The 3D Shaper Technology emerges as a breakthrough solution to combat the silent but debilitating threat of osteoporosis, a bone disease that has long been a major concern for millions of people worldwide. Accurate diagnosis and monitoring of bone health has been paramount in combating this condition.
3D Shaper only looks at the hip. Not the spine.
This chronic condition weakens bones over time, making them fragile and susceptible to fractures. The consequences of osteoporosis can be severe, leading to reduced quality of life, increased risk of disability, and significant healthcare costs. Early detection and effective management are crucial to mitigating the impact of this disease. Enter 3D Shaper Technology, a revolutionary advancement that promises to transform the way we diagnose and treat osteoporosis.
3D Shaper technology, a groundbreaking innovation
This advanced technology, developed by 3D Shaper Medical, a Barcelona-based company, takes the standard 2D DEXA scan and recreates the hip bone in a remarkable 3D representation. This groundbreaking approach makes it possible to extract valuable information about the cortical (hard outer shell) and trabecular (soft inner surface) compartments of the bone – aspects often overlooked by traditional DEXA scans.
By using advanced imaging techniques and statistical modeling, 3D Shaper Technology can transform a generic template into a patient-specific 3D model of the patient. hip bone. This process involves registering the template against the patient’s 2D DEXA scan and adjusting the parameters until perfect alignment is achieved, resulting in an accurate 3D representation. This innovative technology provides healthcare professionals with unprecedented insight into the intricate details of bone structure and density distribution.
Customized treatment plans for optimal bone health
The 3D Shaper Technology provides a fast, safe and cost-effective method for assessing bone density and visualizing local changes in the cortical and trabecular compartments, addressing the limitations of DEXA alone. By providing detailed analysis of the individual compartments of the bone, it enables healthcare professionals to tailor treatment plans and medication choices to the unique needs of each patient. This personalized approach is especially critical when considering potent osteoporosis medications, ensuring the most effective treatment is prescribed from the outset.
Cortical and trabecular compartments
The ability to assess the cortical and trabecular compartments independently provides a more nuanced understanding of bone health. Clinicians can identify local fragility or discrepancies between the two compartments that may have been missed by conventional DEXA scans. Armed with this knowledge, they can make informed decisions about the appropriate course of action, whether that is initiating treatment with a specific medication or modifying an existing regimen.
Advanced Bone Health Monitoring with 3D Shape
One of the key advantages of this technology is its ability to monitor treatment progress with greater accuracy. While DEXA scans can show minimal changes in bone mineral density, the 3D Shaper can detect significant improvements or decreases in the cortical and trabecular compartments – invaluable insights that can inform decisions to modify or continue a treatment regimen. Additionally, the 3D Shaper technology has proven its versatility in assessing the impact of various diseases and medications on bone health.
From chronic kidney disease to breast cancer treatments, this innovative tool provides a comprehensive view of how these conditions and therapies impact the complex components of bone structure. By separating the cortical and trabecular compartments, clinicians can identify specific areas of concern and tailor interventions accordingly, maximizing treatment effectiveness and minimizing potential side effects.
A new era in osteoporosis care
Although 3D Shaper Technology is still in the early stages of adoption in the United States, its potential to revolutionize osteoporosis diagnosis and management is undeniable. As more healthcare facilities embrace this cutting-edge solution, patients will benefit from personalized care, customized treatment plans, and new hope in the fight against this debilitating condition.
The technology’s ability to provide individualized assessments and accurate monitoring allows healthcare professionals to make informed decisions, ultimately improving patient outcomes. In the words of Irma Jennings, an osteoporosis patient navigator who presented the 3D Shaper Technology, “This is an important thing to get out there.” Indeed, the future of osteoporosis care has taken a remarkable step forward, and the 3D Shaper Technology stands as a beacon of hope for millions of people seeking a better understanding and more effective management of this complex disease.
Trends in student-athlete mental health in the National College Health Assessment, 2011-2019.
Edwards B, Froehle AW and Fagan SE. J Athl training. 2023,58(4):361-373. doi: 10.4085/1062-6050-0586.21.
Full text available for free
Take home message
College athletes and non-athletes are under a great deal of stress. Reported mental health symptoms and diagnoses are increasing, with 1 in 3 college students reporting a recent diagnosis. Fortunately, more college students are reporting receiving mental health information from institutions and treatment-seeking behaviors over time.
Background
Awareness of mental health issues is increasing among the general public, including college athletics. Educational efforts and access to mental health resources have increased, but it is unclear whether these efforts have improved student-athletes’ mental health and treatment seeking.
Study Objective
Edwards and colleagues analyzed 8 years of survey data to examine how the mental health of student-athletes, compared to their non-athlete peers, changed between 2011 and 2019.
Methods
Researchers obtained data from the National College Health Assessment. The data, which spanned 8 academic years, were reported anonymously by students at participating institutions. Respondents were classified as “athletes” or “non-athletes” based on their responses to specific survey questions. Researchers excluded students who participated only in club or intramural sports. The survey included “yes” or “no” questions grouped into 5 outcome groups: 1) “recent mental health symptoms,” 2) “recent mental health diagnosis,” 3) “mental health treatment seeking behavior,” 4) “mental health information received from institutions,” and 5) “recent impact of mental health on academic performance.”
Results
A total of 502,780 students from 607 unique institutions completed the surveys and met the inclusion criteria. This included over 54,400 athletes and 448,300 non-athletes. The main results are described in the table, which show that more students received mental health information from institutions and sought treatment or would consider treatment over time. Meanwhile, more students reported recent mental health symptoms/diagnoses and effects on academic performance over time. Student-athletes were less likely to report mental health symptoms/diagnoses and treatment-seeking behavior. However, more student-athletes reported mental health information from institutions.
Changes over time
Differences between groups
Recent mental health symptoms
Increased over time
Athletes < Non-athletes
Recent mental health diagnosis
Increased over time
Athletes < Non-athletes
Behavior Seeking Treatment for Mental Health
Improved over time
Athletes < Non-athletes
Receiving mental health information from institutions
Improved over time
Athletes > Non-athletes
The Recent Impact of Mental Health on Academic Performance
Increased over time
Athletes < Non-athletes
Positions
More than 1 in 5 students reported symptoms of depression. A majority of students reported feeling very sad, very lonely, exhausted, or overwhelmed. Over the 8 years, we went from 1 in 5 students reporting a diagnosis of a mental health condition to 1 in 3 students. It is encouraging that treatment seeking behaviors and access to mental health information have increased over time. This study cannot address whether the increased symptoms/diagnoses of mental health are due to increased prevalence or increased ease of reporting. As access to educational materials increases, it would stand to reason that reporting of mental health issues would also increase. While the trends over time are encouraging, the overall numbers are still discouraging and we need to do more to encourage student-athletes to seek treatment.
Clinical implications
Clinicians need to know that athletes and non-athletes are under immense pressure due to the college experience. This requires clinicians to be fully aware of the signs and symptoms of mental health issues and have an appropriate and empathetic plan to help their athletes get the right treatment. We must also continue to reduce stigma and increase awareness among athletes that treatments are available.
Questions for discussion
What changes have you observed regarding mental health awareness, recognition, and treatment in student-athletes? What specific strategies do you think have had the most impact on mental health awareness, recognition, or treatment in student-athletes?
Written by Kyle Harris Reviewed by Jeffrey Driban
related posts
You are not alone – Depression, stress and anxiety in the sports medicine team Specializing in sports in high school may increase risk of depression Many NCAA Clinicians Fail to Screen for Mental Health Fresh air can improve performance. Want to get better? Take a nap!
What if the key to better health was right under your nose?
We’re going to explore the hidden power of something you do 22,000 times a day, without even thinking about it…
To breathe.
Come with me as I sit with you Stefanie Broesan expert in pharmaceutical sciences, who’s here to reveal how a simple change in the way you breathe could be the game-changer you didn’t know you needed – for your sleep, your stress levels and even your bones.
We introduce you to Moonbird, a revolutionary device making waves in the world of wellness, and explain why everyone from insomniacs to patients with osteoporosis pay attention to this old practice with a modern twist.
Episode Timeline
0:00 – Episode Beginning
2:27 – Meet Stefanie Broes, CEO and co-founder of Moonbird
3:45 – Explanation of the science behind breathing techniques and their impact on overall health and well-being
05:50 – How breathing techniques help reduce stress and anxiety, and why it’s important for people with osteoporosis
8:22 – Details about the Moonbird device: what it is, how to use it, and how it helps with stress and insomnia
10:52 – How Moonbird is different from other health technology products on the market
12:10 – How breathing exercises can improve sleep quality, especially in older adults, and their benefits for bone health
14:34 – The importance of sleep for bone health, including the risks associated with sleep deprivation and its impact on bone formation and remodeling
15:58 – Real success stories from Moonbird users
18:12 – Simple breathing exercises that listeners can begin to improve their health and well-being
19:32 – Future plans for Moonbird and the future of breathwork in the health tech industry
21:19 – Recommendation of the book “Breath” by James Nestor for more insight into the importance of breathing
21:48 – Special offer and where to find more information about Moonbird products
What can you do to support your bone health and this podcast?
1. Click the “Subscribe” button on your respective podcast player (e.g. Apple, Google, Spotify, Stitcher, iHeart Radio, and TuneIn). Never miss an episode that can help improve your bone health.
2. Leave a review. The more positive ratings and reviews and the more subscribers we have, the more people can find us and get the answers to the questions they need. Thank you! 🙂
3. Tell a friend about The Bone Coach Podcast or share via text, email, or social. Know of a Facebook group where people could benefit from this info? Feel free to click one of the share buttons below.
About Stefanie Broes:
Stefanie is the CEO and co-founder of Moonbird, a health tech startup operating in the wellness sector. Moonbird is the world’s first wearable breath pacer and is all about making breathwork accessible so people can live healthier, happier lives.
The product is used to reduce stress, manage anxiety and combat insomnia. Stefanie has a medical background, a PhD in pharmaceutical sciences and a master’s degree in IP and data protection law. When she discovered how effective breathing exercises are in tackling her own insomnia, she delved deeper into the subject and eventually started the company to help more people discover the positive effects of slow breathing.
Medical disclaimer
The information shared above is for informational purposes only and is not intended to provide medical or nutritional advice; it does not diagnose, treat, or cure any disease, condition; it should not be used as a replacement or substitute for medical advice from physicians and trained medical professionals. If you are under the care of a healthcare professional or are currently taking prescription medications, you should discuss any changes to your diet and lifestyle or possible use of dietary supplements with your doctor. You should not discontinue any prescribed medications without first consulting your doctor.
Curovate is a physical therapy app for ACL injury, ACL surgery, knee replacement, knee bracing, hip bracing, and hip replacement. This blog focuses on how to seamlessly sign up for Curovate once you have downloaded the app and are ready to start using it. To download the app, simply click on one of the Apple App Store or Google Play Store links at the top or bottom of this page.
How to Sign Up for Curovate: The One-Click Sign Up Method
When you open Curovate, you can use Apple, Google or Meta (also known as Facebook) as a one-click method to create an account with Curovate. These three one-click methods make it easy for you to start an account with Curovate using an existing account. The advantage of this is that you don’t have to remember another username and password to log in to Curovate!
For Apple, you just need to enter your Apple ID and password to create an account with Curovate.
For Google, you will need your Gmail address and password.
For Facebook or Meta you will need your Facebook ID and password.
Curovate keeps your health data safe
You can rest assured that even though we offer these one-click sign in methods, Curovate is committed to keeping your health data safe. We do not share your data with Apple, Meta, or Google, nor do we sell, trade, or share your data with any other company.
Alternative registration method: Create a Curovate username and password
If you prefer not to use Apple, Meta, or Google to sign in to Curovate, you can create an account using your email address and a secure password. To sign in using this method:
Enter your email address. A verification code will be sent to this email address.
Verify your email by going to your email inbox, finding the verification code that was sent to you, and entering the code into the Curovate app. If you don’t receive an email in your inbox, check your “junk” “spam” and “social” folders, as the verification code may be mistakenly classified as junk.
Once you verify your email address, you can create a new email address and password specific to your Curovate account.
Watch the video below for a step-by-step guide with a screen capture directly from the Curovate Physical Therapy app, showing you how to log into the Curovate app.
What information is required to create a Curovate account?
Curovate will ask you for your date of birth and gender to complete the creation of your account. Once you provide this information, you will be redirected to a screen that asks you to enter your surgery and injury information:
You will be asked what injury or surgery you are recovering from or what body part you are trying to strengthen. For example, if you had a knee replacement, select “total knee replacement” from the surgery options.
You will then be asked to select the date of your surgery and the date of your injury. It is important that you enter the most accurate information about your surgery as this will be used to place you in the correct physiotherapy exercise phase in the app. When you are in the correct exercise phase, you will be able to complete exercises and rehabilitation that take into account your current abilities.
After entering your surgery or injury date, it will take a few seconds for Curovate to load your rehabilitation protocol. This rehabilitation protocol consists of daily exercise videos, progress tracking of all your exercises, the ability to measure your knee or hip range of motion, the option to ask a physiotherapist questions via our in-app chat or book a 1-on-1 physiotherapy appointment.
On the Curovate home screen you can see which stage of your recovery you are in.
Select “play day 1” to see the exercise list and videos needed to complete that day. Review the phase goals and daily exercises to make sure they are appropriate and not too challenging. We have a great video to show you how to use Curovate if the exercises in your beginning phase are too challenging. We also have a video to show you how to use Curovate if the exercises in your beginning phase are too easy.
Want to learn more about how to switch phases when exercises are too easy or too hard? Check out our blogs on How to use Curovate when exercises are too easy? and How to use Curovate when exercises are too hard?
How many days of training are in each Curovate phase?
Each phase has seven days. In the seven days, the exercises are the same. Each day, you will be given a list of equipment that you will need to complete the exercises. You will also have access to a concise exercise program in case you do not have enough time to complete the entire exercise session. Each exercise phase contains different exercises. Only phase one (1) has one day of exercise, all other phases have seven days. You must complete each day in full so that the app can move you to the next day. After you have completed all seven days of exercise, the app will move you to the next exercise phase.
How do I play all the exercises assigned to me within a practice phase every day?
Selecting ‘Play All’ will play all the exercise videos in a session. A session can be morning, afternoon and evening. Some phases have 3 sessions and some have 2 or just one per day. If you complete all the assigned exercises within the day, the app will mark all your exercises as complete and you will move on to day two. Completing all the assigned exercises regularly will help you progress in your recovery journey, so do your best!
The Curovate app gives you guided exercises, rehab reminders, progress tracking, and can even measure your range of motion, all from your phone. To get started, simply download the Curovate app for iOS or Android from one of the links below.
If you need additional tailored help during your surgery or recovery from an injury, check out our Virtual Physiotherapy page to book your 1-on-1 video session with a physiotherapist.
Zoals besproken in een eerdere blog over botafbraakde processen van botmodellering en botremodellering kunnen worden beschreven als een gecoördineerde interactie tussen stamcellen, osteocyten, osteoblasten en osteoclasten. Of bot modellering of remodellering is, hangt af van de balans tussen de resorptie van bestaand bot en de vorming van nieuw bot.
Dezelfde cellen die bij deze processen betrokken zijn, spelen ook een rol bij de genezingsreactie op bottransplantaatmaterialen. Nadat bottransplantaatmateriaal tijdens een operatie bij een patiënt is geïmplanteerd, begint de botvormingsreactie met de vorming van nieuw bot op het transplantaatoppervlak en vervolgens via de porositeit ervan, indien aanwezig. Naarmate er meer bot het implantaatgebied vult, zullen de cellen het transplantaatresorptieproces initiëren. Uiteindelijk is het doel van het geïmplanteerde transplantaatmateriaal om volledig te worden opgevuld met nieuw bot en na verloop van tijd volledig te worden geresorbeerd.
Ongeacht het type bottransplantaatmateriaal dat bij een patiënt is geïmplanteerd, speelt de snelheid waarmee dat transplantaat resorbeert een belangrijke rol in het genezingsproces. De meeste transplantaten resorberen met een vaste snelheid, bepaald door hun materiaalsamenstelling. In tegenstelling tot andere synthetische middelen op de markt, is de geavanceerde TrelCor van Biogennix®-gebaseerde transplantaatmaterialen zorgen voor een optimale resorptie in twee fasen die aansluit bij de unieke botvormingssnelheid van de patiënt. In deze blog wordt het proces van TrelCor-resorptie en de gunstige effecten ervan op het genezingsproces gedetailleerd beschreven.
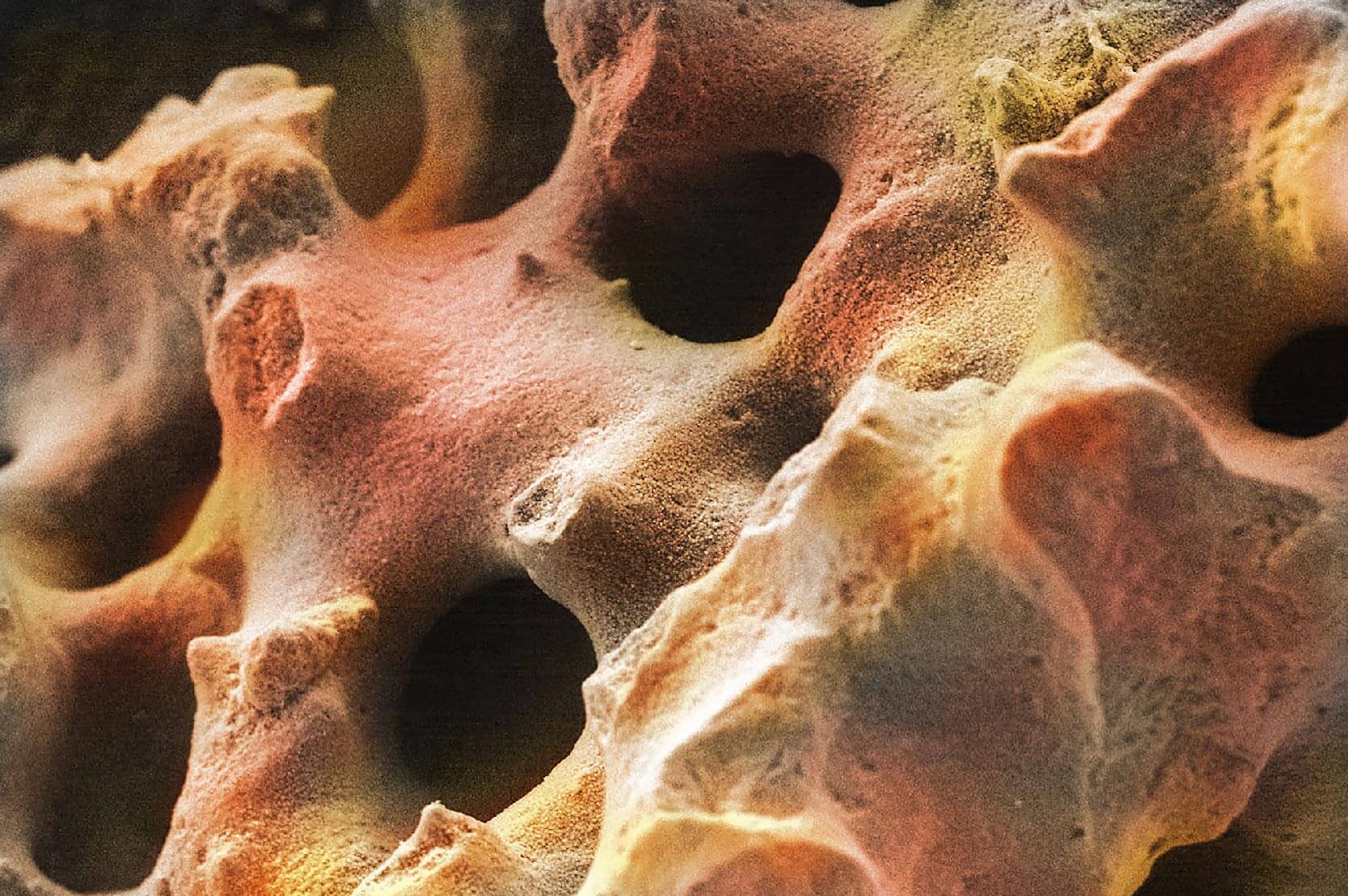
Voordat we leren hoe de tweefasenresorptie van TrelCor plaatsvindt, gaan we eerst kijken hoe resorptie er radiografisch uitziet. Nadat een bottransplantaatproduct chirurgisch is geïmplanteerd bij een patiënt, willen clinici mogelijk de resorptie van het transplantaat beoordelen om te weten hoe goed de patiënt geneest na de operatie. Meestal gebruiken chirurgen röntgenfoto’s (röntgenfoto’s) of computertomogrammen (CT’s) om te zien wat er in de patiënt gebeurt in de loop van de tijd. Afhankelijk van de samenstelling van een bottransplantaatmateriaal kan de zichtbaarheid ervan op röntgenfoto’s/CT’s variëren van radiolucent (niet zichtbaar) tot radiopaak (zichtbaar). Tijdens de operatie en bij vervolgafspraken van de patiënt is het waardevol om een relatief radiopaak transplantaatmateriaal te hebben dat visueel kan worden geïdentificeerd. Hierdoor kunnen clinici eenvoudig de exacte plaats zien waar het transplantaatmateriaal is geplaatst en de botvorming in dit gebied in de loop van de tijd volgen.
Sommige transplantaatmaterialen, zoals TrelCor, zijn zichtbaar op een röntgenfoto. Dankzij deze eigenschap kunnen clinici de voortgang van botvorming in de loop van de tijd visualiseren. Direct na implantatie hebben op TrelCor gebaseerde transplantaatmaterialen een gegranuleerd radiografisch uiterlijk met duidelijke randen. Naarmate er nieuw bot begint te vormen op het oppervlak en binnen de porositeit van TrelCor, worden de randen van het implantaat minder gedefinieerd. Vervolgens, naarmate resorptie van het transplantaatmateriaal optreedt en de hoeveelheid nieuw bot toeneemt, is het transplantaat niet langer zichtbaar en lijkt de plek volledig opgevuld met het eigen bot van de patiënt.
Tdoor Materiaal SamenstellingN
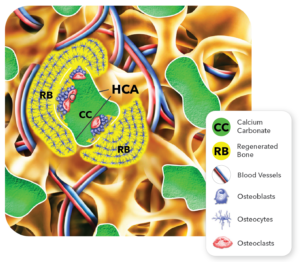
Figuur 1: SEM-beelden van de HCA-oppervlaktelaag op TrelCor-korrels (rechtsboven) en dwarsdoorsnede van TrelCor-korrels waarop de HCA-oppervlaktelaag en de calciumcarbonaat (CC)-kern te zien zijn (rechtsonder).
Bij standaard keramische synthetische bottransplantaatmaterialen bepaalt de samenstelling van het transplantaatmateriaal of het transplantaat snel of langzaam zal resorberen. Bijvoorbeeld hydroxyapatiet (HA) [Ca10(PO4)6(OH)2] en tricalciumfosfaat (TCP) [Ca3(PO4)2] zijn beide calciumfosfaatkeramieken die vaak worden gebruikt als bottransplantaatmaterialen. Hun verschillende samenstellingen resulteren in een langzame resorptiesnelheid voor HA (~1% per jaar) en een snellere resorptiesnelheid voor TCP (6-24 maanden). Deze resorptietijden zijn inherent aan de materialen en kunnen alleen worden gewijzigd door HA en TCP te combineren (bifasisch calciumfosfaat – BCP) of door de structuur van het bottransplantaat aan te passen, wat invloed heeft op het oppervlak voor botgroei en resorptie.
TrelCor verschilt van standaard HA- of TCP-bottransplantaten doordat het een samenstelling met twee regio’s heeft: het oppervlak bestaat uit hydroxycarbanoapatiet (HCA) [Ca10(PO4)x(CO3)y(OH)z] en de kern is calciumcarbonaat (CaCO3) (Figuur 1). Omdat HCA langzamer resorbeert vergeleken met calciumcarbonaat, wordt de resorptie van TrelCor direct gecontroleerd door de dikte van het langzamer resorberende HCA-oppervlak. Als gevolg hiervan, de dikte van de HCA-laag werd geoptimaliseerd tot ~5MMwat voldoende tijd biedt voor botgroei om over het oppervlak te ontstaan voordat het volledig wordt geresorbeerd. Deze combinatie van HCA en calciumcarbonaatsamenstelling stelt TrelCor in staat om een patiëntspecifieke respons te bieden.
Hoe Dual-Stage ResoRptie van TrelCor Okomt voor
Patiënten resorberen en hermodelleren bot met verschillende snelheden op basis van hun leeftijd, gezondheid, de grootte van het botdefect en andere factoren. Het ideale resorptieprofiel is er een dat kan worden gecontroleerd door de eigen botvormingssnelheid van elke patiënt. Bijvoorbeeld, kleine, ingeperkte defecten bij kinderen zullen waarschijnlijk sneller bot regenereren, dus een sneller resorberend transplantaat zou ideaal zijn. Omgekeerd zou botvorming bij een oudere patiënt die een grote, complexe spinale fusie ondergaat, plaatsvinden met een langzamer tempo. In dit geval zou een optimaal transplantaat langer meegaan en een langzamere resorptiesnelheid hebben om overeen te komen met de langzamere botvormingssnelheid van de patiënt.
Het doel van een resorbeerbaar bottransplantaatproduct is om te functioneren als een steiger zolang het duurt om nieuw bot te vormen. Pas dan zou de steiger moeten beginnen met resorberen. Met dit in gedachten is TrelCor specifiek ontworpen om te resorberen naarmate het bot in de porositeit en op het oppervlak groeit. Zoals behandeld in Blog19osteoblasten (botvormende cellen) signaleren de vorming van osteoclasten (bot- en transplantaatresorberende cellen), en vice versa. Het onderstaande proces en Figuur 2 beschrijf gedetailleerd hoe de twee-fase resorptie van TrelCor-gebaseerde transplantaatmaterialen plaatsvindt:
Na de implantatie vindt in eerste instantie botvorming plaats op het TrelCor-materiaal dat direct in contact staat met het omliggende bot. Figuur 2: Belangrijke gebeurtenissen die optreden tijdens botregeneratie en resorptie van TrelCor-bottransplantaatproducten.
Botgroei verloopt geleidelijk over het oppervlak van het TrelCor-poriesysteem totdat de gehele korrel bedekt is met nieuw bot. Dit proces gaat door naar elke aangrenzende korrel.
Naarmate het bot op het oppervlak van de TrelCor-korrels dikker wordt, geven de osteoblasten in dit nieuwe botgebied een signaal aan de osteoclasten om met het resorptieproces te beginnen.
Eenmaal geactiveerd, beginnen de osteoclasten de HCA-oppervlaktelaag te resorberen. Omdat het HCA-oppervlak langzamer resorbeert, geeft dit de botvormingsreactie voldoende tijd om het TrelCor-oppervlak volledig te bedekken en de porositeit op te vullen.
Nadat de osteoclasten het HCA-oppervlak hebben doorbroken, beginnen ze agressief het onderliggende calciumcarbonaat te resorberen.
Vervolgens vindt er nieuw botvorming plaats in het calciumcarbonaatgebied.
Uiteindelijk resorberen osteoclasten het hele transplantaat en is het proces voltooid. Het gebied dat ooit werd ingenomen door het TrelCor-transplantaat is nu volledig vervangen door bot.
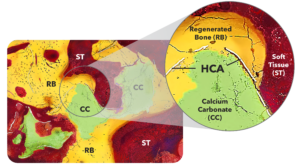
Dit effect is duidelijk te zien inhistologie afbeeldingen vanin vivo-onderzoeken dietonende helende reactievan TrelCor materialen. In één onderzoek werd TRelCor werd gecombineerd in een 1:1 verhouding met autograft en geïmplanteerd in de posterolaterale wervelkolom van konijnen. Na 12 wekenbeide een prominent bot formatie respons was zichtbaar, zoals wasde resorptie antwoord. Dit tijdstip legde specifiek de initiële resorptie van de HCA-laag en de penetratie van nieuw bot in het calciumcarbonaatgebied vast. Figuur 3 toont een SEM-histologie afbeelding die gekleurd is om de nadruk te leggenzedit effect. Op deze afbeelding, de dubbele samenstelling van TrelCor korrel is zichtbaar met het calciumcarbonaat (groente) en het HCA-oppervlak (wit). Bot (geel) is Ook gezien groeien op het oppervlak van de korrels en doordringend het calciumcarbonaatgebied.
Figuur 3: Histoloogik ik benleeftijd die botvorming laat zien in porositeit,inbreuk makenG van TrelCor HCA-laag, En resorptie van calciumcarbonaatkern gevolgd door extra bot vorming.
Voordelen van Dual-StageBottransplantaat Resorptie
Resorptie van bottransplantaatmaterialen is belangrijk omdat bottransplantaten voornamelijk functioneren als een steiger voor nieuwe botgroei. Als de steiger te snel resorbeert (voordat de botvorming is voltooid), kan er een holte ontstaan en kan de operatie mislukken. Als het te langzaam resorbeert, neemt het implantaat ruimte in die moet worden opgevuld met nieuw bot.
Zoals blijkt uit het TrelCor-resorptieproces, kan de balans tussen botvorming en -resorptie worden geregeld door de dikte van het HCA-gebied. Met tientallen jaren ervaring hebben wetenschappers van Biogennix de dikte van de HCA-laag verfijnd om een geavanceerd bottransplantaatmateriaal te creëren met een optimaal resorptieprofiel dat is afgestemd op elke patiënt, d.w.z. “geduldig-gecontroleerde” resorptieDeze geavanceerde bottransplantaateigenschap is uniek voor TrelCor; geen enkel ander bottransplantaatproduct op de markt bezit deze mogelijkheid.
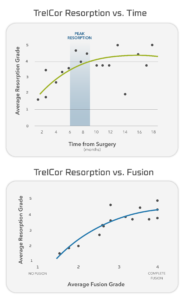
Figuur 4: Fusieresorptiegegevens van klinische onderzoeken met 60 patiënten studie. (Gegevens in bestand)
Bij de tweefasen-resorptierespons van TrelCor worden er uiteindelijk meer osteoclasten geactiveerd als een patiënt snel bot vormt, bijvoorbeeld bij een jonge gezonde patiënt. Dit versnelt de resorptie van de TrelCor HCA-laag en maakt extra botvorming in het calciumcarbonaatgebied mogelijk. Omgekeerd, als de patiënt bot vormt in een langzamer tempo, bijvoorbeeld bij een oudere diabetespatiënt, vertraagt de osteoclastactivatie ook. Dit geeft de botvormingsrespons voldoende tijd om in zijn eigen tempo te vorderen en uiteindelijk de porositeit van TrelCor op te vullen. In dit langzamere genezingsproces treedt het osteoclastproces volledig in werking zodra er voldoende bot is gevormd en maakt het verdere botvorming in het calciumcarbonaatgebied mogelijk.
Dit “patiëntgecontroleerde” resorptie werd gezien in een multicenter klinische studie met 60 patiënten die de fusie- en resorptierespons van TrelCor-bottransplantaatmateriaal evalueerde dat was geïmplanteerd met autograft bij patiënten met spinale fusie. In deze studie werden zowel fusie als resorptie radiografisch beoordeeld en gescoord op een schaal van 1-4 (1 = geen fusie/resorptie; 4 = volledige fusie/resorptie). Zoals getoond in Figuur 4de progressie van fusies is direct gerelateerd aan de progressie van resorptie met een piekresorptie die over het algemeen optreedt na 6-9 maanden. Deze studie bevestigde de effectiviteit van de dual-stage resorptie van TrelCor.
De verschuiving Richting Geavanceerde synthetische bottransplantaatproducten
Terwijl de meeste commercieel verkrijgbare bottransplantaatproducten worden geresorbeerd met een vaste snelheid op basis van hun materiaal samenstellingNext-generatie geavanceerd bottransplantaten werden ontworpen om meer te doen. Geavanceerde synthetische producten zoals TrelCor-gebaseerde bottransplantaatproducten bieden uniekEigenschappen waar chirurgen, ziekenhuizen en vooral patiënten baat bij hebben. TrelCor-bottransplantaten met hun tweefasensamenstelling zorgen voor een optimale “patiëntgecontroleerde” resorptie,wat aanzienlijke voordelen biedt ten opzichte van ‘one-size-fits-all’” eerste generatie materialen die vandaag de dag nog steeds worden gebruikt. Het is geen verrassing dat de markt steeds meer een verschuiving zien naar meer geavanceerde synthetische bottransplantaatmaterialendie bieden duidelijke voordelen ten opzichte van technologieën van de eerste generatie.
Knee pain just below the knee cap can be a real bother. It can stop you from doing the things you love. Knowing what causes this pain and how to treat it can help you get back to your normal activities. This article will explain the common causes, symptoms, and treatments for this type of knee pain. It will also tell you how to prevent it and when to see a doctor.
Key Takeaways
Knee pain below the knee cap can be caused by different conditions like patellar tendinitis, Osgood-Schlatter disease, and chondromalacia patella.
Symptoms of this pain include discomfort during physical activities, swelling, tenderness, and trouble moving the knee.
Doctors use physical exams, imaging tests, and medical history reviews to find out what’s causing the pain.
Non-surgical treatments include physical therapy, medications, and changes in lifestyle, while severe cases might need surgery.
Preventive steps like proper warm-up, strengthening exercises, and wearing the right shoes can help avoid knee pain.
Common Causes of Knee Pain Just Below the Knee Cap
Patellar Tendinitis
Patellar tendinitis, often called jumper’s knee, is a common cause of pain just below the knee cap. This condition happens when the tendon connecting the kneecap to the shinbone gets inflamed. Athletes who do a lot of jumping or running are more likely to get this injury. The pain usually gets worse with physical activity.
Osgood-Schlatter Disease
Osgood-Schlatter disease is another reason for knee pain below the knee cap. It mostly affects kids and teens who are growing fast. The pain comes from swelling and irritation at the top of the shinbone, where the patellar tendon attaches. This condition often happens during growth spurts and can be very painful.
Chondromalacia Patella
Chondromalacia patella is when the cartilage under the kneecap gets soft or wears down. This can cause pain and a grinding feeling when moving the knee. People who do a lot of knee-bending activities, like running or squatting, are more likely to have this problem. Rest and physical therapy can help manage the symptoms.
If you have knee pain that doesn’t go away, it’s important to see a doctor. They can help find out what’s causing the pain and suggest the best treatment.
Symptoms Associated with Knee Pain Below the Knee Cap
Pain During Physical Activity
Feeling pain just below the knee cap is common during physical activities like running, jumping, or climbing stairs. This pain often worsens with more intense activities and can make it hard to continue exercising.
Swelling and Tenderness
Swelling around the knee cap area is another symptom. The area might feel tender to the touch, and you may notice it looks puffier than usual. This swelling can make it uncomfortable to move the knee.
Difficulty in Knee Movement
Having trouble moving your knee smoothly is a sign of pain below the knee cap. You might find it hard to bend or straighten your knee fully. This can affect daily activities like walking, sitting, or standing up.
If you experience any of these symptoms, it’s important to pay attention to your body and consider seeing a doctor for advice.
Diagnosing Knee Pain Below the Knee Cap
Physical Examination
A doctor will start by looking at your knee. They will check for any swelling, tenderness, or unusual movements. They might ask you to move your knee in different ways to see what hurts.
Imaging Tests
Sometimes, doctors need to see inside your knee. They might use X-rays, MRIs, or CT scans. These tests help them find out if there are any problems with the bones or tissues.
Medical History Review
Your doctor will ask about your past health. They will want to know if you have had any injuries or illnesses before. This helps them understand why your knee hurts now.
It’s important to tell your doctor everything about your knee pain. This will help them find the best way to treat it.
https://www.youtube.com/embed/_cbu-W3YuP4
Non-Surgical Treatments for Knee Pain Below the Knee Cap
Physical Therapy
Physical therapy is often the first step in treating knee pain below the knee cap. A therapist will guide you through exercises that strengthen the muscles around your knee, improving stability and reducing pain. Regular sessions can make a big difference in your recovery.
Medications
Over-the-counter pain relievers like ibuprofen or acetaminophen can help manage pain and reduce inflammation. In some cases, your doctor might prescribe stronger medications. Always follow the dosage instructions to avoid side effects.
Lifestyle Modifications
Making changes to your daily routine can also help. This might include losing weight to reduce stress on your knees, wearing supportive footwear, and avoiding activities that worsen the pain. Simple adjustments can lead to significant improvements in your knee health.
Consistency in following these non-surgical treatments can greatly enhance your quality of life and help you avoid more invasive procedures.
Surgical Options for Severe Knee Pain Below the Knee Cap
Arthroscopy
Arthroscopy is a minimally invasive surgery where a small camera is inserted into the knee joint. This allows the surgeon to see inside the knee and fix any problems. This procedure often results in quicker recovery times compared to traditional surgery.
Realignment Procedures
Realignment procedures are done to correct the position of the kneecap. This helps to reduce pain and improve function. These surgeries can be more complex and may require a longer recovery period.
Cartilage Restoration
Cartilage restoration aims to repair or replace damaged cartilage in the knee. This can involve different techniques, such as grafting new cartilage into the knee. Successful cartilage restoration can significantly improve knee function and reduce pain.
For those suffering from severe knee pain, surgical options can offer a path to relief and improved quality of life. Always consult with a healthcare professional to determine the best course of action.
Preventive Measures to Avoid Knee Pain Below the Knee Cap
Proper Warm-Up Techniques
Before engaging in any physical activity, it’s crucial to perform a proper warm-up. This helps prepare your muscles and joints for the exercise ahead. A good warm-up can reduce the risk of injury and improve your overall performance. Spend at least 5-10 minutes on light aerobic exercises like jogging or brisk walking, followed by dynamic stretches.
Strengthening Exercises
Strengthening the muscles around your knee can provide better support and reduce the strain on your knee cap. Focus on exercises that target your quadriceps, hamstrings, and calves. Simple exercises like squats, lunges, and leg presses can be very effective. Aim to include these exercises in your routine at least 2-3 times a week.
Appropriate Footwear
Wearing the right shoes is essential for preventing knee pain. Choose footwear that offers good arch support and cushioning. Avoid wearing worn-out shoes, as they can lead to improper alignment and increase the risk of knee injuries. If you participate in specific sports, consider getting sport-specific shoes designed to provide the necessary support and protection.
Taking these preventive measures seriously can help you avoid knee pain and maintain an active lifestyle. Remember, it’s always better to prevent an injury than to treat one.
When to Seek Medical Attention for Knee Pain Below the Knee Cap
Persistent Pain
If knee pain doesn’t go away after a few days of rest and home care, it might be time to see a doctor. Ignoring ongoing pain can lead to more serious issues. It’s important to get a professional opinion to avoid long-term damage.
Inability to Bear Weight
When you can’t put weight on your knee without feeling pain, it’s a clear sign that something is wrong. This could mean a serious injury that needs medical attention. Don’t try to push through the pain; instead, get it checked out.
Signs of Infection
If your knee is red, warm, and swollen, you might have an infection. Other signs include fever and chills. Infections can get worse quickly, so it’s important to see a doctor right away if you notice these symptoms.
It’s always better to be safe than sorry. If you’re unsure about your knee pain, a quick visit to the doctor can give you peace of mind and help you get back to your normal activities faster.
Conclusion
Knee pain just below the knee cap can be a real bother, but understanding its causes and treatments can help you manage it better. Whether it’s due to overuse, an injury, or a medical condition, knowing what you’re dealing with is the first step. Simple treatments like rest, ice, and exercises can often make a big difference. But if the pain doesn’t go away, it’s important to see a doctor. Taking care of your knees now can help you stay active and healthy in the future.
Frequently Asked Questions
What causes pain just below the knee cap?
Pain just below the knee cap can be caused by conditions like patellar tendinitis, Osgood-Schlatter disease, or chondromalacia patella.
What are common symptoms of knee pain below the knee cap?
Common symptoms include pain during physical activity, swelling and tenderness, and difficulty moving the knee.
How is knee pain below the knee cap diagnosed?
Doctors diagnose this type of knee pain through physical exams, imaging tests like X-rays, and reviewing your medical history.
What are non-surgical treatments for knee pain below the knee cap?
Non-surgical treatments include physical therapy, medications, and lifestyle changes like avoiding activities that cause pain.
When should I see a doctor for knee pain below the knee cap?
You should see a doctor if you have persistent pain, can’t bear weight on your knee, or notice signs of infection like redness and warmth.
How can I prevent knee pain below the knee cap?
You can prevent this kind of knee pain by doing proper warm-ups, strengthening exercises, and wearing the right footwear.
This month’s bulletin begins with a study that could lead to a new drug for osteoporosis. We’ll explore what researchers have discovered and how it could impact the future of bone health.
Next, you’ll learn about a study on the health effects of ultra-processed foods. Cognitive decline may be more related to eating TV dinners than watching TV.
Finally, we discuss a study published in the journal Osteoporosis International that measured the benefits of outdoor walking on bone health. Get your sneakers ready, because these results will inspire you to get out of the house and hit the trails!
Natural protein investigated as potential drug against osteoporosis
Researchers at the University of Birmingham in the UK have discovered that a short protein called PEPITEM (Peptide Inhibitor of Trans-Endothelial Migration) can be turned into a new drug against osteoporosis.
In the study, PEPITEM was administered to laboratory mice to study the protein’s impact on their bones. The researchers found that PEPITEM therapy significantly increased bone volume and thickness in both the tibia and vertebrae of adult mice. They also observed the effects of PEPITEM on osteoblast cells in the laboratory and found that the protein increased the activity of the bone-forming cells.
Relevant fragment
“…the key test for a potential new therapy is its ability to target the natural repair process that is impaired by age or inflammatory disease. Here, the researchers showed that giving extra PEPITEM limits bone loss and improves bone density in animal models of menopause, which is a common trigger for osteoporotic bone loss in humans. Their studies also showed similar findings in models of inflammatory bone disease (arthritis), where PEPITEM significantly reduced bone damage and erosion.”1
This discovery provides useful information about how our bodies regulate the bone remodeling process, but also carries unknown risks as a potential new drug. PEPITEM is likely to enter human trials, which will begin to reveal what unintended side effects are caused by pharmaceutical applications of the protein.
Short content
Scientists in the UK have identified a protein called PEPITEM and found that the compound increases the volume and thickness of bone in studies with mice. The researchers suggest that PEPITEM could be turned into an osteoporosis drug that increases osteoblast activity to improve bone density.
Ultra-processed foods linked to stroke and cognitive decline
A new study published in the May 22, 2024, online edition of Neurology links ultra-processed foods to an increased risk of stroke and cognitive decline. Ultra-processed foods are high in added sugar, fat, and salt, and low in protein and fiber.
The study followed 30,239 people aged 45 or older for an average of 11 years. Participants completed a food questionnaire that was used to calculate the percentage of their daily diet that consisted of ultra-processed foods.
Relevant fragment
“After adjusting for age, sex, high blood pressure and other factors that may influence dementia risk, researchers found that a 10% increase in the amount of ultra-processed foods eaten was associated with a 16% higher risk of cognitive impairment.
They also found that eating more unprocessed or minimally processed foods was linked to a 12% lower risk of cognitive impairment.”2
Similar to the results for cognitive impairment, a higher intake of ultra-processed foods was associated with an 8% higher risk of stroke. Participants with a higher intake of unprocessed or minimally processed foods had a 9% lower risk of stroke.
These findings underscore the value of the Osteoporosis Reversal Program’s 80/20 pH-balanced diet. Processed foods are acidifying, so they are naturally limited by a diet that consists of only 20 percent acidifying foods. Additionally, the Save Institute recommends avoiding processed foods as much as possible.
Short content
A study in the online journal Neurology found that participants who ate higher amounts of ultra-processed foods had a higher risk of stroke and cognitive impairment. All processed foods are acidifying, so they are naturally limited by an 80/20 pH-balanced diet, but they should also be avoided as much as possible.
Walk to stronger bones
A study published in Osteoporosis International analyzed the outdoor walking habits of 24,700 older adults and their risk of osteoporosis. They also looked at participants’ genetic predisposition to osteoporosis.
Researchers divided the participants into four groups:
those who did not go outside
those who walked 30 minutes or less
those who walked 30-60 minutes
those who walked 60 minutes or more
The study included 37 months of follow-up, during which time researchers found a significant negative correlation between daily outdoor walking and the risk of osteoporosis incidence. The reduction in osteoporosis risk was directly correlated with the length of the walks, ranging from 14 percent to as much as 40 percent for those who walked the most.
Relevant fragment
“Researchers also found a “decreasing trend” in osteoporosis risk among participants with both low and high genetic predispositions – meaning that regardless of whether osteoporosis runs in your family, a daily walk may help strengthen bones. Note: If you have a family history of osteoporosis, it may be especially helpful to walk for an hour every day: the researchers found that participants with a high genetic risk who walked outdoors for more than 60 minutes experienced the greatest reduction in their risk.”3
Walking is a weight-bearing exercise that promotes bone formation. It is notable that this study specifically examined outdoor walking. Exposure to greenery and the outdoors has a positive impact on both well-being and bone health.
Regardless of how much or how little you currently walk, you can increase the benefit by adding extra distance, frequency, or intensity to your walks. Additionally, choosing a greener walking path can amplify the positive effects of your walk.
Short content
A study of older adults found that those who spent the most time outdoors (more than 60 minutes per day) had the lowest risk of osteoporosis. This risk reduction was also effective for people who were genetically predisposed to osteoporosis.
What this means for you
Our bodies are complex biological systems that are sensitive to many inputs. That sensitivity is one reason why drugs are such a risky proposition: they cause changes and effects that are not intended or desired. But it is also why natural strategies to improve our health have such far-reaching positive effects. A balanced diet of whole foods and regular exercise can keep your bones strong and your life active.
The Osteoporosis Reversal Program provides a comprehensive approach to strengthening your bones and reducing your risk of fractures, without the risks of medications.
You have an incredible amount of resources at your disposal. Use what you have learned to create the future you deserve.
Experiencing pain can be a part of life, but living with chronic pain is far from normal. It can be exhausting and affect your ability to live an active life, perform tasks, and get the rest you need. Persistent pain can lead to anxiety, insomnia, and depression. Physical therapy can often reduce or eliminate pain so you can get back to living your life.
What is chronic pain syndrome?
There are two primary categories of pain. Acute pain is often a symptom of an underlying health condition. Recovery can take days to weeks and the pain subsides. Chronic pain, or chronic pain syndrome, on the other hand, usually lasts six months or longer. It occurs in addition to the pain caused by the health condition, which may or may not have healed. It is independent of the original injury or illness that began and can persist long after the pain has gone.
Chronic pain can present in different forms, such as:
Back and neck pain
Joint or arthritis pain
Cancer pain near a tumor
Pain in the testicles
Headache, including migraine
Pervasive muscle pain (including fibromyalgia)
Persistent pain in scar tissue
Neurogenic pain due to damage to the nervous system
More than20% of Americans have chronic pain that affects your work and lifestyle.
What causes chronic pain?
Sometimes chronic pain has a clear cause, such as a long-term illness, cancer, or arthritis. Illness can make your body more susceptible to pain, even after you recover. Injuries, including broken bones, sprains, or infections, can also leave you with chronic pain.
Pain that does not seem to be related to a physical illness or injury is psychogenic painIt is believed that anxiety, stress and depression lead to low endorphin levels in the blood.
Regardless of the specific cause, pain is a function of the nervous system. Nerves around an injury site sense the damage and send signals to the spinal cord and brain. The brain registers the pain and the nervous system responds. Muscles tense, emotions run high, and the nervous system becomes hypervigilant.
This high alert state is beneficial in acute pain. It tells the body that something is wrong, allowing us to protect ourselves from further injury. Once the damage or disease heals, the nervous system functions normally.
Symptoms of chronic pain syndrome
When the nervous system remains in a persistent state of high alert, it often becomes hypersensitive. It can continue the pain even after the original damage has healed. People with chronic pain describe it in different ways:
To beat
Stiffness
To shoot
Painful
Burning
pinch
Stinging
Poor sleep, mood swings, irritability and fatigue often accompany pain, which increases stress levels and nervous system reactivity. As pain increases, a new vicious circle begins.
7 Common Treatment Methods for Chronic Pain
Chronic pain can limit your quality of life and lead to significant long-term health problems. It can make managing daily tasks, maintaining relationships, and maintaining financial stability challenging. Chronic pain is uniquely personal, and finding an effective treatment becomes a priority.
Your biology and personal history can influence which pain therapies provide relief. However, the treatment combination for one person may not work for another.
1. Physiotherapy
Physical therapy is a highly personalized treatment regimen. Goals may include increased mobility and reduced pain to help you regain full function. Physical therapy includes passive and active treatments. Your program may begin with passive treatments and progress to active methods. Physical therapists play an important role in pain management through various therapies and daily living techniques. Various forms of exercise, including strength, flexibility, balance, endurance, power, and agility, are used to promote and restore normal function, as well as for pain management. While opioids only mask the sensation of pain, physical therapists can also treat pain through hands-on care. Techniques include manipulation, joint and soft tissue mobilization, dry needling, and cupping. This helps to address the pain and target the root of the problem.
2. Contrast therapy
Physiotherapists often alternate between cold and hot therapies. Cold therapy constricts blood vessels. Inflammation decreases when muscles contract and pain signals are reduced. Heat therapy increases circulation by dilating blood vessels. Flooding areas with nutrients and oxygen reduces muscle pain and allows the body’s cells to shed waste. Contrast therapy can reduce inflammation and increase circulation, which loosens tight, sore muscles.
3. Deep tissue massage
Muscle spasms and chronic muscle tension can build up from the stress of a typical daily routine. Cramps can also occur from sprains and strains. The direct pressure and friction applied during massage can release tension in the muscles, ligaments and tendons.
A TENS unit uses varying intensities of electrical current to stimulate muscles, which helps to reduce the occurrence and severity of muscle spasms. It can also increase the production of endorphins, the body’s natural painkillers. You can use just the unit that’s in your physical therapist’s office, or you can have a smaller unit made for home use.
5. Ultrasound
This deep heating technique is applied to your skin. As the heat waves penetrate your tissues, it is believed to improve blood flow and circulation. An ultrasound helps to reduce cramps, swelling, spasms, pain and stiffness.
6. Drug therapy
Over-the-counter medications may be enough to relieve mild pain caused by stiffness, inflammation, and muscle soreness. Typical drug therapy includes ibuprofen, aspirin, naproxen, and acetaminophen (Tylenol). Topical pain relievers that come in sprays, creams, and lotions may also provide temporary relief. Stronger medications for debilitating pain range from prescription NSAIDs, muscle relaxants, and anti-anxiety medications to opioids and steroid injections.
7. Exercise
Exercise is an active treatment and an essential part of the PT toolkit for improving mobility and strength. The brain stops sending constant alerts to the nervous system as the pain subsides. You and your physical therapist will work together to develop an exercise regimen to relieve pain. Examples of low-impact exercises include:
Swimming
Stretching and strengthening exercises
Cycling
To walk
Tai Chi
Pilates
Yoga
Exercise makes you stronger and trains your nervous system to trust that exercise is safe, allowing it to go from high alert to normal functioning.
If you have pain that comes and goes, physical therapy can help you understand the cause and how to treat it. Everyone responds differently to physical therapy. Contact Us Make an appointment today and learn more about the best treatment options.
Performing Exercises After an ACL Injury or Surgery: A Comprehensive Guide
Anterior cruciate ligament (ACL) injuries are among the most common and potentially devastating knee injuries, particularly in athletes and active individuals. Whether caused by a sudden twist, an awkward landing, or a direct impact, an ACL injury can sideline you for months. However, with the right approach to rehabilitation and a well-structured exercise plan, you can regain strength, mobility, and confidence in your knee. This comprehensive guide offers in-depth information, tips, and advice for performing exercises after an ACL injury or surgery.
Understanding ACL Injuries and Surgery
What is the ACL?
The anterior cruciate ligament (ACL) is one of four major ligaments in the knee joint. It runs diagonally through the center of the knee, connecting the femur (thigh bone) to the tibia (shin bone). The ACL plays a crucial role in stabilizing the knee during dynamic movements such as:
Cutting or changing direction quickly
Pivoting
Jumping and landing
Decelerating rapidly
The ACL prevents the tibia from sliding forward in relation to the femur and provides rotational stability to the knee. This stability is essential for activities that involve quick changes in direction, such as soccer, basketball, skiing, and football.
Mechanisms of ACL Injury
ACL injuries typically occur through one of the following mechanisms:
Non-contact injuries: These account for about 70% of ACL injuries. They often occur when an athlete changes direction rapidly, stops suddenly, or lands from a jump incorrectly.
Contact injuries: These occur when there’s a direct blow to the knee, often from the side, which can happen in contact sports like football or rugby.
Hyperextension: When the knee is forced beyond its normal range of motion, it can cause the ACL to tear.
Types of ACL Injuries
ACL injuries are typically classified into three grades:
Grade 1: A mild sprain where the ligament is stretched but not torn.
Grade 2: A partial tear of the ACL (relatively rare).
Grade 3: A complete tear of the ACL, often referred to as a “rupture.”
ACL Surgery Options
For many active individuals and athletes, especially those with complete ACL tears, surgery is often recommended. The most common surgical treatment is ACL reconstruction, where the damaged ligament is replaced with a graft. There are two main types of grafts:
Autograft: Tissue taken from the patient’s own body. Common autograft sources include:
Patellar tendon
Hamstring tendon
Quadriceps tendon
Allograft: Tissue taken from a donor, usually a cadaver.
Each graft type has its pros and cons:
Graft Type
Advantages
Disadvantages
Patellar Tendon Autograft
Strong initial fixation, faster healing to bone
Potential for anterior knee pain, risk of patellar fracture
Hamstring Tendon Autograft
Less harvest site morbidity, smaller incisions
Slower healing to bone, potential for hamstring weakness
Quadriceps Tendon Autograft
Good size and strength, less harvest site morbidity than patellar tendon
Less commonly used, potential for quadriceps weakness
Allograft
No harvest site morbidity, shorter surgery time
Slower incorporation, slightly higher failure rate in young, active patients
The choice of graft depends on various factors, including the surgeon’s preference, the patient’s age, activity level, and specific anatomical considerations.
ACL Injury Statistics
To understand the scope of ACL injuries, consider these statistics:
Statistic
Value
Annual ACL injuries in the US
~200,000
Percentage of ACL injuries requiring surgery
50-60%
Average recovery time to return to sports
6-9 months
Risk of re-injury within 2 years
15-25%
Percentage of female athletes compared to male athletes suffering ACL injuries
2-8 times higher
Percentage of ACL injuries that occur in non-contact situations
~70%
These statistics highlight the importance of proper rehabilitation and the need for a comprehensive approach to recovery and prevention.
The Importance of Rehabilitation
Rehabilitation following an ACL injury or surgery is crucial for several reasons:
1. Restoring Strength and Stability
ACL injuries and subsequent surgery can lead to significant muscle weakness, particularly in the quadriceps and hamstrings. A structured exercise program helps rebuild strength in these key muscle groups, which is essential for knee stability. Strong muscles around the knee joint can help:
Absorb shock and reduce stress on the knee
Improve joint alignment
Enhance overall leg strength and power
2. Regaining Range of Motion
After surgery, scar tissue formation and swelling can limit knee mobility. Flexibility exercises ensure that the knee can move through its full range of motion without pain or stiffness. This is crucial for:
Normal walking gait
Climbing stairs
Performing sports-specific movements
3. Reducing Swelling and Pain
Early movement and specific exercises can help reduce post-surgical swelling and manage pain by:
Promoting circulation and lymphatic drainage
Preventing adhesions
Stimulating the release of endorphins, the body’s natural pain relievers
4. Improving Proprioception
Proprioception is the body’s ability to sense the position and movement of its parts. ACL injuries can disrupt this sense in the knee. Proprioceptive exercises enhance:
Balance and coordination
Neuromuscular control
Reaction time
These improvements are crucial for preventing future injuries and regaining confidence in the knee’s stability.
5. Psychological Recovery
Rehabilitation is not just about physical recovery. It plays a significant role in psychological healing by:
Building confidence in the injured knee
Providing a sense of progress and accomplishment
Preparing the athlete mentally for return to sport
6. Preventing Re-injury
A comprehensive rehabilitation program addresses factors that may have contributed to the initial injury, such as:
Muscle imbalances
Poor movement patterns
Inadequate core strength
By correcting these issues, the risk of re-injury can be significantly reduced.
Show Image
Detailed Guide to Performing Exercises After an ACL Injury or Surgery
Pre-Exercise Considerations
Before beginning any exercise program, it’s crucial to:
Consult with your surgeon and physical therapist: They will provide clearance and guidelines specific to your case.
Understand your restrictions: Know what movements or activities to avoid at each stage of recovery.
Set up a safe exercise environment: Ensure you have a non-slip surface and any necessary equipment (e.g., resistance bands, stability ball).
Warm up properly: Start with gentle movements to increase blood flow to the area.
Phase 1: Early Rehabilitation (Weeks 1-4)
The focus in this phase is on protecting the graft, reducing swelling, and gradually restoring range of motion.
Key Exercises:
Heel Slides:
Lie on your back with legs straight.
Slowly slide your heel towards your buttocks, bending your knee.
Hold for 5 seconds, then slowly straighten.
Perform 3 sets of 10 repetitions.
Quad Sets:
Sit with your leg straight and supported.
Tighten your thigh muscle, pressing the back of your knee down.
Hold for 5 seconds, then relax.
Perform 3 sets of 10 repetitions.
Ankle Pumps:
Lie on your back or sit with your leg elevated.
Point your toes away from you, then flex them back towards you.
Perform 3 sets of 20 repetitions.
Passive Knee Extension:
Sit with your leg supported, a small rolled towel under your heel.
Relax and allow gravity to straighten your knee.
Hold for 5 minutes, gradually increasing duration as tolerated.
Straight Leg Raises:
Lie on your back with your uninjured leg bent.
Tighten your thigh muscle and lift your straight leg about 6 inches.
Hold for 3 seconds, then slowly lower.
Perform 3 sets of 10 repetitions.
Phase 2: Intermediate Rehabilitation (Weeks 4-8)
This phase focuses on progressive strengthening and introducing weight-bearing exercises.
Key Exercises:
Mini Squats:
Stand with feet shoulder-width apart, holding onto a stable surface.
Slowly bend your knees to about 30 degrees.
Hold for 3 seconds, then slowly straighten.
Perform 3 sets of 10 repetitions.
Step-Ups:
Stand in front of a low step (4-6 inches high).
Step up with your surgical leg, bringing your other foot onto the step.
Step back down, leading with the non-surgical leg.
Perform 3 sets of 10 repetitions on each leg.
Hamstring Curls:
Lie on your stomach.
Slowly bend your knee, bringing your heel towards your buttocks.
Hold for 3 seconds, then slowly lower.
Perform 3 sets of 10 repetitions.
Stationary Cycling:
Start with no resistance, focusing on smooth motion.
Gradually increase duration and resistance as tolerated.
Aim for 10-20 minutes per session.
Calf Raises:
Stand holding onto a stable surface.
Rise up onto your toes, then slowly lower.
Perform 3 sets of 15 repetitions.
Phase 3: Advanced Rehabilitation (Weeks 8-12)
This phase introduces more dynamic exercises and focuses on improving balance and proprioception.
Key Exercises:
Lunges:
Stand with feet hip-width apart.
Take a large step forward, lowering your hips until both knees are bent at 90 degrees.
Push back to the starting position.
Perform 3 sets of 10 repetitions on each leg.
Single-Leg Balance:
Stand on your surgical leg.
Maintain balance for 30 seconds.
Progress to closing your eyes or standing on an unstable surface.
Perform 3 sets.
Leg Press:
Start with light weight and gradually increase.
Press the weight away until your knees are almost straight, then slowly return.
Perform 3 sets of 12 repetitions.
Lateral Step-Downs:
Stand on a 4-6 inch step with your surgical leg.
Slowly lower your other foot to touch the ground, then raise back up.
Perform 3 sets of 10 repetitions on each leg.
Swimming or Water Jogging:
Start with 15-20 minutes and gradually increase duration.
Focus on proper form and avoid breaststroke kick initially.
Phase 4: Return to Activity (Weeks 12 and Beyond)
This phase prepares you for a return to sports or high-level activities.
Key Exercises:
Plyometric Drills:
Box Jumps: Start with a low box and progress in height.
Lateral Hops: Hop side to side over a line or low obstacle.
Progress from double-leg to single-leg exercises.
Agility Drills:
Shuttle Runs: Start with straight-line runs and progress to change of direction.
Ladder Drills: Focus on quick, precise foot movements.
Sport-Specific Exercises:
Gradually introduce movements specific to your sport.
Start at low intensity and progress as tolerated.
Strength Training:
Continue with progressive resistance training for legs and core.
Include exercises like squats, deadlifts, and leg press.
Cardiovascular Conditioning:
Progress to running on various surfaces and inclines.
Include interval training to improve endurance.
Nutrition and Recovery
Proper nutrition plays a crucial role in recovery from ACL surgery and rehabilitation. A well-balanced diet can help reduce inflammation, support tissue repair, and provide the energy needed for rehabilitation exercises.
Key Nutritional Considerations:
Protein Intake:
Essential for muscle repair and rebuilding.
Aim for 1.6-2.0 grams of protein per kilogram of body weight daily.
Include sources like lean meats, fish, eggs, dairy, and plant-based proteins.
Anti-Inflammatory Foods:
Help reduce inflammation and support healing.
Include omega-3 rich foods like salmon, flaxseeds, and walnuts.
Consume a variety of colorful fruits and vegetables for antioxidants.
Complex Carbohydrates:
Provide energy for rehabilitation exercises.
Choose whole grains, fruits, and vegetables.
Hydration:
Crucial for overall health and recovery.
Aim for 8-10 glasses of water per day, more if exercising intensely.
Recommended Daily Nutrient Intake for ACL Recovery
Nutrient
Recommended Daily Intake
Key Sources
Protein
1.6-2.0 g/kg body weight
Lean meats, fish, eggs, dairy, legumes
Omega-3 Fatty Acids
1-2 g
Fatty fish, flaxseeds, chia seeds, walnuts
Vitamin C
75-90 mg
Citrus fruits, berries, bell peppers, broccoli
Vitamin D
600-800 IU
Sunlight exposure, fatty fish, fortified foods
Calcium
1000-1200 mg
Dairy products, leafy greens, fortified foods
Iron
8-18 mg
Red meat, spinach, lentils, fortified cereals
Supplements
While a balanced diet should be the primary source of nutrients, some supplements may be beneficial during ACL recovery:
Collagen: May support joint health and ligament healing.
Vitamin D and Calcium: Essential for bone health, especially if mobility is limited.
Omega-3 Supplements: Can help reduce inflammation if dietary intake is insufficient.
Protein Powder: Can help meet increased protein needs, especially for athletes.
Always consult with your healthcare provider before starting any new supplement regimen.
Pain Management and Rest
Managing pain and getting adequate rest are crucial components of ACL rehabilitation:
Pain Management Strategies:
RICE Method: Rest, Ice, Compression, and Elevation, particularly in the early stages of recovery.
Proper Form: Ensure correct technique during exercises to avoid unnecessary strain.
Gradual Progression: Increase intensity and duration of exercises slowly to prevent overexertion.
Pain Medication: Use as directed by your healthcare provider, typically for short-term relief.
Importance of Rest:
Sleep: Aim for 7-9 hours of quality sleep per night to support tissue repair.
Recovery Days: Include rest days in your exercise routine to prevent overtraining.
Listen to Your Body: If you experience increased pain or swelling, take a break and consult your physical therapist.
Psychological Support and Mental Health
Recovering from an ACL injury can be mentally challenging. It
Psychological Support and Mental Health
Recovering from an ACL injury can be mentally challenging. It’s not just a physical journey, but an emotional one as well. Understanding and addressing the psychological aspects of recovery is crucial for a successful return to activity.
Common Psychological Challenges:
Fear of Re-injury: Many patients develop a fear of returning to the activity that caused their injury. This fear can be paralyzing and hinder progress.
Loss of Identity: For athletes, being sidelined can lead to a loss of identity and purpose.
Depression and Anxiety: The long recovery process and uncertainty about the future can trigger symptoms of depression and anxiety.
Frustration with the Recovery Process: The lengthy rehabilitation can be frustrating, especially when progress seems slow.
Loss of Confidence: Doubts about physical capabilities can erode self-confidence.
Strategies for Mental Health Support:
Set Realistic Goals:
Break down your recovery into small, achievable goals.
Celebrate minor milestones to maintain motivation.
Visualization Techniques:
Mentally rehearse successful performance of exercises and sports movements.
Visualize yourself returning to your sport or activity successfully.
Mindfulness and Relaxation:
Practice mindfulness meditation to stay present and manage anxiety.
Use deep breathing exercises to reduce stress.
Seek Professional Support:
Consider working with a sports psychologist or counselor.
Join support groups for individuals recovering from similar injuries.
Stay Connected:
Maintain contact with teammates and coaches.
Engage in team activities in non-physical roles when possible.
Education:
Learn about your injury and the recovery process to feel more in control.
Understand that setbacks are a normal part of the recovery journey.
Focus on Overall Health:
Use this time to improve other aspects of your health and fitness.
Explore new hobbies or skills to maintain a sense of progress and accomplishment.
Returning to Sport or Activity
Returning to sport or high-level activity after an ACL injury is a critical phase that requires careful planning and execution. It’s important to remember that being cleared to return to sport doesn’t necessarily mean you’re ready for full competition.
Criteria for Return to Sport:
Full Range of Motion: The affected knee should have the same range of motion as the unaffected knee.
Adequate Strength: Typically, the strength of the affected leg should be at least 90% of the unaffected leg.
Neuromuscular Control: Demonstrated ability to perform sport-specific movements with proper form and control.
Psychological Readiness: Confidence in the knee and readiness to return to full activity.
Passing Functional Tests: Successfully completing a series of physical tests that mimic sport demands.
Functional Tests for Return to Sport:
Test
Description
Passing Criteria
Single Leg Hop Test
Hop for distance on each leg
Affected leg ≥ 90% of unaffected leg
Triple Hop Test
Three consecutive hops for distance
Affected leg ≥ 90% of unaffected leg
Crossover Hop Test
Three hops crossing over a line
Affected leg ≥ 90% of unaffected leg
6-meter Timed Hop
Hop on one leg for 6 meters
Affected leg ≤ 10% slower than unaffected leg
Y-Balance Test
Single-leg reach test in 3 directions
< 4 cm side-to-side difference
Gradual Return to Sport Protocol:
Phase 1: Controlled Practice
Participate in non-contact drills
Focus on sport-specific movements in a controlled environment
Phase 2: Team Practice
Introduce contact drills gradually
Participate in scrimmages with teammates
Phase 3: Simulated Competition
Full-speed practice sessions
Scrimmages against other teams
Phase 4: Limited Game Play
Return to competition with limited playing time
Gradually increase duration of play
Phase 5: Full Return
Unrestricted participation in competition
It’s crucial to progress through these phases under the guidance of your healthcare team and to listen to your body throughout the process.
Long-Term Considerations and Injury Prevention
After recovering from an ACL injury, it’s important to focus on long-term knee health and preventing future injuries.
Ongoing Maintenance:
Continue Strength Training: Maintain strength in the quadriceps, hamstrings, and core muscles.
Regular Flexibility Work: Keep up with stretching routines to maintain good range of motion.
Balance and Proprioception Exercises: Incorporate these into your regular workout routine.
Proper Warm-up: Always perform a thorough warm-up before physical activity.
Injury Prevention Strategies:
Proper Technique: Focus on correct landing and cutting techniques in your sport.
Neuromuscular Training: Participate in programs designed to improve movement patterns and reduce injury risk.
Cross-Training: Engage in a variety of activities to promote overall fitness and reduce overuse injuries.
Listen to Your Body: Pay attention to signs of fatigue or pain and adjust your activity accordingly.
Regular Check-ups: Schedule periodic assessments with a sports medicine professional to monitor your knee health.
Long-Term Outlook:
While an ACL injury can be a significant setback, many individuals return to their pre-injury level of activity or sport. However, it’s important to be aware of the long-term implications:
Increased Risk of Osteoarthritis: ACL injuries, even when properly treated, may increase the risk of developing osteoarthritis in the knee later in life.
Potential for Re-injury: There is a slightly elevated risk of re-injury or injuring the opposite knee’s ACL.
Ongoing Maintenance: Long-term success often requires ongoing attention to knee health and overall fitness.
Conclusion
Recovering from an ACL injury or surgery is a challenging but achievable journey. By following a structured rehabilitation program, paying attention to nutrition and mental health, and gradually progressing through the phases of recovery, you can optimize your chances of a successful return to activity.
Key takeaways:
Follow a structured rehabilitation program guided by healthcare professionals.
Progress gradually through the phases of recovery, from gentle movements to sport-specific exercises.
Pay attention to proper form and technique during exercises.
Support your recovery with proper nutrition and rest.
Address the psychological aspects of recovery and seek support when needed.
Use functional tests to gauge readiness for return to sport.
Focus on long-term knee health and injury prevention strategies.
Remember, every individual’s recovery is unique. Stay patient, stay committed, and celebrate the small victories along the way. With dedication and the right approach, you can overcome an ACL injury and return to an active, healthy lifestyle.
Factors that contribute to the relief of knee complaints
From January 2010 to August 2023, a total of 2,321 patients started b/tsDMARD treatment (Fig. 1). Of these, 573 had knee pain and/or swelling at the time of starting b/tsDMARDs (considered baseline). Six months later, 438 individuals returned for follow-up and swelling and/or tender joints were recorded. We excluded patients who had undergone total knee arthroplasty on the symptomatic side (N = 18) and those who had undergone TKA during the follow-up period (N= 7). As a result, 413 patients were included in the study (Supplementary Table S1). We then focused on patients who continued b/tsDMARDs for at least 3 months. Consequently, 295 cases were analyzed. The mean age at baseline was 60.9 years, ACPA positivity was 78.3%, RF positivity was 76.6%, females were 85.1%, and the mean RA duration was nine years (Table 1).
Figure 1
Table 1 Demographics and disease characteristics of patients with knee joint symptoms at baseline of b/tsDMARD treatment who continued the medication for 3 months and had knee joint symptoms at 6 months.
The symptom relief at 6 months in patients who continued b/tsDMARDs for 3 months was 78.2% for IL-6 inhibitors, 68.6% for JAK inhibitors, 65.9% for TNF inhibitors, and 57.6% for CTLA4-Ig (P< 0.01, Figure 2). The rates of knee joint symptom relief at 3 months were 66.3% for IL-6 inhibitors, 51.2% for JAK inhibitors, 61.4% for TNF inhibitors, and 55.6% for CTLA4-Ig, without statistical significance (P= 0.32, Supplementary Figure S1a). Significant differences were observed in the proportion of improvement in knee joint symptoms between 3 and 6 months for all b/tsDMARDs. Notably, further improvement in knee joint symptoms from 3 to 6 months was noted for both IL-6 and JAK inhibitors (Supplementary Figure S1b).
Figure 2
Percentages of relief of knee joint symptoms after 6 months of treatment, categorized by mode of action of each drug, in patients with knee joint symptoms at initiation of treatment with biologic/targeted synthetic disease-modifying anti-rheumatic drugs (b/tsDMARDs) who continued therapy for 3 months. IL-6, interleukin 6; JAK, Janus kinase; CTLA4-Ig, cytotoxic T-lymphocyte-associated antigen-4-Ig; TNF, tumor necrosis factor. ** P< 0.01 according to the Cochran-Armitage trend test.
Three months after initiation, the continuation rate was 76.5% for IL-6 inhibitors, 74.5% for JAK inhibitors, 63.1% for TNF inhibitors, and 85.5% for CTLA4-Ig (P< 0.01; Figure 3a).
figure 3
Continuation rates and disease activity for each drug.a) The percentage of patients with knee joint symptoms at baseline of b/tsDMARD treatment who continued therapy for 3 months. **; P< 0.01, by Chi-square test (B) Basic disease activity (C) Disease activity after 3 months of treatment.D) The difference in disease activity from baseline after 3 months of treatment.and) Disease activity after 6 months of treatment.F) The difference in disease activity from baseline after 6 months of treatment. *; P< 0.05, **; P< 0.01, ***; P< 0.001 by the Steel-Dwass test. DAS28-ESR, disease activity score 28-joint count with erythrocyte sedimentation rate; CDAI, clinical disease activity index; SDAI, simplified disease activity index
In patients who continued b/tsDMARDs after 3 months, disease activity (DAS28-ESR, disease activity score 28-joint count with erythrocyte sedimentation rate [DAS28-ESR]clinical disease activity index [CDAI]and simplified disease activity index [SDAI]) improved at 3 and 6 months compared to baseline (Fig. 3b–f). Although differences were observed in the values of DAS28-ESR, CDAI and SDAI at 3 and 6 months, as well as differences from baseline, between these drugs, IL-6 inhibitors were not inferior to the other drugs in any of these indicators.
When examining treatments associated with relief of knee joint symptoms in patients who continued b/tsDMARD therapy beyond 3 months, the use of IL-6 inhibitors emerged as a significant contributing factor, surpassing TNF inhibitors in resolution of knee joint symptoms (Fig. 4, odds ratio [OR] 2.1, 95% confidence interval [CI] 1.1–4.3, P= 0.03) or CTLA4-Ig (OR 3.0, 95% CI 1.4–6.5, P= 0.005). The OR for relief of knee joint symptoms with b/tsDMARDs as first-line treatment was 1.72 (95% CI 0.99–2.99, P= 0.05). Methotrexate (MTX) or glucocorticoid use did not appear to be a significant risk factor.
Figure 4
Multivariable logistic regression analysis of relief of knee joint symptoms after 6 months of treatment. MTX, methotrexate.
Factors contributing to the inhibition of the destruction of the knee joint
Next, we focused on 141 patients who continued b/tsDMARD therapy for 3 months and underwent knee joint radiography at baseline and 2 years later. At baseline, there were no significant differences in disease activity as measured by DAS28-ESR, SDAI, and CDAI (Supplementary Table S2). At 3 months, DAS28-ESR was higher in patients using JAK inhibitors and CTLA4-Ig, 4.0 and 4.1, respectively, compared with 3.0 in patients using IL-6 inhibitors. MTX use was lower in CTLA4-Ig users; however, this difference was not statistically significant. In addition, the rate of use of JAK inhibitors as first-line b/tsDMARDs was lower.
At baseline, there were no significant differences in Larsen grade between the different drugs (Fig. 5a). Over two years, excluding progression from grade 0 to grade I, worsening of Larsen grade was observed in 5.2% of patients treated with IL-6 inhibitors, 6.3% with JAK inhibitors, 19.4% with TNF inhibitors and 28% with CTLA4-Ig (Fig. 5b, P< 0.01).
Figure 5
Radiographic examination of the knee.a) X-ray of the knee at the start of treatment and after two years, assessed based on the Larsen grade.B) Percentage of patients with progression in Larsen grade on radiographs from baseline to two years, excluding progression from grade 0 to I. **; P< 0.01 according to the Cochran-Armitage trend test.C) Factors contributing to progression of Larsen grade on radiographs from baseline to two years, using multivariable logistic regression analysis.
In line with this, when considering the use of MTX, glucocorticoids, the use of b/tsDMARDs as first-line treatment and the mode of action as covariates, the use of IL-6 inhibitors emerged as a protective factor against knee joint deterioration compared with CTLA4-Ig (OR 0.14, 95% CI 0.02–0.78, P= 0.02, Figure 5c).