highlighting the different structures visible in each.]
Computed Tomography (CT)
CT scans can be useful for:
Detailed bone imaging
Evaluating complex fractures
Guiding interventional procedures
Ultrasound
Ultrasound can be helpful for:
Evaluating soft tissue structures in real-time
Guiding injections or aspirations
Assessing inflammation in tendons and bursae
Lab Tests
In some cases, laboratory tests may be necessary to diagnose or rule out certain conditions:
Blood Tests
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) to assess inflammation
Rheumatoid factor and anti-CCP antibodies for rheumatoid arthritis
Uric acid levels for gout
Joint Fluid Analysis
Aspiration of joint fluid (arthrocentesis) can help diagnose:
Infections (by culturing the fluid)
Crystal-induced arthritis (by identifying uric acid or calcium pyrophosphate crystals)
Inflammatory conditions (by analyzing cell counts and other markers)
[Image: A microscopic view of joint fluid analysis, showing different types of crystals associated with gout and pseudogout.]
Conclusion
Understanding the various causes of knee joint pain is crucial for both patients and healthcare providers. The knee’s complex structure makes it susceptible to a wide range of issues, from acute injuries to chronic degenerative conditions. By recognizing the signs and symptoms associated with different causes of knee pain, individuals can seek appropriate care more promptly.
It’s important to remember that knee pain can often result from a combination of factors. For instance, a minor injury in a person with underlying osteoarthritis can lead to a significant exacerbation of symptoms. Similarly, lifestyle factors like obesity can compound the effects of age-related joint changes.
Proper diagnosis is key to effective treatment. While some causes of knee pain, such as minor strains or overuse injuries, may resolve with rest and home care, others require professional medical intervention. Persistent or severe knee pain should always be evaluated by a healthcare provider to ensure appropriate management and prevent long-term complications.
By staying informed about the potential causes of knee pain and being proactive about joint health, individuals can take steps to maintain healthy, pain-free knees throughout their lives. Regular exercise, maintaining a healthy weight, using proper techniques during physical activities, and seeking timely medical attention when problems arise are all crucial components of long-term knee health.
[Image: A motivational image showing people of various ages engaged in knee-friendly activities like swimming, cycling, and low-impact exercises, emphasizing the importance of staying active for knee health.]
Foothills Sports Medicine Physical Therapy (Foothills), Arizona’s largest and most respected provider of musculoskeletal and physical therapy services, is pleased to announce that after months of diligent negotiations, an agreement has been reached with UnitedHealthcare (UHC). Effective August 1, 2024, Foothills will once again be an in-network provider for UHC’s commercial insurance and Medicare Advantage plans, providing thousands of patients covered by these plans with access to high-quality physical therapy services.
View our full list of providers
Foothills contracts with over 1,500 insurance plans. Below is a general list of United Healthcare plans included in the network.
Commercial United Healthcare
United Health One
UHC Golden Rule
UHC Oxford health insurance
United Healthcare Additional Plans
UHC AARP Medicare Complete
Medicare Advantage insurance from United Healthcare Group
UHC Student Resources
UMR
GEHA
Patients can view their insurer’s coverage here.
“We are pleased to have reached an agreement that will allow us to continue to provide the exceptional care our patients expect and deserve,” said Stephen Motte, COO of Foothills Sports Medicine Physical Therapy. “This resolution underscores our commitment to the well-being of our patients and the importance of accessible, high-quality health care.”
Foothills has been recognized as the top-rated physical therapy provider in Arizona for years. However, UHC’s low reimbursement rates have forced Foothills to withdraw from the network as it seeks to maintain its high standards for providing high-quality, affordable patient care.
“We are committed to ensuring that our patients have access to the best possible care, regardless of their insurance provider,” Motte said. “We hope that United Healthcare will continue to expand its position and agree to fair reimbursement rates so that we can continue to provide patients with access to the care they need.”
This multi-year agreement ensures that UHC members enrolled in employer-sponsored, individual commercial plans, and Medicare Advantage will once again have access to Phoenix AZ’s largest provider of physical therapy services. Restoring in-network status will ease the financial burden on patients and ensure continuity of care.
“Throughout the negotiation process, we remained focused on securing terms that benefit both our patients and our practice,” Motte said. “We look forward to continuing our mission to provide exceptional care to those who need it, without compromise.”
Foothills believes in the power of patient choice and the right to access the care they need, when they need it. Patient access is a top priority.
The largest study of CTE to date has found a new link between contact sports participation, chronic traumatic encephalopathy (CTE) and the development of a movement disorder known as parkinsonism.
The study of 481 deceased athletes by researchers from Boston University Chobanian and Avedisian School of Medicine and VA Boston Healthcare, published today in JAMA Neurologyit appears that most individuals with CTE developed parkinsonism, and CTE pathology appears to be the cause of the parkinsonism symptoms in most cases.
Parkinsonism is a condition characterized by symptoms similar to Parkinson’s disease, such as tremor, abnormal slowness of movement, or abnormal stiffness of the arms or legs. It has long been associated with traumatic brain injury (TBI) and CTE in boxers. However, the specific pathologies underlying these symptoms in CTE were unknown.
Parkinson’s disease is classically associated with the buildup of proteins called Lewy bodies in brain cells, but researchers found that 76% of individuals with CTE and Parkinsonism did not do Have Lewy body pathology.
“We were surprised to find that most individuals with CTE and parkinsonism did not have Lewy body pathology,” noted Thor Stein, MD, PhD, associate professor of pathology and laboratory medicine at BU and VA Boston Healthcare, and one of the study’s corresponding authors. “Instead,” Stein explained, “subjects with parkinsonism were more likely to have more severe CTE-related brain cell death in a region of the brainstem important for controlling movement.”
CTE is a degenerative brain disease whose only known cause is repeated head blows, such as those that occur in contact sports. A 2018 study by the same research team found that the duration of contact sports is associated with an increased risk of developing Lewy body disease. However, the current study is the first to describe a link between contact sports participation, brainstem pathology, and parkinsonism in CTE.
“Increased CTE severity has been shown to be associated with longer playing time,” noted Daniel Kirsch, an MD/PhD student at BU and one of the study’s first authors. “In this study, we found that eight additional years of contact sports play was associated with a 50 percent increased risk of more severe disease in a specific area of the brainstem that controls movement.”
The study subjects donated their brains to the Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE) brain bank. People with parkinsonism were compared to those without to identify the types of pathologies that might explain why some people with CTE develop these symptoms and to examine relationships with the duration of contact sports.
This study underscores the importance of understanding the long-term effects of repeated head impacts and the need for preventive measures in contact sports to reduce the risk of neurodegenerative diseases such as CTE and parkinsonism.
Dealing with Knee Pain After ACL Reconstruction Surgery
Anterior cruciate ligament (ACL) tears are a common knee injury, especially among athletes. Approximately 200,000 ACL reconstruction surgeries are performed in the United States every year to repair these torn ligaments. While the procedure helps stabilize the knee long-term, post-operative knee pain is incredibly common.
In one study, as many as 72% of patients continued experiencing knee pain even 2 years after their ACL reconstruction. This pain can persist due to multiple biomechanical and inflammatory factors during the healing and rehab process.
Understanding typical recovery timelines and implementing self-care and physical therapy protocols appropriately can help manage discomfort. With proper treatment, most individuals experience significant improvements in knee pain and function over the first post-operative year.
Acute Knee Pain: Swelling and Inflammation
In the early phases after surgery (1-2 months), acute inflammation around the knee joint is very common. Triggered by surgical trauma, swelling, stiffness, and significant pain with movement often occur as part of the body’s healing response. Fluid buildup and inflammation in and around the joint can lead to throbbing discomfort and difficulty bearing weight through the leg.
Controlling Inflammation Initially Critical
During this inflammatory period, management involves medication, frequent icing, compression bandages, keeping the leg properly elevated, and joint offloading with crutches or a brace. Moving too aggressively through range of motion before inflammation settles can worsen fluid build-up. Finding the right balance between rest and gentle movement is key. Once swelling reduces, light physical therapy emphasizing controlled mobility and muscular activation begins.
Ongoing Knee Pain Risk Factors
While most patients move past the intense acute pain phase after about 6-8 weeks, some individuals continue battling discomfort even months or years later. There are several potential culprits of this lingering knee pain:
Improper Biomechanics: Imbalances or atypical movement patterns (known as compensations) during activities like walking, running or squatting after ACL surgery can overload areas around the knee joint. Common issues involve knocking knees inward, improper landing mechanics from jumping, overpronating feet, and relying too heavily on uninjured limbs during exercise. Certain patients are predisposed towards persistent abnormalities or asymmetries due to age, sex, genetics and pre-existing conditions.
Quadriceps Weakness: The thigh muscles (quadriceps) typically atrophy after ACL tears from disuse and inflammation. Reactivating and rebuilding quadriceps strength is paramount for stabilizing the knee for dynamic activities. However, lingering weakness is common long-term after ACL reconstruction. This affects range of motion and shock absorption, causing worse outcomes and pain.
Secondary Joint Injuries: After ACL surgery, patients often unconsciously overcompensate and overload adjacent joints like the hip and ankle while recovering. Cartilage wear, tendinitis and premature arthritis in these areas causing referred pain at the knee is increasingly recognized. Similarly, other structures like the meniscus are frequently damaged in combination with ACL tears, necessitating additional surgeries if problematic.
Scar Tissue Build-Up: During healing, dense scar tissue commonly develops around the ACL graft. In some people, too much builds up or it adheres incorrectly to surrounding tissues. This misplaced and inflexible scar tissue tugging on nerves can directly generate knee pain with movement.
Graft Complications: In rarer cases of chronic pain, issues with the ACL graft itself have occurred. This includes delayed healing, improper graft positioning during surgery, reinjury of the graft, and possibly graft-tunnel mismatches contributing to instability and pain.
What Does Rehab Program Include?
Custom structured physical therapy programs are essential not only for regaining knee functionality after ACL reconstruction, but also helping wean off pain medications and prevent future problems.
Stage 1 – Early Mobility & Range of Motion
Begins with 1-2 weeks of inflammation control, then progresses to restoring passive knee extension/flexion mobility (ideally full range of motion by 12 weeks). Light quadriceps activation and proprioception exercises follow.
Stage 2 – Muscle Strengthening Phase
Focuses primarily on rebuilding quadriceps and hip strength, while progressing standing balance challenges. Abandoning crutches and slowly reintegrating walking with good mechanics is targeted before more advanced drills.
Stage 3 – Multiplane Dynamic Control
Incorporates movement pattern and stability training including single leg loading, squats, agility movements in multiple planes of motion. The goal is reestablishing proper knee shock absorption strategies and lower limb control. Closely managing strength/activity progressions prevents overloading.
Stage 4 – Sports Specific Training
Transitions towards advanced plyometric and high intensity sport-specific conditioning to simulate demands of athletic participation. Confidence in knee function gets tested before gradual full competition clearance.
Adhering to activity restrictions and exercise protocols in each phase allows for appropriate muscular and tissue-loading to stimulate healing without provocation. Touching base regularly with physical therapists and surgeons ensures appropriate customization and progressions.
Treatment Options for Ongoing Pain
If knee pain persists months beyond surgery despite appropriate adherence to rehabilitation protocols, further targeted evaluation and management is warranted:
Imaging Tests like x-rays, CT or MRI scans help identify abnormal bony alignment or positioned grafts contributing to symptoms. Secondary injuries causing issues are also spotted.
Return to the OR – Occasionally revision ACL surgery is required if the graft re-tears or was improperly placed. Other joint debris clean-ups or repairs (like meniscus fixing) may help reduce pain generators.
Viscosupplementation Injections – Hyaluronic acid gel injections into the knee can help lubricate and cushion joint spaces, temporarily aiding pain.
Braces & Orthotics – Unloader knee braces and custom shoe inserts help take pressure off injured ACL graft or problem joint areas to alleviate discomfort.
Physiotherapy – Further advanced manual therapy, taping techniques and corrective exercises target the specific dysfunction (quad weakness, movement pattern abnormalities etc) perpetuating pain.
While most post-ACL reconstruction knee pain improves significantly in 6-12 months with concerted rehabilitation, lingering issues left unaddressed can remain problematic long-term and increase arthritis risk. Thus, prompt intervention tailored to root causes provides better function restoration and enhanced quality of life.
Moving Forward Post-Surgery
Though uncomfortable and frustrating, pain after ACL surgery remains fairly common with modern techniques. Sticking firmly to prescribed activity guidelines and customized therapy plans allows for appropriate muscular development and movement pattern retraining for long-term knee health.
Patience and perseverance are key – with concerted effort from both patient and medical team, the road to recovery continues getting smoother. If pain seems atypical or severe, do not hesitate reaching out promptly to treat any complications early before they become permanent. With today’s treatment algorithms prioritizing function preservation, a return to high performance athletics and an active lifestyle is very achievable after ACL tears.
Results of the comprehensive strength ranking and grading
According to the ranking and grading results of 38 matches that H participated in from 2018 to 2020 in Table 10, there were only three matches between him and the player with the strongest comprehensive strength, which was consistent with the results of matches won by a large score. However, based on the Ci value analysis of the serve round and the receive round, the match (X3) is in the grade with the strongest comprehensive strength, and the first rank has the highest value in the serve round, consistent with the comprehensive strength ranking. The Ci value ranking of the receive round was 21st, which was at the lower average grade, and quite different from the ranking result of the comprehensive strength in the match. At the technical level, in the X3, H had excellent techniques and tactics in the serve round, especially the high contribution quality of attack after serve. Meanwhile, H could maintain a high-pressure situation and active attack with fewer mistakes from the attack after serving to stalemate phases. However, his techniques and tactics of the receive round were average. As a result, the contribution quality of serve rounds and receive rounds in this match showed a bipolar trend. This phenomenon illustrated that his superior techniques could make up for the mediocre or weak techniques in the match, so the overall strength of X3 was better than that of other matches. In previous studies, Chen [37] and Yin [38] have clearly pointed out that Chinese table tennis players Liu Shiwen and Ding Ning have experienced the phenomenon of unbalanced competitive strength with too obvious good and poor techniques in their matches, which is similar to the view that exists in this study. In terms of evaluation methods, the combination of TOPSIS and RSR contributes to the objectivity and accuracy of the comprehensive strength in each match so that the comprehensive strength of X3 could clearly distinguish the gap with other matches. Otherwise, researchers further analyzed the ranking and grade of the following groups, including X36 (3:4) and X30 (3:4) in the second grade as well as X7 (4:3), X19 (4:1) and X5 (4:2) in the third grade. Theoretically, the overall strength of the winning rounds in the third grade should be in a higher grade, especially since H won by a large score in X19. By contrast, the overall strength of the losing matches in the second grade should have been lowered, but the overall strength of the winning race in the third grade was higher than the winning race, which was quite different from the expectation of the theoretical and actual results. However, researchers had new findings through game videos and the above analysis. The chance of winning or losing a table tennis match has increased since the development of the 11-point system in table tennis and the implementation of the new material table tennis. In the meantime, winning or losing at a high level is decided by the most critical points. The imbalance of the winning and losing relationship in the above matches in this study is consistent with the problems raised by Huang [39] and Cui [40] in their research results. There is a 5% probability of total score-loss imbalance (i.e., a player wins the match but scores less than his opponent) occurred in international male table tennis match. Therefore, the individual technical and tactical indicators of table tennis players can be applied to objectively reflect the effect of technical and tactical play in each stage by selecting the contribution quality of individual technical and tactical indicators and using the comprehensive evaluation combining TOPSIS and RSR. This method could conduct a more objective and comprehensive evaluation of the overall strength of a match. Prior to this, Yang et al. [27] conducted a comprehensive evaluation of the attack and defense ability of volleyball players in the competition by combining TOPSIS and RSR method, and believed that the combination of the two could comprehensively evaluate the attack and defense strength of each team, as well as the ranking of guard positions, which had certain reliability and rationality. In his study, Zhao and Tang [32] used TOPSIS alone to evaluate the competition quality of two high-level Chinese table tennis players, and the comprehensive ranking could also reflect the competitive status of the players to a certain extent. It shows that the combined application of the two comprehensive evaluation methods is feasible to diagnose the contribution efficiency of table tennis matches. In this regard, athletes can understand their technical and tactical deficiencies through comprehensive evaluation and analysis. Meanwhile, the analysis of their advantages and disadvantages in techniques and tactics when competing with strong and weak players could help athletes carry out targeted training for athletes to strengthen their weak techniques in future training. In this way, their techniques can provide stable and changeable intentions for implementing tactics in field competitions. Furthermore, coaches can help athletes to formulate corresponding tactical training based on analytical results. Afterwards, athletes could further understand their shortcomings in field competitions to strengthen the connection and conversion of techniques and tactics in the future and avoid polarized performances (the technical and tactical play is volatile) [37,38,39,40].
The selection of various evaluation indicators
Table tennis matches have diverse evaluation indexes, such as the initial three-phase index, ten-phase index, and more widely used four-phase index. All of these methods aim to conduct statistics on the score and loss of each technique and tactic. However, some scholars analyzed the use of the active attack, spin serve, control, defence, position, hit placement and other indexes to study the technique and tactics of table tennis. Some scholars directly analyzed the scoring effect or losing effect of technique and tactic in each stroke. For example, unilateral evaluation of the scoring rate of various indicators in table tennis could not objectively evaluate the comprehensive competitive strength of athletes because the loss of points in the competition was ignored, leading to different evaluation results. Moreover, the evaluation composed of technical and tactical indicators such as an attack, defence, control, and position involves too many technical and tactical indicators (e.g.: according to the characteristics of the athlete’s position, there are short court attack after receive, middle court or back court counterattack, rally or defense, etc.). In the meantime, it was difficult to collect technical and tactical data. The implementation effect of technical and tactical could only be obtained from the unilateral score or loss, so it was laborious to highlight the contribution quality of table tennis matches. According to the previous table tennis technical phase can be divided into attack after serve phase, attack after receive phase and rally phase.With the reform of table tennis rules and equipment, the past Three-phase table tennis technology has been unable to meet the needs of current table tennis technology statistics, and there is also the problem of table tennis competition data statistics not corresponding [8]. Therefore, in terms of the selection of technical indicators in table tennis matches, Zhao and Tang used TOPSIS to evaluate the scoring rate of six indicators, including serve, attack after serve or control (the third stroke), receive, continuous attack after receive or control (the fourth stroke) and rally technique [32]. When Wang used RSR to analyze the offensive techniques of women’s table tennis matches, he selected the hit rate and scoring rate of serve, attack after serve, attack on the fifth stroke and attack after the seventh stroke as indicators to evaluate the offensive techniques of athletes [41]. These studies are sub-indicators selected on the basis of Three-phase technical indicators, which fail to consider the problems corresponding to the competition data and the utilization rate of athletes. In the match, the athletic performance of athletes cannot be reflected only by the scoring rate, which is not comprehensive enough. Each point scored or lost in the match needs to be converted into a scoring rate and utilization rate to determine the effect of the athlete’s technical efficiency output. High scoring rate and low utilization rate or high utilization rate and low scoring rate reflect the technique level of athletes. The contribution rate includes the effect of scoring rate and utilization rate, and the contribution rate of athletes in the corresponding phase can directly reflect the quality of athletes’ contribution per stroke. Therefore, based on previous studies, this study selects the four-phase index (Purpose: the four-phase index effectively solves the problem that the data of the fifth stroke was not corresponding), including the serve round——the attack after serve (the first stroke, the third stroke, the loss of the fifth stroke) and the stalemate I phase (the score of the fifth stroke, the seventh stroke and later), the receive round——the attack after receive (the first stroke, the third stroke, the loss of the fifth stroke) and the stalemate II phase (the sixth stroke, the eighth stroke and later) and the score and loss of the last stroke as statistical points. The scoring rate and utilization rate were calculated by the score and loss in each stroke. Through this way, researchers could obtain the contribution quality of each stroke. This index makes up for the shortcoming that some scholars only analyze the competition quality from the score but ignore the utilization effect of techniques in matches. Meanwhile, as an easy and understandable evaluation method, the contribution quality of each stroke in the four-phase index can objectively and comprehensively reflect the actual differences between single or multiple matches, which makes the evaluation results more representative than other methods. It can also provide decision-making guidance for coaches to clearly understand the contribution effect of athletes in a certain technical phase or a certain stroke in the match. In addition, this study focused on applying TOPSIS and RSR in the comprehensive evaluation of the contribution quality of techniques and tactics in table tennis matches, aiming to provide a new method and idea for analyzing techniques and tactics. In evaluating technical and tactical indicators based on different evaluation purposes in the specific operation process, the evaluation indicators could be adjusted according to the corresponding evaluation purposes. In the meantime, the evaluation could be added when athletes could implement other corresponding technical and tactical indicators in the competition, which was more representative of evaluating the comprehensive competitive strength of athletes.
The application of the evaluation method
TOPSIS and RSR are two frequently-used comprehensive evaluation methods without special requirements for the data used. Currently, the relatively widely applied fields of TOPSIS mainly focus on enterprise performance management, health decision-making and public health management, etc. [41, 42]. In sports, they were also applied to evaluate the competition performance of basketball, football and volleyball [27, 34, 36]. RSR is more used in basketball. The main advantages of the two comprehensive evaluation methods are simple operation, flexible application, objective and accurate measurement of the evaluated objects, and there are no special requirements on the size of the sample, the number of evaluation objects and the distribution of index data. For example, the same trend transformation and normalization of the raw data by TOPSIS can eliminate the influence of different index levels, and the ranking results make full use of the raw data information, which can quantitatively reflect the degree of superiority and inferiority of different evaluation stages, and have certain practical value in the evaluation of contribution quality indexes of table tennis tournaments. Moreover, the resulting data processing results are easy to understand and more in line with the actual situation of table tennis match. However, when a particular index has a significant degree of dispersion, the results calculated by TOPSIS may not be stable, and the advantages and disadvantages of evaluation objects cannot be classified [41]. Due to this, RSR can cover the shortcomings of TOPSIS and broaden the application range of TOPSIS. On the other hand, TOPSIS can fill the fault of RSR, which is resulted from excessive information loss due to non-parametric transformation. The combined application of both methods can carry out reasonable evaluation and classification, which improves the statistical efficiency and makes the evaluation results more objective by complementing both advantages [43], avoiding the limitations of a single evaluation method. According to the previous literature, in the field of sports, whether it is Chinese literature or foreign literature, it is common to use a single method (TOPSIS or RSR) for quality evaluation, and to some extent there is unreasonable index evaluation phenomenon. However, in the field of public health, there are many literatures that use TOPSIS combined with RSR for comprehensive evaluation. For example, TOPSIS is used for comprehensive evaluation of hospital medical quality, while RSR is used for more reasonable classification evaluation based on TOPSIS analysis. Therefore, the combination of the two can achieve complementary advantages and avoid unreasonable single evaluation [32]. In addition, by comparing the comprehensive evaluation of the four-phase indicators on the competitive performance of each match, it is found that the four-phase indicator evaluation can separately assess the competitive strength of each phase of each game. For example, according to Yang and Zhang’s “four-phase index evaluation method” and “four-phase index strength difference method”, the scoring rate, utilization rate and strength difference of four-phase indexes are divided into different evaluation levels based on the scoring rate and utilization rate [8, 9]. In terms of the contribution rate of four-phase indexes, the diagnostic formula of four-phase indexes’ contribution rate extended by Yin et al. [44]. can effectively diagnose the magnitude and advantages and disadvantages of the contribution rate of each phase index in each match. However, the four-phase indicator evaluation method mentioned above only evaluates the competitive performance of each phase of each match, and cannot assess, rank and archive the comprehensive strength of each match. Therefore, TOPSIS combined with RSR method for table tennis competitive strength evaluation can effectively optimize the above existing defects. Based on this consideration, this study combines two methods. This combination changed the traditional evaluation methods adopted in previous studies of table tennis techniques and tactics to avoid the shortcomings such as complicated index selection, sophisticated calculation, and dispersed evaluation. Meanwhile, it could enhance objectivity, rationality and accuracy in the comprehensive strength evaluation in table tennis matches. So it can provide scientific evidence for the training of athletes and the decisions of coaches. Meanwhile, this method is also worthy of further promotion and application in net games.
The limitations of this study
There were still some limitations in this study. First, this study was only evaluated unilaterally from the match data of H, a International Excellent table tennis player. It was impossible to directly and objectively infer the competitive state of the other player in the match. So, data from both athletes could be included for comparative evaluation and analysis in future studies. Second, due to the impact of the epidemic, many important international table tennis matches were suspended, which led to the imbalance between the selection of different matches and the designated time period, failing to achieve real-time tracking and statistics. In addition, the grib method and technical characteristics of the opponent are not specifically described in the paper, which leads to the limited application value of this study to a certain extent. It is hoped that relevant scholars can further improve the design and analysis of the comprehensive evaluation of competitive strength in table tennis match in the future. Finally, this study only quantified the game data from videos and ignored the psychological changes of the athletes in the game. In some critical games, the loss or win was not a technical or tactical problem but a psychological problem. For example, an athlete usually showed more flexible and steady techniques and tactics when he was ahead by a large margin. Due to this variable, future studies should pay attention to the combination of quantitative research on the technical and tactical index data of athletes and qualitative research on clinical performances to analyze techniques and tactics.
If walking around on flat surfaces feels fine but your knees start to ache as soon as you start climbing stairs, you might be wondering what’s going on. While your knees are designed to withstand a lot of pressure, stepping onto a staircase engages different muscles and makes you move at an angle while working against gravity. As you climb, your knees may end up bearing a force that’s anywhere from three to six times your body weight. That extra pressure alone shouldn’t hurt, but if you’ve been doing a lot of stair climbing, have an underlying health condition, or even just turn the wrong way you might find that taking the stairs is suddenly painful. There are many possible causes of knee pain when climbing stairs, including patellofemoral pain syndrome, meniscus tear, chondromalacia patella, IT band syndrome, and muscle imbalance. Strengthening and stretching exercises, body awareness, and modifying walking technique can help prevent and treat knee pain when going up steps.
Key Takeaways:
Knee pain when climbing stairs can be caused by various conditions such as patellofemoral pain syndrome, meniscus tear, chondromalacia patella, IT band syndrome, and muscle imbalance.
Strengthening and stretching exercises, body awareness, and modifying walking technique can help prevent and treat knee pain when going up steps.
Proper knee anatomy understanding is important to comprehend why knee pain occurs when climbing stairs.
Rest, physical therapy, pain relievers, assistive devices, and surgical intervention may be needed for treating and managing knee pain on stairs.
Listening to your body and seeking professional guidance is essential for finding lasting relief and improving overall knee function.
The Anatomy of the Knee
In order to understand knee pain when climbing stairs, it helps to know some basics about what comprises your knee and how this important joint works. The knee joint consists of the patella (kneecap), femur (thigh bone), and tibia (shin bone). Ligaments hold everything together, including collateral ligaments and cruciate ligaments. Tendons connect muscle to bone, while cartilage lines the ends of the knee bones and helps them glide. Menisci act as bumper pads for shock absorption, and bursae provide extra cushioning. Several muscles are involved in bending and straightening the knee, and nerves transmit signals to the brain.
Anatomical Component
Description
Patella
The kneecap that sits over the front of the knee joint.
Femur
The thigh bone that connects to the knee joint.
Tibia
The shin bone that forms the lower part of the knee joint.
Ligaments
Collateral ligaments and cruciate ligaments that provide stability and support to the knee joint.
Tendons
Connective tissues that attach muscles to bones, allowing movement.
Cartilage
A smooth, elastic tissue that covers the ends of the knee bones, preventing friction and allowing for smooth movement.
Menisci
C-shaped discs of cartilage that act as shock absorbers and help distribute weight evenly across the knee joint.
Bursae
Fluid-filled sacs that reduce friction between tendons, ligaments, and bones.
Muscles
Various muscles, including the quadriceps and hamstrings, that facilitate movement and stability of the knee joint.
Nerves
Nerves that transmit signals between the knee joint and the brain, allowing for sensory and motor functions.
Common Causes of Knee Pain on Stairs
Knee pain while climbing stairs can be caused by a variety of conditions. Understanding these causes can help identify the appropriate treatment and management strategies for alleviating the pain and discomfort. The common causes of knee pain on stairs include:
Patellofemoral Pain Syndrome: Also known as runner’s knee, this condition results in pain at the front of the knee. It is often caused by overuse or a sudden increase in physical activity.
Meniscus Tear: A tear in the meniscus, either due to a specific injury or age-related degeneration, can lead to pain on the inner or outer aspect of the knee.
Chondromalacia Patella: This condition involves the wearing of the cartilage behind the kneecap, which leads to irritation and a dull ache.
IT Band Syndrome: The rubbing and irritation of the IT band can cause pain on the outside of the knee, particularly when going down stairs.
Muscle Imbalance: Being quad dominant, or having an imbalance between the quadriceps and other leg muscles, can put excess pressure on the front of the knee, resulting in pain while climbing stairs.
Managing these conditions and alleviating knee pain when going up steps often involves a combination of strengthening exercises, improving body awareness, and modifying walking technique. By addressing these underlying causes, individuals can find relief and improve their overall knee health.
“Understanding the specific causes of knee pain on stairs is crucial for effective treatment and management strategies.”
Treatment and Management of Knee Pain on Stairs
When it comes to addressing knee pain while going up and down stairs, there are several effective treatment and management options available. These approaches target different aspects of the issue to provide relief and promote healing. Let’s explore some of the key strategies:
Targeted Exercises
One effective way to alleviate knee pain is through targeted exercises that strengthen the structures surrounding the knee. These exercises can help improve stability, support, and flexibility. Consider incorporating exercises such as hip flexor stretches, single-leg lifts, and hamstring stretches into your routine. These exercises specifically target the muscles and tendons around the knees, promoting strength and resilience.
Body Awareness and Modification of Walking Technique
Developing body awareness and understanding proper movement and alignment can help reduce knee pain on stairs. By being mindful of your posture and movement patterns, you can avoid unnecessary strain and pressure on the knees. Modifying your walking technique, such as squeezing your glutes, using a handrail for support, or keeping weight in your heels, can also alleviate discomfort and provide relief.
Rest and Physical Therapy
Proper rest is essential for the healing and recovery of the knees. Avoid overexertion and give your knees ample time to rest and recover. Physical therapy can also play a crucial role in knee pain management. A physical therapist can prescribe targeted exercises, provide guidance on proper movement patterns, and employ techniques such as massage, heat therapy, or electrical stimulation to promote healing and strengthen the knee.
Pain Relievers
Over-the-counter pain relievers can help temporarily alleviate discomfort associated with knee pain on stairs. Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen can help reduce inflammation and provide pain relief. However, it is important to consult with a healthcare professional before relying on pain relievers as a long-term solution.
Assistive Devices
In some cases, assistive devices can provide support and stability for individuals experiencing knee pain on stairs. Knee braces can help stabilize the knee joint and provide additional support during movement. Crutches or canes can also assist in taking weight off the affected knee and reducing pressure while walking on stairs. It is important to consult with a healthcare professional to determine the most suitable assistive device for your specific needs.
Surgical Intervention
While surgical intervention is typically considered a last resort, it may be necessary in certain cases to address underlying causes of knee pain. Surgical options can include procedures such as arthroscopic surgery to repair or remove damaged cartilage, meniscus repair, or even knee replacement surgery. If conservative treatments have been unsuccessful in managing knee pain on stairs, it is essential to consult with an orthopedic specialist to discuss potential surgical interventions.
By utilizing a combination of targeted exercises, modifying walking technique, rest, physical therapy, pain relievers, assistive devices, and, if needed, surgical intervention, individuals can effectively manage and alleviate knee pain when ascending and descending stairs.
Treatment Options
Benefits
Targeted Exercises
Strengthens structures around the knee, improves stability and flexibility
Body Awareness and Modification of Walking Technique
Reduces strain and pressure on the knees, provides relief
Rest and Physical Therapy
Aids healing and recovery, strengthens the knee
Pain Relievers
Temporarily alleviates discomfort
Assistive Devices
Provides support and stability during movement
Surgical Intervention
Addresses underlying causes of knee pain
Conclusion
Knee pain when climbing stairs can be a common and uncomfortable issue that many people face. However, there are effective ways to find relief and manage the discomfort. By gaining a better understanding of the anatomy of the knee and identifying the underlying causes of pain, individuals can take proactive steps towards improving their knee health and finding lasting relief.
Strengthening exercises targeted at the muscles around the knee, along with body awareness and modifying walking techniques, can play a significant role in preventing and reducing knee pain while going up stairs. These strategies can help alleviate the strain on the knee joint and promote better alignment and stability.
It is crucial to listen to your body and seek professional guidance when necessary. Consulting with a healthcare professional or physical therapist can provide valuable insights and personalized recommendations for managing knee pain. They can also offer expert advice on exercises, assistive devices, and other treatment options that can contribute to lasting relief and improved overall knee function.
By taking proactive steps to prevent knee pain, implementing effective management strategies, and prioritizing knee health, individuals can experience significant improvements in their overall quality of life. Remember, finding lasting relief is possible, and with the right approach, you can overcome knee pain and enjoy an active lifestyle.
FAQ
What causes knee pain when climbing stairs?
Knee pain when climbing stairs can be caused by various conditions, including patellofemoral pain syndrome, meniscus tear, chondromalacia patella, IT band syndrome, and muscle imbalance.
How can I relieve knee pain when climbing stairs?
There are several ways to relieve knee pain when climbing stairs, such as targeted exercises to strengthen the knee structures, modifying walking technique, using assistive devices, and seeking professional guidance for treatment and management.
What exercises can help alleviate knee pain when climbing stairs?
Exercises that can help alleviate knee pain when climbing stairs include hip flexor stretches, single-leg lifts, and hamstring stretches, as these exercises strengthen the muscles in and around the knees.
How does body awareness and proper movement alignment help with knee pain on stairs?
Body awareness and understanding proper movement and alignment can help prevent knee pain on stairs by ensuring correct posture and reducing stress on the knee joints.
Are there any over-the-counter pain relievers that can help with knee pain on stairs?
Yes, over-the-counter pain relievers can temporarily alleviate knee pain on stairs, but it is advisable to consult with a healthcare professional to determine the appropriate medication and dosage for your specific condition.
When should I consider surgical intervention for knee pain on stairs?
Surgical intervention for knee pain on stairs may be considered if non-surgical treatments have been ineffective or if there is an underlying structural problem in the knee that requires surgical correction.