FDA Adverse Event Reporting System (FAERS)
The United States Food and Drug Administration Adverse Event Reporting System (FAERS) is a data repository that collects voluntary drug-related reports from healthcare professionals, consumers, and legal representatives. In cases where the adverse reaction (AE) is reported to the manufacturer, the manufacturer is required to forward the report to FAERS. At the time of the survey, FAERS contained 17,392,666 AE reports collected from the first quarter of 2004 (including historical reports since 1982) through the second quarter of 2022. The reports are available online: https://www.fda.gov/ medications/questions-and-answers-fdas-reporting-system-faers-side-effects/fda-reporting-system-faers-last-quarter-data.
Data preparation
FAERS reports are added quarterly and stored in a set of text files. Subsets of data are organized by specific report fields (demographics, drug, side effects, outcome, etc.) and their respective case IDs. The data format is not uniform and has changed several times since its inception. Therefore, appropriate changes have been made. Moreover, as the side effect reports are collected from all over the world, the respective brand names of drugs are translated into the generic equivalents19,20,21.
Study results
The MedDRA Dictionary version 25.1 was searched to define the measured study outcomes using higher-level terms such as “immune-associated conditions not elsewhere classified (NEC)” and “psoriatic conditions.” All psoriasis-associated preferred terms (PT) were used in the search. To avoid indication-related confounding effects, psoriatic conditions associated with RA, such as psoriatic arthropathy, were excluded from the MedDRA PT list. The following PTs were used for the definition psoriasis in the analysis: erythrodermic psoriasis, guttate psoriasis, nail psoriasis, psoriasiform dermatitis, pustular psoriasis and psoriasis.
Cohort selection
Of the total 17,392,666 adverse event reports in FAERS, a total of 881,182 reports included RA indications, and for 663,922 of these, RA was listed as the sole indication. These data were further broken down by monotherapies and only reports from physicians, pharmacists and other healthcare professionals were included to avoid bias and increase clinical relevance. The final monoindication + monotherapy sets were as follows: certolizumab pegol (n = 5168), adalimumab (n = 9221), golimumab (n = 2899), tocilizumab (n = 4819), abatacept (n = 7574), infliximab (n = 5579), rituximab (n = 2519), etanercept (n = 89543), tofacitinib (n = 10686), and methotrexate (n = 6142). Demographic analysis was performed for TNF inhibitors and methotrexate RA AE cohorts (Tables 1 and 2). The following terms for psoriasis are included: erythrodermic psoriasis, guttate psoriasis, nail psoriasis, psoriasiform dermatitis, pustular psoriasis and psoriasis. These psoriasis type terms describe the psoriasis Adverse event rates were calculated for each drug cohort: certolizumab pegol (n = 98), adalimumab (n = 107), golimumab (n = 20), tocilizumab (n = 29), abatacept (n = 40), infliximab (n = 29 ), rituximab (n = 11), etanercept (n = 260), tofacitinib (n = 24), and methotrexate (n = 7). A disproportionality analysis was performed using the reported AE rates to calculate the reporting odds ratios (RORs). These figures were used to calculate psoriasis reported frequencies. Methotrexate was selected as a control cohort because of its unique mechanism of action (MOA) as an immunosuppressant that inhibits the conversion of folic acid to folic acid cofactors, and because of its common use as a monotherapy in RA.
Demographic analysis
Gender (Table 1).
Age (Table 2).
static analysis
Descriptive statistics
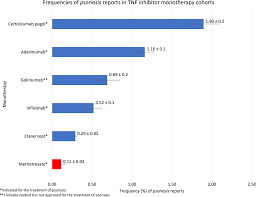
The frequencies for each side effect examined (Figs. 1, 3) were calculated using the following equation:
$$\textFrequency = \left( \textnReports\,\text with \,\textpsoriasis \,\textin \, \texta \,\textcohort \right)/\textnReports\,\text in \,\texta \,\ textcohort*100$$
(1)
Frequency error:
$$\textError = \left( \sqrt \textnReports \,\textwith\, \textpsoriasis\,\text in \,\text a\, \textcohort \right)/\textnReports\,\text in\,\text a \,\textcohort*100$$
(2)
Comparative statistics
The numbers of psoriasis reports were compared via the Reporting Odds Ratio (ROR) analysis for Fig. 2, 4 and 5 and Tables 3, 4 and 5 using the following equations:
$$\mathrmROR=(\mathrma/\mathrmb)/(\mathrmc/\mathrmd)$$
(3)
where Number of cases in exposed group with psoriasis, Number of cases in exposed group without psoriasis, Number of cases in control group with psoriasis, Number of cases in control group without psoriasis.
$$\mathrmLnROR=\mathrmLn(\mathrmROR)$$
(4)
Standard error of odds ratio for log reporting;
$$\mathrmSE_\mathrmLnROR=\sqrt1/\mathrma+1/\mathrmb+1/\mathrmc+1/\mathrm d$$
(5)
95% confidence interval;
$$95\text\%CI = \left[ {\textexp\left( \textLnROR – 1.96 \times \textSE_\textLnROR \right),\textexp\left( {\textLnROR + 1.96 \times \textSE_{\textLnROR} } \right)} \right]$$
(6)
Leave a Reply