Prevalence and normalization of stress urinary incontinence in female strength athletes.
Mahoney K, Heidel RE, and Olewinski LJ Good luck Cond2023 [epub ahead of print].
Full text freely available
Take home message
Seven in ten female strength training athletes report stress urinary incontinence (SUI) in some aspect of their lives. However, fewer than 2 in 10 athletes talk to their doctor or seek treatment for SUI.
Background
Very intensive physical activity can increase the risk of SUI, an involuntary loss of urine due to increased intra-abdominal pressure. Up to 2 in 5 women may experience SUI throughout their lives, which can negatively impact an individual’s quality of life. Pelvic floor training can treat SUI. Although female strength training athletes may be at greater risk for SUI, it remains unclear how many of these athletes experience SUI and seek treatment, as well as how they would prefer to learn about SUI.
Study aim
The researchers conducted a cross-sectional study to assess female strength training athletes’ understanding and normalization of SUI, including how often female strength training athletes sought treatment for SUI.
Methods
The researchers developed a new study, which was expertly reviewed, to share on various social media platforms. The survey asked respondents about demographic information, risk factors for SUI, experience with SUI, favorite sources of information about SUI, and whether the respondent had sought treatment for SUI. Respondents to the survey were women over the age of 18 who considered powerlifting, weightlifting or strongman as their main activity.
Results
Of the 425 respondents, 69% reported experiencing SUI in some aspects of their lives. Of the athletes who experienced SUI, 61% reported that they first experienced SUI after starting their sport. About two-thirds of athletes thought SUI was a normal part of their sport. Only 17% of respondents reported talking to their doctor about SUI, and 9% sought treatment. Nearly 30% of respondents reported seeking advice about SUI from videos and articles on the internet, 23% spoke to friends and 13% spoke to their coach about SUI.
Viewpoints
Overall, the results of this study indicated that SUI is common among female strength training athletes, and most consider it a normal part of their sport. However, very few athletes turn to healthcare to address their SUI. It would be interesting to see this study replicated by asking athletes to complete the survey during competitions, as it is unclear whether women with SUI are more likely to complete the online survey. So the online survey may overestimate how many women have SUI, but the answers about engaging the health care system and where they seek advice are still likely to be informative.
Clinical implications
Clinicians who work with athletes who are at high risk for developing SUI should educate athletes about effective treatments. It can also be helpful to educate strength and conditioning coaches about SUI and available treatments.
Questions for discussion
How do you talk to your athletes about SUI? Have you noticed that other athletes have high SUI rates?
Written by Kyle Harris Reviewed by Jeffrey Driban
related posts
Check the lights before you check that urine! Throw away your strips for better urine density results Altered hydration status may impact concussion assessment Cheers! The more you exercise, the more you should drink
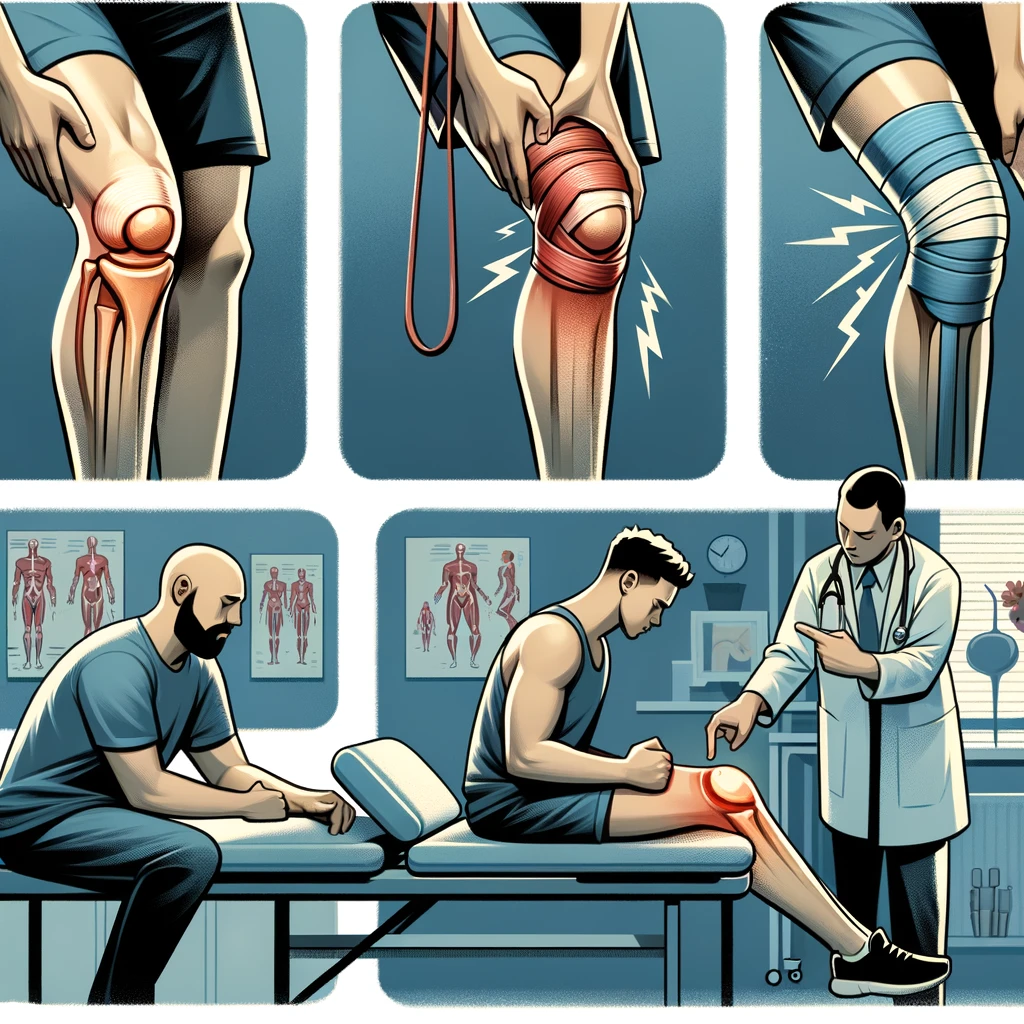
Prevention Strategies for Knee Ligament Injuries: Professional Tips
Knee ligament injuries are common among athletes and can be a frustrating setback for anyone who enjoys an active lifestyle. The knee joint is one of the largest and most complex joints in the body, making it vulnerable to various types of injuries. Understanding and identifying knee ligament injuries is crucial to prevent further damage and promote quick recovery.
The most common knee ligament injuries are the anterior cruciate ligament (ACL), medial collateral ligament (MCL), posterior cruciate ligament (PCL), and lateral collateral ligament (LCL). These injuries can occur due to direct trauma, such as contusions and strains, or from indirect trauma, such as sudden changes in direction. Symptoms of knee ligament injuries include pain, swelling, inflammation, and joint laxity. In this article, we will discuss five prevention strategies for knee ligament injuries to help maintain knee stability and prevent knee instability.
professional tips for prevention strategies to help avoid knee ligament injuries:
Category
Tips
Strength & Flexibility Training
– Emphasize hamstring, glute, quad, hip & core exercises<br>- Ensure muscle imbalances are addressed<br>- Use proper form/technique to prevent overstress
Movement Control & Balance
– Practice proper landing mechanics when jumping <br>- Enhance proprioception & body control<br>- Integrate deceleration drills
Equipment & Environment
– Wear supportive & appropriate footwear <br>- Tape or brace vulnerable knees if needed <br>- Ensure safe, even playing surfaces
Loading & Recovery
– Follow loading guidelines for ramping up intensity<br>- Avoid aggressive pivoting until tissues adapted<br>- Schedule adequate rest periods between sessions
Body Composition & Nutrition
– Prevent muscle loss during injury layoffs<br>- Maintain healthy BMI year-round<br>- Support exercise recovery nutritionally
Mindset & Motivation
– Foster positive, confident mentality<br>- Set smaller achievable goal steps <br>- Enlist social support structure
The most effective ACL/knee ligament injury prevention programs take a comprehensive approach. Optimizing strength, movement mechanics, loading, and nutrition helps create resilience. Confidence in knee stability paired with caution towards unsafe mechanics allows for safer progression. Expert guidance tailoring programs is key for best injury deterrence.
Key Takeaways
Understanding the anatomy of the knee joint and identifying knee ligament injuries can promote quick recovery.
Direct and indirect trauma can cause knee ligament injuries, leading to pain, swelling, inflammation, and joint laxity.
Understanding and Identifying Knee Ligament Injuries
Knee ligament injuries are common among athletes and individuals who engage in physical activities that require jumping, pivoting, or sudden changes in direction. In this section, we will discuss the common types and causes of knee ligament injuries, how to identify symptoms and diagnose the injury, treatment and rehabilitation options, and the role of sex and age in knee ligament injuries.
Common Types and Causes
The most common types of knee ligament injuries are the anterior cruciate ligament (ACL) and medial collateral ligament (MCL) injuries. The ACL is usually injured during non-contact activities such as landing after a jump or sudden stops and changes in direction. On the other hand, the MCL is usually injured from a direct blow to the outer side of the knee, such as when playing football or hockey.
Symptoms and Diagnosis
The symptoms of knee ligament injuries include pain, swelling, bruising, and instability. The diagnosis of knee ligament injuries is usually made through a physical exam and imaging tests such as MRI or X-rays. It is important to seek medical attention if you experience any of these symptoms.
Treatment and Rehabilitation
The treatment and rehabilitation of knee ligament injuries depend on the severity of the injury. Treatment options include rest, ice, compression, and elevation (RICE), physical therapy, and surgery. Rehabilitation includes exercises to improve range of motion, strength, and mobility. It is important to follow the guidance of a physical therapist or orthopedic surgeon to ensure proper recovery.
Role of Sex and Age
Research shows that females are more prone to knee ligament injuries than males due to differences in anatomy, form, and hormones such as estrogen and relaxin. Additionally, age plays a role in knee ligament injuries, with individuals over 50 years old being at a higher risk due to decreased muscle strength and flexibility.
Sports and Injuries
Knee ligament injuries are common in sports that require sudden stops and changes in direction such as soccer, basketball, and football (soccer). Injury prevention programs that include warm-up, neuromuscular training, and proprioception exercises can reduce the frequency of knee ligament injuries by up to 50%. Coaches and athletes should also prioritize proper technique, posture, and fatigue management to prevent knee ligament injuries.
In conclusion, knee ligament injuries are common among athletes and individuals who engage in physical activities. Understanding the common types and causes of knee ligament injuries, identifying symptoms and diagnosing the injury, and following proper treatment and rehabilitation options can help prevent long-term damage. Coaches, athletes, and individuals should prioritize injury prevention programs and proper technique to reduce the frequency of knee ligament injuries.
Prevention Strategies for Knee Ligament Injuries
When it comes to knee ligament injuries, prevention is key. Here are some effective strategies that we recommend:
Strengthening and Conditioning
Strengthening and conditioning exercises can help improve muscle strength and endurance, which can help reduce the risk of knee ligament injuries. Exercises that target the hips, ankles, and core can be particularly effective in improving stability and reducing the risk of injury.
Injury Prevention Programs
Injury prevention programs can be an effective way to reduce the risk of knee ligament injuries. These programs typically include a combination of warm-up exercises, neuromuscular training, and strength and conditioning exercises. They can be particularly effective for athletes who participate in high-risk sports, such as soccer, basketball, and football.
Importance of Compliance and Frequency
Injury prevention strategies are only effective if they are followed consistently and frequently. Compliance with injury prevention programs is essential for reducing the risk of knee ligament injuries. It is important to follow the program as prescribed and to make sure that exercises are performed correctly and with good form.
In conclusion, preventing knee ligament injuries requires a combination of strategies that target strength, stability, and flexibility. Injury prevention programs that incorporate warm-up exercises, neuromuscular training, and strength and conditioning exercises can be particularly effective. However, compliance with these programs is essential for success. By following these strategies, we can help reduce the risk of knee ligament injuries and keep athletes healthy and active.
Most high school athletic administrators reported having a written heat illness policy in place, but they were often missing key components. The presence of an athletic trainer helped create a written policy that included more components.
Background
Sports administrators play an important role in policy acceptance. Policy measures such as addressing acute heat illness are critical as improper management can lead to poor outcomes. Unfortunately, we know little about the factors that promote and hinder the implementation of heat illness policies.
Study aim
The authors surveyed high school athletic administrators in the United States to describe the adoption of exertional heat illness policies and to examine factors that influence the adoption of these policies.
Methods
During the 2018-2019 academic school year, the research team emailed nearly 7,000 athletic administrators inviting them to complete a questionnaire asking about 1) demographics, 2) exercise-related illness policies, 3) monitoring and modification of written policy, and 4) enablers and barriers to policy development. The researchers used the precautionary adoption process model to assess an athletics administrator’s willingness to adopt policies. The adoption model is based on 8 phases, from not being aware to maintaining a written policy for more than 6 months.
Results
Of 466 athletics administrators (~48 years old, 82% male, 77% worked in the field for more than 15 years), 78% reported having a written policy on the prevention and treatment of exertional heat illness. Only 6% adopted all eleven essential elements of an exertional heat illness policy. Almost half of the managers indicated that they adopted fewer than 5 essential elements.
Older athletics administrators, those who had previously dealt with heat illness, or those with an athletic trainer on their staff were more likely to have a written policy. Additionally, state mandates and having a medical professional were the most commonly cited facilitators for adopting policies on exertional illness prevention and use of a rectal thermometer. Similarly, the most commonly reported barrier to comprehensive heat illness management was the lack of a full-time athletic trainer (11). Administrators also recognized budget constraints that limited the use of a cold water immersion pool (23%), and the top barriers to using a rectal thermometer were discomfort using the thermometer (32%), parent/guardian resistance (30 %), resistance from parents/guardians (30%). coaches (30%) and liability issues (27%).
Viewpoints
Nearly 80% of athletics administrators surveyed reported that they had a written policy on exertional heat illness. Few integrated or were aware of all the necessary components to meet best clinical practices. The authors found that access to athletic training services was associated with better adoption of exercise health policies. This finding is consistent with it being an athletic trainer who would implement such a policy. It’s worth recognizing that only 7% of administrators contacted completed the survey. Therefore, these results may not accurately reflect what is happening in high schools across the country. One possibility is that people more interested in policy or heat illness completed the survey. So these results may show us the best-case scenario for written policies (78%) that include all components (6%) – which is a worrying sign.
Clinical implications
Encouraging state mandates and schools to hire athletic trainers can ensure that there are written policies to address heat illness. Clinicians may also want to consider strategies to educate coaches and parents/guardians about the reasons for this policy, such as rectal thermometers and cold water plunge pools.
Questions for discussion
Are you having trouble adding rectal temperature to your exercise heat illness protocol? Do you communicate with your athletics administrator regarding the approval, implementation and annual review/practice of your emergency policy?
related posts
Management of exertional heat stroke still leaves something to be desired
A little more education about heat stroke due to exertion could go a long way
Clinical Pearl: prevention and treatment of exertional heat stroke
Tag us! What do coaches know about heat stroke during exertion and the role of the athletic trainer?
Follow guidelines to prevent exertional heat illness? Let’s reconsider these guidelines
Written by Jane McDevitt Reviewed by Jeffrey Driban
Anterior cruciate ligament (ACL) reconstruction is a common surgical procedure for individuals who have suffered a torn ACL. While outcomes have improved dramatically, knee pain and re-injury continue to be concerns during the recovery process. Recent advances in rehabilitation protocols and biomechanical research are shedding light on optimal recovery strategies.
Knee pain following ACL reconstruction arises due to multiple interrelated biomechanical and physiological factors. The initial trauma of surgery triggers an inflammatory response which can lead to fluid buildup, swelling, and stiffness, resulting in pain with movement. This acute inflammatory phase usually lasts 6-8 weeks. Concurrently, muscular imbalances around the knee joint develop, most notably quadriceps inhibition and weakness. The quadriceps muscles play a crucial role in stabilizing the knee joint. When weakened and inhibited after surgery, abnormal forces are transmitted through the joint, exacerbating pain and dysfunction. Finally, biomechanical alterations including asymmetric gait patterns and improper landing mechanics cause further pain. A careful evaluation of all these contributing trigger points through a full physical therapy examination is key to pinpointing the optimal treatment approach.
Causes of Knee Pain
Knee pain following ACL reconstruction arises due to multiple interrelated biomechanical and physiological factors. The initial trauma of surgery triggers an inflammatory response which can lead to fluid buildup, swelling, and stiffness, resulting in pain with movement.
Inflammation
This acute inflammatory phase usually lasts 6-8 weeks.
A 2022 study found that altered walking biomechanics were present even 2 years after surgery, especially in females (Smith et al). These persistent abnormalities highlight the need for rehabilitation focused on normalizing movement patterns.
Effective knee pain management requires a multifaceted rehabilitation program tailored to the individual’s specific deficits and dysfunctions. The priority initially is controlling inflammation through ice, compression, medication, and activity modification. Once pain and swelling have been reined in, restoring full knee mobility is essential for reducing stiffness and dysfunction. Gentle manual therapy techniques and range of motion exercises facilitate this process. As mobility improves, muscular imbalances must be addressed through targeted stretching and progressive strength training, focused especially on reactivating the quadriceps. Finally, movement pattern retraining helps ingrain proper mechanics. Areas to emphasize include squatting, lunging, walking gait, running, jumping and landing. The goal is to eliminate any asymmetries or compensations that could lead to abnormal forces through the joint. Throughout this process, communication with the care team is key to calibrate the program to avoid flare-ups while still stimulating progress.
Anti-inflammatory medications
Ice, compression, elevation
Restoring range of motion
Eliminating muscle imbalances
Normalizing movement patterns
2: Rehabilitation Phases and Focus Areas
Phase
Timing
Goals
Inflammation & Early ROM
0-2 weeks
– Manage swelling/pain<br>- Regain mobility
Intermediate ROM & Early Strengthening
3-6 weeks
– Improve quad strength<br>- Single leg stability
Advanced Strengthening & Neuromuscular Control
6-12 weeks
– Running mechanics<br>- Multi-plane agility
Return to Sport
4+ months
– Sport-specific training<br>- Confidence in knee function
Muscular Imbalances
Concurrently, muscular imbalances around the knee joint develop, most notably quadriceps inhibition and weakness. The quadriceps muscles play a crucial role in stabilizing the knee joint. When weakened and inhibited after surgery, abnormal forces are transmitted through the joint, exacerbating pain and dysfunction.
Biomechanical Changes
Finally, biomechanical alterations including asymmetric gait patterns and improper landing mechanics cause further pain. A careful evaluation of all these contributing trigger points through a full physical therapy examination is key to pinpointing the optimal treatment approach.
Managing Knee Pain
Rehabilitation Program
Effective knee pain management requires a multifaceted rehabilitation program tailored to the individual’s specific deficits and dysfunctions.
Early Phase
The priority initially is controlling inflammation through ice, compression, medication, and activity modification. Once pain and swelling have been reined in, restoring full knee mobility is essential for reducing stiffness and dysfunction. Gentle manual therapy techniques and range of motion exercises facilitate this process.
Later Phase
As mobility improves, muscular imbalances must be addressed through targeted stretching and progressive strength training, focused especially on reactivating the quadriceps.
Movement Retraining
Finally, movement pattern retraining helps ingrain proper mechanics. Areas to emphasize include squatting, lunging, walking gait, running, jumping and landing. The goal is to eliminate any asymmetries or compensations that could lead to abnormal forces through the joint. Throughout this process, communication with the care team is key to calibrate the program to avoid flare-ups while still stimulating progress.
Optimizing Long-Term Outcomes
Preventing Re-Injury
Due to the high risk of retear after ACL reconstruction, prevention of re-injury is paramount during recovery. Gradually building up strength and then progressing activity in a controlled manner based on specific objective criteria allows tissues to heal while regaining function.
As the graft incorporation stretches beyond 6 months, impact activities can be cautiously integrated. However, pivoting sports may need to wait 9 months or more. Maintaining quadriceps and core strength and allowing the full return of power and agility prior to discharge from therapy ensures the knee can withstand demands of sport. Sticking to activity guidelines, along with smart training periodization can optimize recovery even years after ACL surgery.
Unraveling the Mystery Behind Knee Discomfort: A Comprehensive Guide to Knee Pain Causes
Introduction
Knee pain is a common ailment that can significantly impact mobility and quality of life. Understanding the underlying causes of knee pain is crucial for effective treatment and prevention.
In this comprehensive guide, we will delve into the various causes of knee pain, exploring the biomechanics of the knee joint and the role of surrounding muscles and ligaments. We will discuss common knee pain conditions, diagnostic tests, and treatment options for specific knee pain causes.
Biomechanics of the Knee Joint
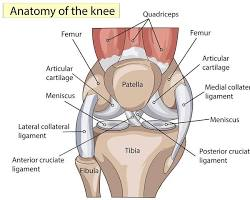
The knee joint is a complex structure that bears significant weight and facilitates movement. It consists of the thigh bone (femur), shinbone (tibia), kneecap (patella), and various ligaments, tendons, and cartilage.
Ligaments: Strong bands of connective tissue that connect bones and provide stability to the joint.
Tendons: Connect muscles to bones and transmit the force generated by muscle contraction.
Cartilage: Cushions the bones and prevents friction within the joint.
Common Knee Pain Conditions
Patellofemoral pain syndrome (PFPS): Pain caused by misalignment of the kneecap in the groove of the thigh bone.
Gout: Medication to reduce inflammation and prevent gout attacks.
Conclusion
Knee pain can arise from various causes, affecting individuals of all ages and activity levels. Understanding the underlying causes of knee pain is essential for proper diagnosis, treatment, and prevention. By consulting a healthcare professional and following their recommendations, you can effectively manage knee pain, improve mobility, and maintain overall joint health.
Common Knee Pain Conditions and Treatment Options
Condition
Treatment
Patellofemoral pain syndrome (PFPS)
Rest, ice, compression, elevation (RICE), strengthening exercises, and physical therapy.
Anterior cruciate ligament (ACL) tear
Surgical reconstruction of the ACL.
Meniscal tear
Rest, pain management, or surgical repair, depending on severity.
Osteoarthritis
Weight management, exercise, pain relievers, and joint injections.
Rheumatoid arthritis
Medication to manage inflammation and slow joint damage.
Gout
Medication to reduce inflammation and prevent gout attacks.
Healing Process for Knee Ligament Damage: A Professional Guide
As healthcare professionals, we understand the importance of knee ligaments in maintaining stability and mobility in the knee joint. Unfortunately, ligament injuries are common, especially in individuals who engage in physical activity. A ligament injury can be debilitating and may limit an individual’s ability to perform daily activities. In this article, we will discuss the three-step healing process for knee ligament damage.
Understanding Ligament Damage and Its Implications is the first step in the healing process. Knee ligaments are strong, fibrous tissues that connect the bones in the knee joint. When a ligament is damaged, it can result in pain, swelling, and instability in the knee joint. The severity of the injury can range from mild to severe, depending on the degree of damage to the ligament. It is crucial to diagnose and treat a ligament injury promptly to prevent further damage and complications.
Treatment and Rehabilitation of Ligament Damage is the second step in the healing process. The treatment plan for a ligament injury depends on the severity of the injury. Mild injuries may require rest, ice, compression, and elevation (RICE) therapy, while severe injuries may require surgery. Rehabilitation is an essential aspect of the healing process, and it involves exercises and physical therapy to restore strength, flexibility, and mobility in the knee joint.
Key Takeaways
Understanding the implications of ligament damage is crucial in the healing process.
Treatment plans for knee ligament damage vary based on the severity of the injury.
Rehabilitation is a vital aspect of the healing process and can help restore strength, flexibility, and mobility in the knee joint.
Understanding Ligament Damage and Its Implications
When it comes to knee injuries, ligament damage is one of the most common. Ligaments are the tough, fibrous bands of tissue that connect bones to each other and provide stability and strength to the joint. However, when these ligaments are damaged, it can lead to pain, tenderness, swelling, inflammation, stiffness, and a limited range of motion.
Types of Ligament Injuries
There are several types of ligament injuries that can occur in the knee, including sprains, ruptures, and strains. The most common type of knee ligament injury is an anterior cruciate ligament (ACL) tear, which can occur during sports or other physical activities that involve sudden stops or changes in direction.
Signs and Symptoms
The signs and symptoms of a knee ligament injury can vary depending on the severity of the injury. Common symptoms include pain, tenderness, swelling, inflammation, stiffness, and a limited range of motion. In more severe cases, the knee may feel unstable or give out when weight is placed on it.
Diagnosis and Evaluation
If you suspect that you have a knee ligament injury, it is important to seek medical attention from a specialist or physical therapist. They will perform a thorough evaluation to determine the severity of the injury and the best course of treatment. This evaluation may include X-rays or an MRI to assess the extent of the damage.
Overall, understanding the implications of ligament damage is critical to properly diagnose and treat knee injuries. If you experience any symptoms or have any questions, it is important to seek medical attention as soon as possible.
Treatment and Rehabilitation of Ligament Damage
At times, knee ligament damage can be a painful experience that may require treatment and rehabilitation. We have put together a comprehensive guide to help you understand the treatment process and how to rehabilitate your knee ligament damage.
Initial Treatment and Pain Management
The initial treatment for knee ligament damage involves rest, ice, compression, and elevation (RICE). RICE helps reduce swelling, pain, and inflammation around the affected area. We recommend using nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen to manage pain and inflammation.
different types of knee injuries, their typical healing times, and recovery notes:
Injury
Healing Time
Recovery Notes
Bone bruise
2-4 weeks
Rest, ice, compression. Gradual return to activity over 1-2 months.
Meniscus tear – minor
4-6 weeks
Often heals with conservative treatment.
Meniscus tear – moderate/severe
12+ weeks
Often requires surgery. Multi-month recovery common.
MCL tear – grade 1/2
3-6 weeks
Healing progresses well if braced.
MCL tear – grade 3
8-12 weeks
Often requires surgical repair/reconstruction followed by extensive rehab.
LCL sprain
4-8 weeks
Bracing to stabilize knee throughout healing.
ACL tear – partial
Up to 8 weeks
May heal with rehab/bracing or require surgical reconstruction.
Requires reconstructive surgery with graft. Months of rehab.
Patellar dislocation
6 weeks
Knee immobilized in early recovery. Later rehab focuses on realignment.
Patellar fracture
6-8 weeks
Cast/brace to immobilize. Surgical fixation may be necessary.
Arthritis flare up
1-4 weeks
Resting the joint along with anti-inflammatory meds helps recovery.
Recovery times are general estimates and can vary significantly depending on injury severity. Re-injury risks can persist even months after the acute healing phase
Surgical Intervention and Post-Surgery Care
In some cases, surgical intervention may be necessary to repair the damaged ligament. Surgery is typically followed by a period of rest, ice, compression, and elevation. Physical therapy and rehabilitation exercises may also be recommended to help regain range of motion and strength.
Rehabilitation and Therapy
Physical therapy and rehabilitation exercises are an essential part of the recovery process. Rehabilitation exercises help to strengthen the muscles around the knee and improve range of motion. We recommend working with a physical therapist to develop a personalized rehabilitation plan.
Advanced Treatments and Techniques
Advanced treatments and techniques such as tissue engineering, mesenchymal stem cells, and platelet-rich plasma may be used to promote healing and regeneration of the damaged ligament. We recommend discussing these options with your doctor to determine if they are appropriate for your specific condition.
Prevention and Future Care
Prevention and future care are essential to avoid re-injury and maintain healthy knee ligaments. We recommend engaging in regular physical activity and exercise to improve strength and flexibility. We also recommend wearing appropriate protective gear during sports activities to minimize the risk of injury.
In conclusion, knee ligament damage can be a painful experience, but with proper treatment and rehabilitation, you can recover and regain your strength and mobility. Remember to always consult with your doctor and physical therapist to develop a personalized treatment plan that meets your specific needs.
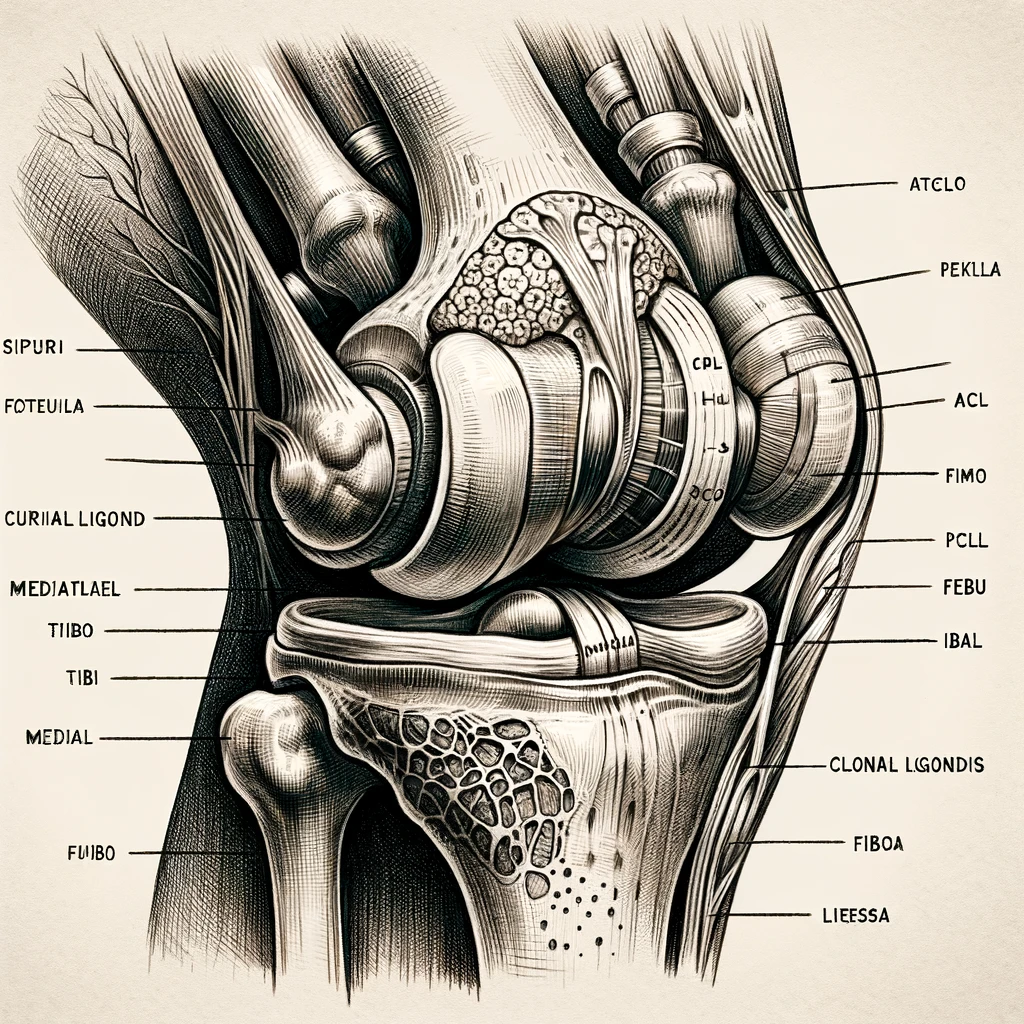
Comprehensive Guide to Knee Ligaments: Anatomy, Function, and Injuries
Knee ligament injuries can be painful and debilitating, affecting the quality of life of many individuals. Understanding knee ligament anatomy and associated conditions can help prevent injuries and ensure proper treatment. In this comprehensive guide, we will explore knee ligaments and their role in knee stability, common knee ligament injuries, and treatment and management strategies.
The knee joint is one of the most complex joints in the human body, consisting of bones, cartilage, tendons, and ligaments. Knee ligaments play a crucial role in providing stability and support to the joint. The four main knee ligaments include the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). These ligaments work together to control knee movement and prevent excessive rotation and translation.
Knee ligament injuries are common among athletes and can occur due to sudden twisting or impact to the knee joint. These injuries can cause pain, swelling, and limited mobility, which can lead to disability if left untreated. Early diagnosis and proper treatment can help prevent long-term complications and improve outcomes.
Understanding Knee Ligaments and Associated Conditions
At the core of knee joint stability are the ligaments that connect the bones of the knee together. The knee joint is comprised of four major ligaments that connect the femur to the tibia and fibula: the anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), the medial collateral ligament (MCL), and the lateral collateral ligament (LCL).
Anatomy of Knee Ligaments
The ACL and PCL are located inside the knee joint, while the MCL and LCL are located on the outside of the joint. These ligaments are made up of collagen and elastic fibers that provide strength and stability to the knee joint. The ACL is responsible for preventing the tibia from moving too far forward, while the PCL prevents the tibia from moving too far backward. The MCL and LCL work together to prevent the knee from moving side to side.
Common Injuries and Disorders
Ligament injuries are a common cause of knee pain and can range from mild sprains to complete tears. ACL tears are one of the most common knee injuries and often occur in athletes who participate in high-impact sports. PCL injuries are less common and typically occur as a result of a direct blow to the front of the knee. MCL and LCL injuries are usually caused by a direct blow to the outer or inner knee, respectively.
Osteoarthritis is another common disorder that affects the knee joint. It is a degenerative joint disease that is characterized by the breakdown of cartilage in the knee joint. Rheumatoid arthritis is an autoimmune disorder that can also affect the knee joint.
Epidemiology and Risk Factors
Knee ligament injuries are more common in athletes who participate in high-impact sports such as football, basketball, and soccer. Overuse injuries are also common in athletes who participate in running and jumping sports. Advancing age, sedentary lifestyle, smoking, and low income are all risk factors for knee osteoarthritis.
Pain and Mental Health Considerations
Knee pain can have a significant impact on an individual’s mental health and quality of life. Chronic pain syndromes, such as chronic musculoskeletal pain, can lead to anxiety, depression, and sleep disorders. Local pain, neuropathic pain, somatic pain, and visceral pain are all types of pain that can be associated with knee injuries and disorders. Insomnia and other sleep disorders are common in individuals with chronic pain and can further exacerbate the impact on quality of life.
The Impact on Quality of Life
Knee pain and associated conditions can have a significant impact on an individual’s quality of life. Disability, social interactions, and overall physical and mental health can all be affected by knee pain and related disorders.
Diagnostic Tools and Techniques
Diagnostic tools and techniques for knee injuries and disorders include X-rays, MRI scans, and physical examinations. Patient assessments are also important in determining the extent of the injury or disorder and developing an appropriate treatment plan.
In conclusion, understanding knee ligaments and associated conditions is essential for maintaining knee joint health and preventing injury. By understanding the anatomy of knee ligaments, common injuries and disorders, epidemiology and risk factors, pain and mental health considerations, the impact on quality of life, and diagnostic tools and techniques, individuals can take steps to prevent knee injuries and manage knee pain and related disorders.
Treatment and Management Strategies
When it comes to knee ligament injuries, treatment and management strategies vary depending on the severity and type of injury. In this section, we will discuss the various treatment options for knee ligament injuries. We will divide the treatment options into five subsections: non-surgical interventions, surgical procedures, pharmacological approaches, interventional strategies, and prognosis and outcome measures.
Non-Surgical Interventions
Non-surgical interventions are often the first line of treatment for knee ligament injuries. These interventions include rest, ice, compression, and elevation (RICE), physical therapy, and neuromuscular training. Physical therapy and neuromuscular training are particularly effective for patients with moderate-to-severe chronic pain or brief episodes of knee pain. These interventions can help improve lower extremity kinematics, reduce patellofemoral pain syndrome, and prevent sarcopenia.
Patient education is an essential component of non-surgical interventions. Patients need to understand the importance of proper posture, body mechanics, and preventive strategies. Patients should also be taught non-pharmacological pain control techniques like meditation, deep breathing exercises, and relaxation techniques.
Surgical Procedures
Surgical procedures are typically reserved for patients with severe knee ligament injuries that do not respond to non-surgical interventions. The most common surgical procedures include knee arthroplasty, total knee arthroplasty, hip arthroplasty, and total hip arthroplasty. Preoperative planning and surgical technique are critical to ensure successful outcomes.
Pharmacological Approaches
Pharmacological approaches are often used in conjunction with non-surgical and surgical interventions. The most common pharmacological therapies include corticosteroids, mesenchymal stem cells, nonsteroidal anti-inflammatory drugs (NSAIDs), and opioids. Pharmacological therapies can help reduce pain and inflammation, improve functional outcomes, and enhance the patient’s overall quality of life.
Interventional Strategies
Interventional strategies are minimally invasive procedures that can help manage knee ligament injuries. These strategies include interventional pain therapy, multimodal analgesia, and multidisciplinary intervention. Interventional strategies can help improve functional level, reduce pain, and enhance functional outcomes.
Prognosis and Outcome Measures
Prognosis and outcome measures are essential to assess the effectiveness of treatment and management strategies for knee ligament injuries. Outcome measures include functional outcomes, patient satisfaction, and quality of life. Prognosis is influenced by age and sex, pediatric population, manual labor, urban and rural populations, and rheumatologic problems.
In conclusion, knee ligament injuries require a multidisciplinary approach to treatment and management. Non-surgical interventions, surgical procedures, pharmacological approaches, interventional strategies, and prognosis and outcome measures are all important components of a comprehensive treatment plan. With the right treatment and management strategies, patients can achieve improved outcomes and a better quality of life.
Different Types of Knee Ligament Injuries: A Professional Overview
Knee ligament injuries are common among athletes and can result in significant pain and discomfort. Understanding the different types of knee ligament injuries can help individuals recognize the symptoms and seek appropriate treatment. Knee ligaments are strong, fibrous bands that connect the thigh bone to the lower leg bones, providing stability and support to the knee joint.
There are four primary ligaments in the knee: the anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), the medial collateral ligament (MCL), and the lateral collateral ligament (LCL). Each of these ligaments plays a critical role in the function of the knee joint and can be injured in a variety of ways. For example, ACL injuries are common among athletes who engage in high-impact sports like football and basketball, while MCL injuries are more frequently seen in skiing and other winter sports.
Some common causes of these knee ligament and tendon injuries are sudden stops/twists, blows to the knee, hyperextension, and frequent overuse in sports. Treatment varies depending on severity but may involve RICE (rest, ice, compression, elevation), immobilization brace, physical therapy, medications, or surgery.
details on a few common knee ligament injuries and their typical treatments:
ACL Tear:
Most commonly caused by sudden stops/change in direction, hyperextension, or direct blow
Can be partial or complete tears
Nonsurgical treatment may be used for partial tears or non-athletes: rehab to strengthen muscles around knee, bracing
But most ACL tears, especially complete tears or athletes, require reconstructive surgery using a tissue graft
Caused by direct blow or valgus stress (knee pushed inwards)
Minor sprains can heal with RICE, bracing, rehab
More severe Grade 3 sprains may require surgery to repair or reconstruct ligament
Meniscus Tear:
Often caused by sudden twisting motion
Partial tears may heal with conservative treatment – physical therapy, brace, injections
Surgery usually required for complex, unstable tears or tears with mechanical symptoms (locking, catching, etc.)
Surgery removes damaged meniscus or repairs tears through suturing
PCL Tear:
Most result from direct blow/force to flexed knee (dashboard injuries)
Nonsurgical treatment can be tried especially partial tears – rehab, bracing
Surgical options are PCL repair, reconstruction with tissue graft
The specifics of treatment really depend on factors like location/severity of injury, patient age and activity level. But in general, mild sprains do well with conservative care, while severe ligament tears often require surgery. Let me know if you have any other questions!Copy
knee ligament injuries and their treatments :
Injury
Cause
Symptoms
Nonsurgical Treatment
Surgical Treatment
ACL Tear
Sudden stops/change of direction, hyperextension, direct blows
Knee ligaments are strong, fibrous bands that connect the thigh bone to the lower leg bones, providing stability and support to the knee joint.
The four primary ligaments in the knee are the anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), the medial collateral ligament (MCL), and the lateral collateral ligament (LCL).
ACL injuries are common among athletes who engage in high-impact sports like football and basketball, while MCL injuries are more frequently seen in skiing and other winter sports.
Understanding Knee Ligament Injuries
As orthopedic specialists, we understand that knee injuries can be debilitating and painful. Knee ligament injuries are a common type of knee injury that can cause knee pain and limit passive range of motion. In this section, we will discuss two of the most common types of knee ligament injuries: Anterior Cruciate Ligament (ACL) Injuries and Meniscal Injuries.
Anterior Cruciate Ligament Injuries
The ACL is one of the four main ligaments in the knee that connects the femur to the tibia. It is responsible for controlling rotation and forward movement of the tibia. ACL injuries are a common type of knee injury, especially among athletes who engage in high-impact sports such as football, soccer, and basketball.
An ACL tear can occur due to a traumatic injury, such as a sudden stop or change in direction, or due to degenerative changes in the knee over time. Symptoms of an ACL tear include knee pain, swelling, and instability. An ACL tear is typically diagnosed through a physical exam, imaging tests such as an MRI, and arthroscopy.
Treatment for an ACL tear may involve nonsurgical options such as physical therapy and bracing, or surgical options such as ACL reconstruction. ACL reconstruction involves replacing the torn ACL with a graft, typically from the patellar tendon or hamstring tendon.
Meniscal Injuries
The menisci are two crescent-shaped pieces of cartilage in the knee that act as shock absorbers and help to distribute weight evenly across the knee joint. Meniscal injuries are a common type of knee injury, especially among athletes who engage in high-impact sports.
Meniscal tears can occur due to a traumatic injury or due to degenerative changes in the knee over time. Symptoms of a meniscal tear include knee pain, swelling, and clicking or locking of the knee joint. A meniscal tear is typically diagnosed through a physical exam, imaging tests such as an MRI, and arthroscopy.
Treatment for a meniscal tear may involve nonsurgical options such as physical therapy and bracing, or surgical options such as meniscal repair or meniscectomy. Meniscal repair involves suturing the torn meniscus back together, while meniscectomy involves removing the torn portion of the meniscus.
In conclusion, knee ligament injuries such as ACL injuries and meniscal injuries can cause knee pain and limit passive range of motion. It is important to seek medical attention if you suspect you have a knee injury. Treatment options vary depending on the severity of the injury and may involve nonsurgical or surgical options.
Treatment and Rehabilitation
When it comes to treating knee ligament injuries, there are a few different options available. Depending on the severity of the injury, surgical procedures may be necessary. In less severe cases, non-surgical treatments such as physical therapy and rehabilitation exercises may be recommended.
Surgical Procedures
Surgical procedures for knee ligament injuries can include knee surgery or knee replacement. Knee surgery may involve arthroscopic lavage or debridement, which is the removal of damaged tissue from the knee joint. In more severe cases, surgical procedures may be necessary to repair or replace damaged ligaments or cartilage.
Cartilage Regeneration Techniques
Cartilage regeneration techniques are used to repair damaged cartilage in the knee joint. Techniques such as marrow stimulation and autologous chondrocyte implantation can be used to regenerate cartilage and promote healing. These techniques involve the use of chondrocytes, which are cells that produce and maintain cartilage tissue.
It is important to note that post-traumatic osteoarthritis can develop after knee ligament injuries, especially if they are not treated properly. To prevent this, it is important to follow a rehabilitation program that includes exercises to strengthen the muscles around the knee joint and improve knee kinematics. Additionally, large animal models such as rabbits, sheep, goats, pigs, and dogs have been used for translational work in this field.
In conclusion, there are various treatments available for knee ligament injuries, ranging from non-surgical options such as physical therapy to surgical procedures such as knee replacement. Cartilage regeneration techniques can also be used to promote healing and prevent post-traumatic osteoarthritis. It is important to follow a rehabilitation program to prevent further damage and promote healing.
Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev. Saude Publica. 2015;49:1. https://doi.org/10.1590/S0034-8910.2015049005874.
Article PubMed PubMed Central Google Scholar
Ay S, Evcik D. Depression and quality of life in patients with chronic low back pain. Department of Physical Medicine and Rehabilitation. Ankara New Medical Journal. 2008; 25:228–31.
Google Scholar
Bogduk N. On the definitions and physiology of back pain, referred pain and radicular pain. Pain. 2009;147(1–3):17–9. https://doi.org/10.1016/j.pain.2009.08.020.
Article PubMed Google Scholar
van Tulder M, Becker A, Bekkering T, Breen A, del Real MTG, Hutchinson A, Bart Koes B, Laerum E, Malmivaara A. Chapter 3 European guidelines for the treatment of acute non-specific low back pain in primary care. Eur Spine J. 2006; 15:169–91. https://doi.org/10.1007/s00586-006-1071-2.
Article Google Scholar
Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database System Rev. 2021;28(9):CD009790. https://doi.org/10.1002/14651858.CD009790.pub2.
Article Google Scholar
Allen RJ. Physical agents used by physiotherapists in the treatment of chronic pain. Phys Med Rehabil Clin N Am. 2006; 17:315–45. https://doi.org/10.1016/j.pmr.2005.12.007.
Article PubMed Google Scholar
Qaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of Physicians, Denberg TD, Barry MJ, Boyd C, Chow RD, Fitterman N, Harris RP, Humphrey LL, Vijan S. Noninvasive treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–30. https://doi.org/10.7326/M16-2367.
Article PubMed Google Scholar
KramerJF. Ultrasound: evaluation of its mechanical and thermal effects. Arch Phys Med Rehabilitation. 1984; 65:223–7.
CAS PubMed Google Scholar
Maxwell L. Therapeutic ultrasound: its effects on the cellular and molecular mechanisms of inflammation and repair. Physiotherapy. 1992; 78:421–6. https://doi.org/10.1016/S0031-9406(10)61528-3.
Article Google Scholar
Kitchen S, Partridge C. Review of continuous and pulsed shortwave diathermy patterns. Physiotherapy. 1992; 78:243–52. https://doi.org/10.1016/S0031-9406(10)61434-4.
Article Google Scholar
Unlu Z, Tasci S, Tarhan S, Pabuscu Y, Islak S. Comparison of 3 physiotherapy modalities for acute pain in lumbar disc herniation measured by clinical evaluation and magnetic resonance imaging. J Manipulative physiotherapy. 2008;31(3):191–8. https://doi.org/10.1016/j.jmpt.2008.02.001.
Article Google Scholar
Ebadi S, Henschke N, Forogh B, Nakhostin Ansari N, van Tulder MW, Babaei-Ghazani A, Fallah E. Therapeutic ultrasound for chronic low back pain. Cochrane Database System Rev. 2020;7(7):CD009169. https://doi.org/10.1002/14651858.CD009169.pub3.
Article PubMed Google Scholar
Seco J, Kovacs FM, Urrutia G. The efficacy, safety, effectiveness and cost-effectiveness of ultrasound and shock wave therapies for low back pain: a systematic review. Rug J 2011;11:966–77. https://doi.org/10.1016/j.spinee.2011.02.002.
Article PubMed Google Scholar
Kreiner DS, Hwang SW, Easa JE, Resnick DK, Baisden JL, Bess S, Cho CH, DePalma MJ, Dougherty P 2nd, Fernand R, et al. North American Spine Society. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Rug J 2014;14(1):180–91. https://doi.org/10.1016/j.jmpt.2008.02.001.
Article PubMed Google Scholar
Chapman JR, Norvell DC, Hermsmeyer JT, Bransford RJ, DeVine J, McGirt MJ, Lee MJ. Evaluation of common outcomes for measuring treatment success for chronic low back pain. Spine. 2011;36:S54–68. https://doi.org/10.1097/BRS.0b013e31822ef74d.
Article PubMed Google Scholar
Chiarotto A, Maxwell LJ, Terwee CB, Wells GA, Tugwell P, Ostelo RW. Roland-Morris Disability Questionnaire and Oswestry Disability Index: which has better measurement properties for measuring physical functioning in non-specific low back pain? Systematic review and meta-analysis. Phys Ther. 2016;96(10):1620–37. https://doi.org/10.2522/ptj.20150420.
Article PubMed Google Scholar
Yakut E, Düger T, Oksüz C, Yörükan S, Ureten K, Turan D, Frat T, Kiraz S, Krd N, Kayhan H, Yakut Y, Güler C. Validation of the Turkish version of the Oswestry Disability Index for patients with low backache. Spine. 2004;29(5):581–5.
Article PubMed Google Scholar
True JEJ, Sherbourne CD. The MOS 36-item short health survey (SF-36). I. Conceptual framework and item selection. Medical care. 1992;30:473–83.
Article PubMed Google Scholar
Demiral Y, Ergor G, Unal B, Semin S, Akvardar Y, Kivircik B, Alptekin K. Normative data and distinctive properties of short form 36 (SF-36) in Turkish urban population. BMC Public Health. 2006;6:247.
Article PubMed PubMed Central Google Scholar
Ansari NN, Ebadi S, Talebian S, Naghdi S, Mazaheri H, Olyaei G, Jalaie S. A randomized, single-blind, placebo-controlled clinical trial of the effect of continuous ultrasound on low back pain. Electromyogr Clin Neurophysiol. 2006;46(6):329–36.
CAS PubMed Google Scholar
Saghaei M. Random assignment software for parallel-group randomized trials. BMC Med Res Method. 2004;4:26. https://doi.org/10.1186/1471-2288-4-26.
Robertson VJ, Baker KG. A review of therapeutic ultrasound: effectiveness studies. Phys Ther. 2001;81(7):1339–50.
Article CAS PubMed Google Scholar
Miller DL, Smith NB, Bailey MR, Czarnota GJ, Hynynen K, Makin IR. Bioeffects Committee of the American Institute of Ultrasound in Medicine. Overview of therapeutic ultrasound applications and safety considerations. J Echo Med. 2012;31(4):623–34. https://doi.org/10.7863/jum.2012.31.4.623.
Article PubMed PubMed Central Google Scholar
Noori SA, Rasheed A, Aiyer R, Jung B, Bansal N, Chang KV, Ottestad E, Gulati A. Therapeutic ultrasound for pain management in chronic low back pain and chronic neck pain: a systematic review. Pain Med. 2020;7(21):1482–93. https://doi.org/10.1093/pm/pny287.
Article Google Scholar
Haile G, Hailemariam TT, Haile TG. Effectiveness of ultrasound therapy in the treatment of chronic nonspecific low back pain: a systematic review. J Pain Res. 2021;14:1251–7. https://doi.org/10.2147/JPR.S277574.
Benincá IL, de Estéfani D, Pereira de Souza S, Weisshahn NK, Haupenthal A. Tissue heating in different shortwave diathermy methods: a systematic review and narrative synthesis. J Bodyw Mov Ther. 2021;28:298–310. https://doi.org/10.1016/j.jbmt.2021.07.031.
Article PubMed Google Scholar
Dos Reis do Nascimento DM, Raab FGC, Silva GLH, de Andrade AM, Ferreira PML, Silveira GAR, Brandt de Macedo AC. Immediate analgesic effect of two forms of short-wave diathermy in chronic low back pain: study protocol for a randomized controlled trial. Pain management. 2022;12(2):131–9. https://doi.org/10.2217/pmt-2021-0026.
Article CAS PubMed Google Scholar
Abdulla FA, Alsaadi S, Sadat-Ali M, Alkhamis F, Alkawaja H, Lo S. Effects of pulsed low-frequency magnetic field therapy on pain intensity in patients with chronic low back musculoskeletal pain: study protocol for a randomized double-blind placebo-controlled trial. BMJ opened. 2019;9(6):e024650. https://doi.org/10.1136/bmjopen-2018-024650.
Article PubMed PubMed Central Google Scholar
Shields N, Gormley J, O’Hare N. Shortwave diathermy: a review of existing clinical trials. Phys Ther Rev. 2001;6(2):101–18. https://doi.org/10.1002/pri.259.
Article Google Scholar
Paladini LH, Almeida N, Korelo RIG, Michel de Macedo R, Guarita-Souza LC, Zotz TGG, Brandt de Macedo AC. Shortwave therapy in patients with chronic low back pain: a systematic review. Column/Column. 2020;19(3):218–22. https://doi.org/10.1590/S1808-185120201903219301.
Article Google Scholar
Karasel S, Oncel S, Sonmez I. The effect of shortwave diathermy and exercise on depressive feelings in patients with chronic low back pain. Med Arch. 2021;75(3):216–20. https://doi.org/10.5455/medarh.2021.75.216-220.
Article PubMed PubMed Central Google Scholar
Shakoor MA, Rahman MS, Moyeenuzzaman M. Effects of deep heat therapy on patients with chronic low back pain. Mymensingh Med J. 2008;17(2):32–8.
This controlled pilot clinical study involved 60 patients admitted to Ghaem Hospital of Mashhad, Iran. These patients were specifically from the cardiac surgery intensive care unit and were admitted between May 2020 and January 2021 (Figure 1).
figure 1
CONSORT Flowchart of participants
Attendees
The study included patients who met specific inclusion criteria. These criteria required that patients be between 18 and 60 years old and willing to undergo non-emergency coronary transplant surgery. On the other hand, the exclusion criteria included patients who experienced loss of consciousness until the day after surgery, those who did not have a smartphone, individuals with severe postoperative arrhythmias and hemodynamic disorders, and patients who were prohibited by their physicians from participating in rehabilitation.
Intervention
Software production
Prior to the design of the software, extensive research was done to prepare its contents. This involved reviewing various texts, including articles, reference works, and gathering insights from experienced nurses in specialist care units. The content was then submitted to a panel of ten specialists for validation, and their suggested revisions were incorporated.
The software’s educational content covered a range of topics, including breathing and diaphragm exercises, instructions on physical exercises and their proper performance, discussions and interactions with patients, and encouragement for patients to participate in routine activities. These concepts were presented primarily through instructional videos and engaging animations.
Once the content was ready, it was handed over to the software development and information technology team for creating the software. After the initial software was developed, a specialized validation process was carried out by ten IT experts to ensure its functionality and effectiveness.
To validate the software, both white-box and black-box testing methods were used. In black-box testing, users without knowledge of the software’s internal structure enter the desired items and verify the recorded information. The purpose is to ensure accurate data recording. White-box testing, on the other hand, requires users to have knowledge of the software’s internal structure and is typically performed by designers or experts. For example, to assess the speed of the software, several items were selected at different speeds and the accuracy of the selections was examined.
The next phase included compatibility testing and security testing. Compatibility testing involved installing the application on multiple Android smartphones and tablets to assess performance on each device. In the security testing, a double confirmation method was implemented to ensure accurate recording of each patient’s problems. This required the patient to confirm the selected item by clicking again, which reduced the chance of inadvertent data entry errors.
The augmented reality software is registered and approved within the electronic services system of the Information Technology Organization of Iran.
To evaluate patient satisfaction with the augmented reality software, the Mobile Application Rating Scale (MARS) was used.
This scale evaluates the quality and performance of the application on four dimensions: attractiveness (5 questions), functionality (4 questions), aesthetics (3 questions), information (7 questions) and subjective quality (4 questions). Each item in the scale was rated on a five-point scale. The maximum achievable score was 115, while the minimum acceptable score was set at 23. For a detailed presentation of the results, please refer to (Table 1).
Table 1 Mean and standard deviation of dimensions of MARS questionnaire
Phase I cardiac rehabilitation training based on augmented reality
After establishing the necessary agreements with officials at Ghaem Hospital in Mashhad, Iran, the first author of the study initiated the sampling process. In the intervention group, rehabilitation program training began upon patient entry into the cardiac surgery intensive care unit and continued until the patient’s discharge.
During several sessions, augmented reality software was used to train patients in physical activities, such as walking around the hospital ward and climbing stairs. These exercises were performed under the direct supervision of the researcher and were taught individually to each patient using the augmented reality software. The duration of physical activity varied depending on the patient’s condition and the length of hospital stay, ranging from 5 to 10 minutes. During the rehabilitation sessions, the ECG and perceived exercise intensity were closely monitored and controlled.
In the control group, the rehabilitation training program was implemented using a routine method based on the Ministry of Health protocol. The researcher provided face-to-face training within the unit. Both the intervention and control groups completed the cardiac self-efficacy questionnaire upon admission and discharge to the special care cardiac surgery department.
Results
The data collection process used two demographic information questionnaires and a cardiac self-efficacy questionnaire.
The cardiac self-efficacy questionnaire used in this study was the Cardiovascular Management Self-Efficacy Questionnaire, which was developed by Estka of Italy in 2015. This questionnaire consists of 9 questions, each rated on a 5-point Likert scale, ranging from ‘completely confident’ to ‘not at all confident’. The questionnaire consists of three subscales.
The first four questions assess a person’s belief in their ability to quit smoking, maintain good nutrition, exercise, and avoid stressful situations. This subscale is called cardiac risk factor self-efficacy. Questions 5 and 6 relate to a person’s confidence in remembering to take medications correctly, which reflects self-efficacy for medication adherence. Finally, questions 7 through 9 evaluate a person’s belief in their ability to identify symptoms and signs of disease worsening, indicating self-efficacy in recognizing symptoms.
Each answer is assigned a score, with ‘not at all confident’ given a score of one, ‘somewhat confident’ given a score of two, ‘somewhat confident’ given a score of three, ‘fairly confident’ given a score of four, and “completely confident” with a score of five. Total scores range from 9 to 45, with higher scores indicating greater self-efficacy in cardiovascular management [21]. Borzou et al. (2017) evaluated the validity and reliability of this tool in Iran [33]. Patients completed the Cardiovascular Management Self-Efficacy Questionnaire both before and after the intervention.
Sample size and randomization
The study involved the continuous and purposeful selection of patients who were then randomly assigned to one of two groups. After confirming that they met the inclusion criteria, eligible individuals were divided into intervention and control groups using a random sequence generated by SPSS software. This series was kept in a sealed envelope to ensure confidentiality. Although it was challenging to blind the participants in this study, the outcome assessors and statisticians were unaware of the type of intervention, ensuring a level of objectivity.
Because no comparable study was found examining the effectiveness of phase I cardiac rehabilitation training based on augmented reality on the self-efficacy of patients undergoing coronary artery bypass surgery, a sample size of 10 participants was determined for each group. The sample size was calculated using the mean comparison formula, with a 95% confidence interval and 80% test power for each group, resulting in a total of 20 participants. To account for the potential dropout rate, an additional 30 participants were added to each group, representing a 10% increase over the values calculated in the formula.
After data collection and sampling, the collected data was analyzed using SPSS 21. Various statistical tests were used, including the independent t-test, the Mann-Whitney test, the paired t-test, and the chi-square test. These tests were performed at a 95% confidence level to ensure statistical significance. Descriptive indicators such as mean, standard deviation and frequency were also used to provide a comprehensive overview of the data. Cohen’s d was also used to evaluate the magnitude of the effect size, calculated by standardized mean difference, with g > 0.2 to 0.5 = small effect size, g > 0.5 to 0.8 = medium effect size, and g > 0 .8 = large effect size [38].