In this study, YKL-40 serum levels are influenced by factors such as age, inflammation and diagnosis of autoimmune diseases (RA/MII)3. Currently, due to its participation in tissue remodeling and degradation, attempts have been made to use it as a biomarker in pro-inflammatory states and as an indicator of poor prognosis in inflammatory diseases.6.7. However, its usefulness is still controversial because its full biological effects are still unknown. Furthermore, the specific factors that promote its expression, as well as its interaction with the majority of cytokines and molecules involved in the development and establishment of autoimmune inflammatory diseases, are not well established.17.
YKL-40 serum levels have been reported to increase with age in various cardiovascular, metabolic and systemic inflammatory diseases3. Bojesen et al. found that serum levels of YKL-40 increased exponentially with aging. In subjects with two YKL-40 measurements ten years apart, the average increase in YKL-40 was 1.5 μg/l/year18. Regarding inflammatory diseases, increased serum levels of YKL-40 were reported in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis, which was hypothesized to play a role in promoting chemotaxis, tissue damage and vascular damage.19.
In RA it has been recognized as a potential candidate autoantigen. Furthermore, in these patients it is produced and secreted by monocytes differentiated into macrophages, articular chondrocytes, synovium, peripheral blood mononuclear cells (PBMCs), and endothelium.17,19,20. It has been proposed that the pathogenic mechanism of YKL-40 in RA initiates through its binding to the HLA-DR4 peptide-binding motif promoting mononuclear cell proliferation, and HLA-DM plays a key role in presenting YKL-40 to CD4+ T cells. Furthermore, antigen-presenting cells (APCs) present YKL-40 at early-stage RA sites, suggesting an association for YKL-40 in the pathogenesis of RA.20,21,22. On the other hand, differentiated DR4+ dendritic cells and macrophages are similar to APCs of synovial joints and have the potential to carry out MHC II presentation of YKL-40 epitopes, resulting in higher levels in synovial and serum.21,22. Although the pathogenic mechanism in RA has been elucidated, agents that promote YKL-40 expression in RA are still lacking. It has been associated with the development of chronic, destructive, relapsing arthritis due to its role in tissue remodeling and breakdown. . It is considered an effective marker in estimating RA disease activities and prognostic value, and may be a therapeutic target19.
As for IIM, information is even more limited as few studies have been conducted in this regard and thus the role YKL-40 plays in this area has not yet been established. Regarding the pro-inflammatory effect and its relationship with the diagnosis and phenotype of IIM, Noguchi et al. found significantly increased serum in patients with PM/DM compared to the healthy population, as well as age-adjusted serum YKL-40 levels were significantly increased in patients with PM/DM compared to HC. In muscle biopsies, infiltration of YKL-40-positive inflammatory cells (probably macrophages) in the endomysium and perimysium was found. This suggests that cells other than CD8+ and CD4+ T cells can cause inflammation.23.
Ming-Zhu Gao et al. measured YKL-40 levels in patients with DM/PM and HI and reported significantly higher levels in patients with IIM compared to controls (51.6 vs. 27.8 ng/ml, respectively)6. In a systematic review by Cui et al. reports levels of 84.09 ng/ml in patients with PM and DM versus 27.37 ng/ml in HI24. On the other hand, Carboni et al. analyzed YKL-40 serum levels and its expression in muscle tissue in patients with ASSD. However, serum levels of YKL-40 did not correlate with other clinical, laboratory, disease status, or therapeutic parameters. Furthermore, YKL-40 was expressed by the inflammatory cells of the muscle tissue.13. Our study reinforces these results with serum levels of 187.80 ng/ml in patients with IIM versus 46.82 ng/ml in RA and 57.17 ng/ml in HI, as well as their presence mainly in inflammatory cells. This increase can be explained by inflammation, activation of macrophages, destruction of fibroblasts and existing vascular changes.
As previously mentioned, several biological effects of YKL-40 are known, such as inflammation and tissue remodeling, as well as its main sources, which, however, highlights its exacerbated expression in inflammatory diseases such as RA or SLE; some researchers have pointed out that this expression may vary depending on the disease type, which could be due to the multi-organ damage in IIM compared to RA, where the damage is mainly directed against the joints19.24. Tang et al. found that YKL-40 concentration was significantly higher in IIM patients with myocardial injury than without myocardial injury25.
In addition, YKL-40 plays a role in cardiovascular diseases such as early atherosclerosis, essential hypertension and other progressive vascular complications. In IIM patients, as in many other autoimmune diseases, serum levels of this protein have a positive association, particularly with atherosclerosis, and may predict both overall and cardiovascular mortality.5,26,27.
We wanted to know whether YKL-40 is affected by certain factors in IIM, as mentioned by Tizaoui et al. First, we compared some demographic, laboratory and clinical variables between patients with RA and IIM mentioned in Table 1. Of all After analyzing the variants, we found a significant difference in pDBP (P = 0.024) and pMBP (P = 0.035) which were higher in IIM patients. This may be due to the fact that blood vessels suffer damage in the early stages of the development of inflammatory diseases, altering blood pressure and increasing the risk of cardiovascular damage.28.29. Furthermore, the endothelial changes in IIM progress to microangiopathy, causing blood pressure changes12. Although information on exactly how the process occurs is scarce, it has been suggested that cardiovascular disease and cardiovascular risk increase mortality in IIM patients, but this is becoming controversial because a single center cross-sectional study recently reported that it risk of cardiovascular disease increases. factors in IIM patients are not significant compared to HI, but are significant in IIM if they are related to age, disease duration, duration of therapy and body composition, which could be related to our patients included in our study25.30. Although these evaluated variables were significant between these two groups, serum levels of YKL-40 were the most significant variable (P = 0.010). These were higher in IIM than in RA patients (187.80 ng/ml). vs 46.82 ng/ml, respectively).
Once we established that IIM exhibits higher serum levels of YKL-40 than RA, we examined whether serum levels of YKL-40 were influenced by age or disease duration. Our results show that only aging has a positive correlation with increased YKL-40, but not with disease duration. The reports conducted by Johansen in 2006 and Schultz 2010 have clearly shown that aging is predictive of the increase of YKL-40 in HI, but in our IIM patients the concentration of this protein is higher due to inflammation and damage to multiple organs.2.3.
We evaluated the predictive value of inflammatory state, age and diagnosis of IIM on serum levels of YKL-40 and clarified that CRP has predictive value on serum YKL-40 levels in IIM patients.P= 0.038) which corresponds to a cross-sectional survey and systematic review published by Cui andYou at the . In addition, age and the IIM diagnosis ( P=0.008AndP=0.001respectively) were found to be powerful predictors of YKL-40 serum levels24. On the other hand, we confirmed that age and IIM diagnosis have an important influence on YKL-40 concentration, because YKL-40 serum levels are the highest compared to control and RA groups, thus we know that the presence of the disease or its type influences the disease. the YKL-40 concentration. Some reports state that the YKL-40 concentration in HI is stable for many years, but increases with aging or inflammatory conditions. Other researchers reported that normal YKL-40 serum levels may be different among a healthy population. Therefore, they recommend establishing baseline values for each study, because in addition to environmental factors, genetic load is another variable that can influence the expression pattern. of this protein26. We previously mentioned the pathogenic mechanism by which YKL-40 expression is mediated in RA and its possible role in IIM, but the information is still insufficient.
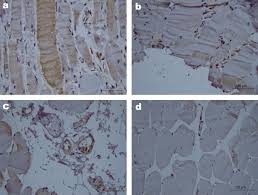
Regarding the in situ analysis of YKL-40 muscle expression, we observed that YKL-40 is mainly expressed in inflammatory cells rather than in muscle cells. We also observed that YKL-40 expression is associated with higher CPK serum levels and MYOACT score which are often related. to higher inflammation and muscle weakness. This observation is in agreement with the unique previous report of YKL-40 in muscle tissue made by Carboni et al.13It thus supports its role in inflammation, as well as its function as a clinical marker for poor prognosis in inflammatory diseases.
Taking into account all our findings, we demonstrated the expression of YKL-40 in both HI and in patients with RA and IIM and the possible factors that could influence its expression.
Leave a Reply