Inverted knees, also known as knee inversion, is a condition where the knees turn inward, affecting the alignment and movement of the lower extremities. Understanding the causes, effects, and management of inverted knees is crucial for individuals dealing with this condition. In this article, we will explore the anatomy of inverted knees, methods for diagnosis, treatment options, and preventive measures to help manage and improve the condition.
Key Takeaways
- Understanding the anatomy of inverted knees helps in identifying the structural issues that contribute to knee inversion.
- Diagnosing inverted knees involves physical examination and imaging techniques such as X-rays and MRI scans.
- Treatment options for inverted knees include physical therapy, orthotic devices, bracing, and surgical interventions, depending on the severity of the condition.
- Preventive measures and lifestyle modifications, such as specific exercises, proper footwear, and avoiding aggravating activities, can help in managing and preventing knee inversion.
- Consulting a healthcare professional is essential for accurate diagnosis and personalized treatment plans for inverted knees.
Understanding the Anatomy of Inverted Knees
The Structure of the Knee Joint
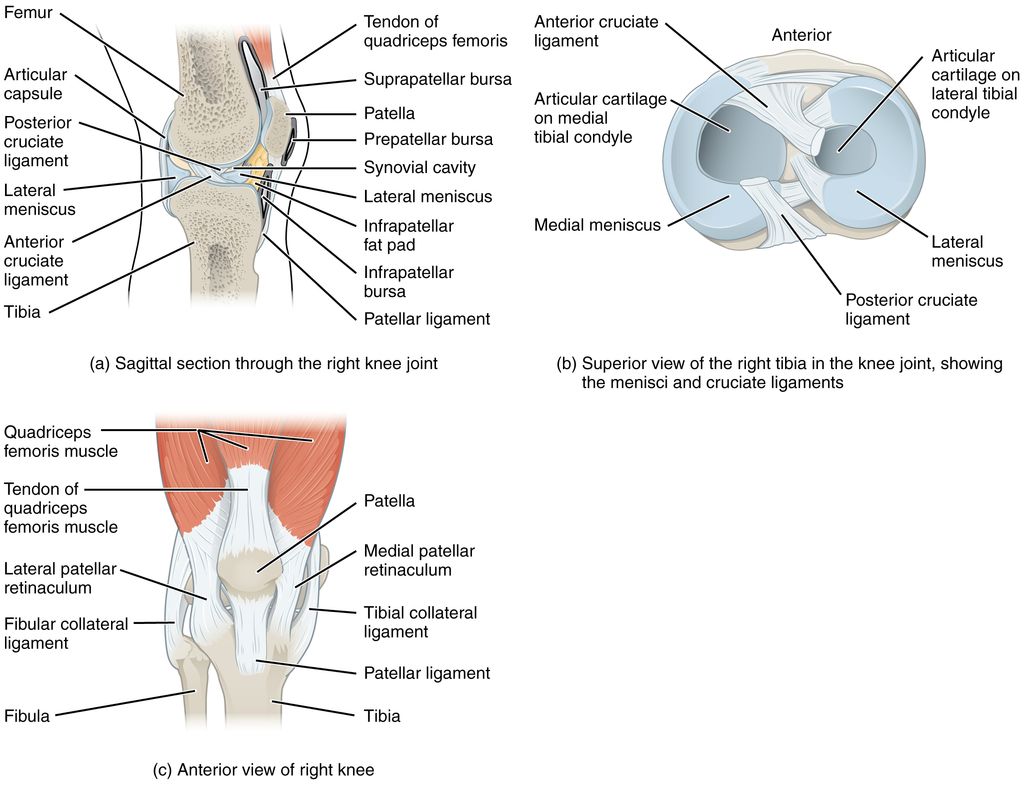
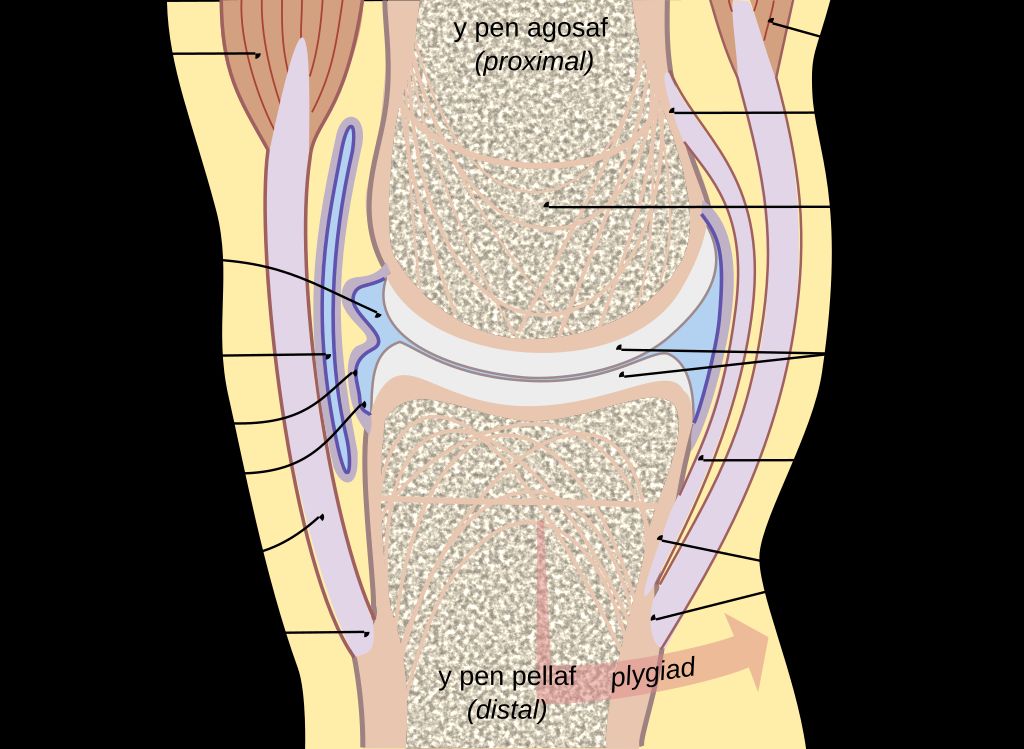
When we explore the anatomy of the knee joint, we delve into a complex structure pivotal for movement. The knee joint is primarily composed of three bones: the femur, tibia, and patella. These bones are connected by ligaments that provide stability and tendons that attach muscles to the bones, allowing for movement.
The knee joint’s stability is largely due to four key ligaments: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). Each plays a vital role in maintaining knee alignment and preventing excessive movement that could lead to injury.
Cartilage within the knee, including the menisci and articular cartilage, acts as a cushion and allows for smooth motion. However, when the knee is inverted, or the tibia is abnormally rotated inward, the stress distribution across these structures changes, which can lead to discomfort or injury over time.
Tip: Regularly engaging in exercises that strengthen the muscles around the knee can help maintain proper alignment and prevent the development of inverted knees.
Understanding the intricate workings of the knee joint is essential for recognizing the implications of knee inversion and the importance of seeking appropriate treatment to manage this condition.
Causes of Knee Inversion
In understanding the causes of knee inversion, it is essential to consider the structural aspects of the knee joint. The alignment of the bones, ligaments, and tendons plays a crucial role in maintaining stability and preventing excessive inward rotation of the knee. Misalignment of these structures can lead to increased stress on the joint and contribute to the development of inverted knees. Additionally, factors such as muscle weakness and imbalances can further exacerbate the risk of knee inversion. Understanding these structural and biomechanical aspects is fundamental in addressing and managing inverted knees effectively.
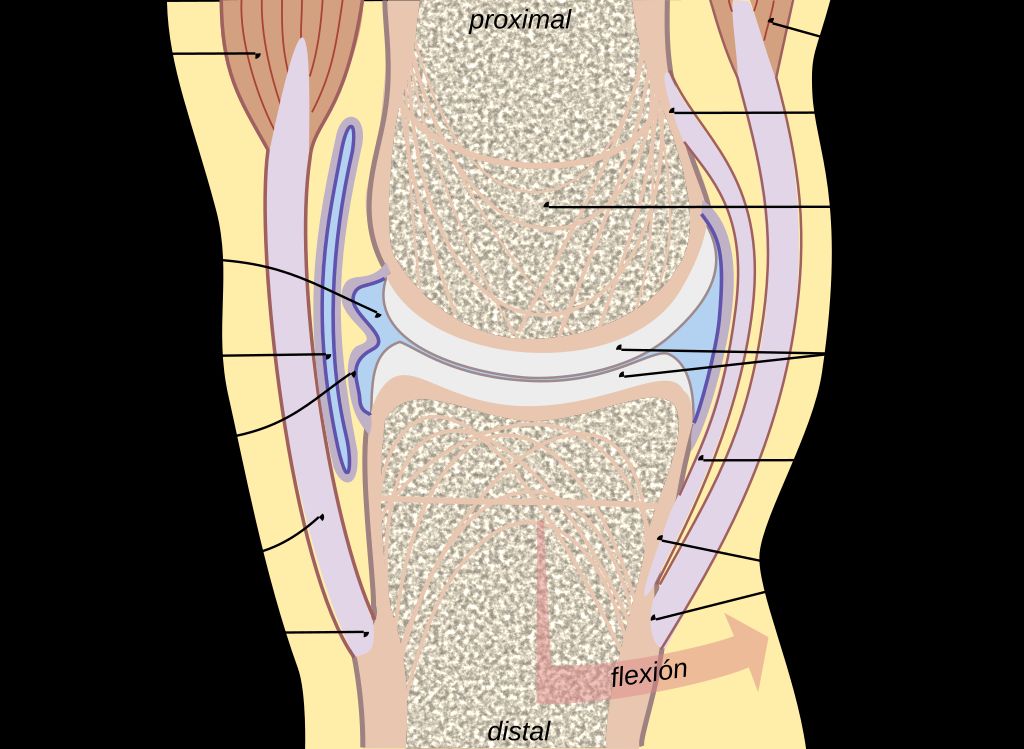
Effects of Inverted Knees on Movement
The structure of the knee joint is crucial in understanding the complexities of knee inversion. It involves the interaction of bones, ligaments, and tendons, with the patella playing a significant role in stabilizing the joint. Additionally, the alignment of the femur and tibia is a key factor in determining the degree of knee inversion. Understanding these structural components is essential for effective management of inverted knees.
Furthermore, the causes of knee inversion can vary, including genetic predisposition, muscle imbalances, and improper biomechanics. These factors contribute to the misalignment of the knee joint, leading to increased stress on specific structures. Identifying the underlying cause is crucial for developing targeted treatment strategies.
The effects of inverted knees on movement can be profound, impacting activities such as walking, running, and even standing. Individuals with inverted knees may experience instability and reduced range of motion, affecting their overall mobility and quality of life. It is important to address these movement limitations through targeted interventions and lifestyle modifications.
Diagnosing Inverted Knees

Physical Examination
Upon conducting a thorough physical examination, we carefully assess the alignment, range of motion, and stability of the knee joint. We pay close attention to any signs of discomfort, swelling, or abnormal movement patterns. Additionally, we may perform specialized tests to evaluate the strength and function of the muscles surrounding the knee. These assessments provide valuable insights into the extent of knee inversion and guide further diagnostic decisions. In some cases, imaging techniques, such as X-rays or MRI scans, are employed to visualize the internal structures of the knee and confirm the diagnosis.
Imaging Techniques for Diagnosis
When we suspect inverted knees, we often turn to imaging techniques to confirm the diagnosis. These methods provide us with a detailed view of the knee’s structure, allowing us to assess the extent of inversion and any associated conditions. The most common imaging techniques include X-rays, MRI (Magnetic Resonance Imaging), and CT (Computed Tomography) scans.
- X-rays are typically the first step, offering a clear image of bone alignment and joint space.
- MRI scans provide a more detailed image, showing soft tissues such as ligaments and cartilage.
- CT scans combine X-rays from different angles to create cross-sectional images of the knee, which can be particularly useful in complex cases.
Tip: It’s essential to choose the most appropriate imaging technique based on the individual’s symptoms and physical examination findings to ensure an accurate diagnosis.
Treatment Options for Inverted Knees

Physical Therapy and Rehabilitation
In our approach to managing inverted knees, we emphasize the role of physical therapy and rehabilitation. This non-invasive treatment plan is tailored to each individual’s needs, focusing on strengthening the muscles around the knee to improve stability and correct alignment.
Physical therapists often recommend a series of exercises that target the quadriceps, hamstrings, and calf muscles. These exercises not only help in realigning the knee joint but also contribute to overall leg strength and balance. It’s crucial to follow the prescribed regimen diligently for the best outcomes.
Consistency in performing therapeutic exercises is key to managing knee inversion effectively.
We also incorporate proprioceptive training into the rehabilitation program. This involves exercises that enhance the body’s awareness of joint position, which is vital for maintaining knee stability during movement. Below is a list of common exercises included in a typical rehabilitation program:
- Straight leg raises
- Hamstring curls
- Calf stretches
- Step-ups
- Balance exercises, such as single-leg stands
Orthotic Devices and Bracing
Orthotic devices and bracing play a crucial role in providing support and stability for individuals with inverted knees. Custom orthotic devices are designed to address specific alignment issues and provide comfort during daily activities. Bracing, on the other hand, offers external support to the knee joint, reducing the risk of injury during physical movements. It’s important to consult with a healthcare professional to determine the most suitable orthotic device or brace based on individual needs and lifestyle. Additionally, proper fitting and regular maintenance of these devices are essential for long-term effectiveness and comfort.
Surgical Interventions
In cases where physical therapy and orthotic devices are insufficient to correct inverted knees, we may consider surgical interventions. These procedures are typically reserved for severe deformities or when the condition leads to persistent pain and functional impairment. Surgical options vary depending on the underlying cause and severity of the knee inversion.
The most common surgeries include realignment osteotomies, where the bone is cut and repositioned, and ligament reconstructions to stabilize the knee joint. It’s essential to understand that surgery is followed by a period of rehabilitation to ensure the best possible outcome.
- Post-operative care is critical and includes: *
- Pain management
- Physical therapy
- Gradual return to activities
Remember, the goal of surgery is not only to correct the anatomical issue but also to restore function and alleviate discomfort. It’s a decision that should be made with careful consideration of all potential risks and benefits.
Preventive Measures and Lifestyle Modifications
Exercises to Improve Knee Alignment
We understand that managing inverted knees involves a proactive approach to improving knee alignment. One of the most effective strategies is engaging in a series of targeted exercises. These exercises are designed to strengthen the muscles around the knee, enhance joint stability, and promote proper alignment.
- Quadriceps strengthening: Essential for supporting the front of the knee joint.
- Hamstring curls: Improve the strength of the muscles at the back of the thigh.
- Calf raises: Enhance the stability of the lower leg and support knee alignment.
- Hip abductor and adductor exercises: Balance the muscles on the inner and outer thigh to assist in knee positioning.
Consistency in performing these exercises is key to seeing improvements. It is advisable to start with lower intensity and gradually increase as your muscles adapt.
It’s also important to incorporate exercises that focus on balance and proprioception, such as single-leg stands, to further support knee alignment. We recommend consulting with a physical therapist to tailor an exercise program that is specific to your needs and condition.
Footwear and Foot Support
When it comes to managing inverted knees, footwear and foot support play a crucial role in maintaining proper alignment and reducing stress on the knee joint. Our choice of footwear can either support or exacerbate knee inversion, so it’s important to select shoes that provide adequate arch support and stability. Additionally, using orthotic inserts can further enhance the alignment of the feet and ankles, which in turn positively impacts knee positioning. It’s advisable to consult with a podiatrist or orthopedic specialist to determine the most suitable footwear and support options for individual needs.
Tip: When choosing footwear, prioritize comfort and support over style. Look for shoes with good arch support and cushioning to help maintain proper alignment and reduce the risk of knee inversion.
Avoiding Activities that Aggravate Knee Inversion
It is crucial to be mindful of our movements and activities to prevent exacerbating knee inversion. Engaging in high-impact sports or activities that involve sudden changes in direction can put unnecessary strain on the knees. Additionally, wearing improper footwear with inadequate support can further contribute to knee misalignment. Choosing supportive footwear and being mindful of the impact of certain activities on knee alignment is essential for managing knee inversion effectively.
Conclusion
In conclusion, understanding the complexities of inverted knees is crucial for effective management and treatment. By addressing the underlying causes and implementing targeted interventions, individuals with inverted knees can experience improved mobility and reduced discomfort. Further research and clinical studies are needed to enhance our understanding of this condition and develop more tailored approaches for management. Empowering individuals with knowledge about their condition is essential for promoting proactive self-care and optimizing long-term outcomes.
Frequently Asked Questions
What are the common symptoms of inverted knees?
Common symptoms of inverted knees include knee pain, instability, and difficulty with activities that involve weight-bearing on the knees.
Can inverted knees be corrected without surgery?
In some cases, physical therapy, orthotic devices, and lifestyle modifications can help improve knee alignment and manage the symptoms of inverted knees without the need for surgery.
Are there specific exercises that can help improve knee alignment?
Yes, exercises such as leg strengthening, stretching, and balance training can help improve knee alignment and stability.
How can footwear and foot support affect knee inversion?
Proper footwear and foot support can help distribute weight evenly and provide stability, which can reduce the risk of knee inversion and improve overall knee alignment.
What activities should be avoided to prevent aggravating knee inversion?
Activities that involve excessive twisting, pivoting, or sudden changes in direction should be avoided to prevent aggravating knee inversion.
What are the potential long-term effects of untreated inverted knees?
Untreated inverted knees may lead to chronic knee pain, increased risk of knee injuries, and altered gait patterns, which can impact overall mobility and quality of life.