
Jordan Reed- I am not currently monitoring air pollution/quality in my area. I’ve been more aware of it lately because of the fires that have been happening in Canada. Seeing the enormous effect it has had not only on the land, but also in the air. It has spread all the way to my home state of Virginia. I think if you live somewhere where air quality is a concern, you should be aware of it and monitor it daily, especially if you have athletes participating in outdoor sports. Long-term effects can occur due to poor air quality and it is not ideal for people to regularly breathe outside. If the air quality is poor, as a future Athletic Trainer there must be other places where the team/individual can participate and/or practice. It is preferable to ensure that these areas are available and ready for use, as air quality can change quickly.
Blog
-

A deep learning system accurately identifies joint space narrowing and erosions on hand X-rays

New research at ACR Convergence 2023, the annual meeting of the American College of Rheumatology (ACR), shows that a deep learning system can accurately identify and predict joint space narrowing and erosions in hand x-rays of patients with rheumatoid arthritis (RA) (Abstract #0745) .
X-rays are the most commonly used imaging technique for detecting and monitoring RA in the hand. Radiologists often use the well-validated Sharp/van der Heidje (SvH) method to evaluate joint space narrowing and erosions by assessing specific locations in each hand and wrist. However, scoring SvH is time-consuming and requires expertise that is not always available. This has led to increased use of deep learning (also called machine learning) to analyze hand X-ray data in RA.
According to Carol Hitchon, MD, FRCPC, MSc, associate professor at the University of Manitoba and clinical scientist in rheumatology and lead co-author of the study: “Machine learning offers a powerful and complementary approach to traditional RA detection and diagnosis methods. It improves the accuracy, efficiency and objectivity of RA radiograph assessment, while providing the opportunity for early detection of damage and valuable insights into the disease.”
For the current study, Hitchon and colleagues aimed to develop and validate a deep learning system for the automated detection of joints and prediction of SvH scores on hand radiographs of patients with RA.
They used a convolutional neural network (CNN)-based algorithm called You Only Look Once (YOLO). CNN is a deep learning neural network commonly used in computer vision and recognition tasks and has been successfully used in medical image classification. YOLO is a type of CNN model specifically designed for real-time object detection in images and videos and known for its speed and efficiency in image processing. Hitchon and colleagues used a recent version of YOLOv516, which they showed to be more than 90% accurate in detecting hand joints.
The YOLO model was trained to detect joints in 240 training and evaluation pediatric hand radiographs from the Radiologic Society of North America database.
The researchers boxed and labeled the different joints of interest: proximal interphalangeal, metacarpophalangeal, wrist, distal radius, and distal ulna. The joint detection model was validated with 54 clinician-labeled radiographs from four adult RA patients followed for more than ten years.
Researchers then applied a vision transformer model (VTM) to predict the erosion and joint space narrowing score of each joint. Hitchon explains that a VTM is a deep learning architecture designed to efficiently process and understand sets of data.
It works by splitting an image into small chunks, transforming or flattening the chunks into a sequence, creating low-dimensional linear embeddings from the flattened spots, adding the positional embedding, and then running the encoded sequence into a standard transformer encoder for the remaining prediction task. ”
Carol Hitchon, MD, FRCPC, MSc, Associate Professor, University of Manitoba
The VTM was validated using more than 2,200 hand radiographs from 381 RA patients to whom the physician assigned SvH scores. Patients were from the Canadian Early Arthritis Cohort, a multicenter Canadian study. These scored radiographs were used as the gold standard for this study.
The joint detection model was trained to detect the entire wrist, but the researchers had SvH scores for individual wrist joints, so they trained a separate model to detect joint space narrowing and erosion in each joint.
When they evaluated the accuracy of their models, they found:
-
- The joint detection model accurately identified target joints. The F1 score for children was 0.991 and the F1 score for adults was 0.812. (In machine learning, the F1 score is a metric that measures the accuracy of a model).
-
- VTM predictions for joint space narrowing and erosion were very accurate. The principal square error, which evaluates the accuracy of predictions, was 0.91 and 0.93, respectively.
-
- The multitask models predicted SvH erosion and joint space narrowing scores of individual wrist joints with moderate accuracy (0.6 to 0.91).
Hitchon says they weren’t surprised by the performance of their model.
“The AI technologies we applied in this study have been successfully and widely used in other domains, some of which have been commercialized. Compared to the model’s performance in other domains, our performance is relatively low in predicting X-ray scores for some joint types, such as the wrist. [This] may be due to the relatively small sample size in our study or to the complexity of the anatomy of the wrist joint,” she notes.
Hitchon also says the model’s performance does not match that of human radiologists for joints such as the wrist.
“The AI models cannot replace human radiologists at this stage, but they will be excellent complementary tools that can improve the overall quality and efficiency of radiograph scoring analysis when used in conjunction with the radiologist’s judgment. [these models] may be applicable to the interpretation of large volumes of radiographs in clinical trials.”
The study has two major limitations: X-rays were obtained from cohorts composed almost entirely of white women, and the findings may not apply to races and ethnicities traditionally underrepresented in research studies. Hitchon acknowledges that the findings need to be replicated in other groups. The model also lacks the ability to learn and become more accurate with subsequent images, although Hitchon says they are developing a new deep learning framework so that the model continuously learns as new data is available.
This study received local funding from the Health Science Center Foundation, a hospital charity in Winnipeg, Manitoba, Canada. One of the co-authors, Pingzhao Hu, is supported by the Canada Research Chair Program. The Canadian Early Arthritis Cohort, which provided one set of radiographs, is funded by multiple sources.
Source:
American College of Rheumatology
-
-

Paragon 28 Announces New $150 Million Credit Facility to Replace Existing $90 Million Credit Facility
ENGLEWOOD, CO, November 7, 2023–(BUSINESS WIRE)–Paragon 28, Inc. (NYSE: FNA) (“Paragon 28” or “Company”), a leading medical device company focused exclusively on the foot and ankle orthopedic market, today announced that it has received a new $150 million credit facility from Ares Capital Corporation (“the Facility”) to replace the existing $90 million senior credit facility. The facility consists of up to $100 million in term loans, with $75 million drawn at closing, and a $50 million revolving credit facility, with $25 million drawn at closing. The facility has no dilutive effect without warrants or other equity-based instruments. The Company’s pro forma liquidity as of September 30, 2023 is $147.0 million, including $97.0 million of pro forma cash and $50 million of available borrowings under the facility.
“We expect continued improvements in our earnings and cash flow in 2024 and beyond, and the non-dilutive liquidity provided by Ares strengthens P28’s path to breakeven cash flow,” said Steve Deitsch, Chief Financial Officer.
“We are excited to partner with Paragon 28, a truly innovative and fast-growing company,” said Doug Dieter, partner at Ares’ Credit Group. “P28’s growth and leadership in the global foot and ankle market has been impressive, and we are pleased to support its continued mission to improve patient outcomes.”
Further details regarding the credit agreement are included in the Company’s Form 8-K filed with the U.S. Securities and Exchange Commission on November 7, 2023.
About Paragon 28, Inc.
Based in Englewood, Colo., Paragon 28 is a leading medical device company focused exclusively on the foot and ankle orthopedic market and committed to improving the lives of patients. Since its inception, Paragon 28® has provided innovative orthopedic solutions, procedural approaches and devices covering a wide range of foot and ankle conditions, including fracture fixation, forefoot, ankle, progressive collapsing foot deformity (PCFD) or flat foot, Charcot foot and orthobiological agents . The company designs products with both the patient and surgeon in mind, with the goals of improving outcomes, reducing recurrences of disease and complications, and making procedures simpler, more consistent and reproducible.
About Ares Management Corporation
Ares Management Corporation (NYSE: ARES) is a leading global alternative investment manager offering clients complementary primary and secondary investment solutions across the credit, private equity, real estate and infrastructure asset classes. We strive to provide flexible capital to support businesses and create value for our stakeholders and within our communities. By working with all our investment groups, we aim to generate consistent and attractive investment returns throughout market cycles. As of September 30, 2023, Ares Management Corporation’s global platform had approximately $395 billion in assets under management, with approximately 2,800 employees operating in North America, Europe, Asia Pacific and the Middle East. For more information, please visit www.aresmgmt.com.
Forward-Looking Statements
Except for the historical information contained herein, the matters set forth in this press release are forward-looking statements within the meaning of the “safe harbor” provisions of the Private Securities Litigation Reform Act of 1995, including, but not limited to to: Paragon 28’s potential to shape a better future for foot and ankle patients and estimated net revenues for the full year 2023. You are cautioned not to place undue reliance on these forward-looking statements. Forward-looking statements are only predictions based on our current expectations, estimates and assumptions, which speak only as of the date on which they are made, and are subject to risks and uncertainties, some of which we are not currently aware of. Forward-looking statements should not be read as a guarantee of future performance or results and may not necessarily be an accurate indication of the times at or at which such performance or results will be achieved. These forward-looking statements are based on Paragon 28’s current expectations and inherently involve significant risks and uncertainties. As a result of these risks and uncertainties, actual results and the timing of events may differ materially from those anticipated in such forward-looking statements. These risks and uncertainties are more fully described in the section entitled “Risk Factors” in Paragon 28’s filings with the Securities and Exchange Commission (the “SEC”), including Paragon 28’s Annual Report on Form 10-K filed on filed with the SEC on March 2. , 2023. Paragon 28 undertakes no obligation to update any forward-looking statements and expressly disclaims any obligation or undertaking to publicly release any updates or revisions to any forward-looking statements contained herein. These forward-looking statements should not be relied upon as representing the views of Paragon 28 as of any date subsequent to the date of this press release. Paragon 28’s results for the quarter ended September 30, 2023 are not necessarily indicative of our results of operations for future periods.
Contacts
Contact person for investors:
Matt Brinckman
Senior Vice President, Strategy and Investor Relations
mbrinckman@paragon28.com -

Influence of the 2000-meter ergometer test on indirect markers of intestinal injury in competitive elite rowers in different training phases BMC Sports sciences, medicine and rehabilitation
Attendees
Eighteen male members of the National Polish Rowing Team (heavyweight rowers) were recruited, but only 10 met the inclusion criteria and participated in the study; all participants completed the two ergometer tests of 2000 meters. Before each test, anthropometric parameters were assessed using an electronic scale to the nearest 0.05 kg (Tanita BC-980 MA, Tanita Corporation, Tokyo, Japan). The results are shown in Table 1. The study was conducted by following the Declaration of Helsinki. The study protocol was approved by the local ethics committee of Poznań University of Medical Sciences (decision No. 314/22 in 2022). All participants were informed of the study procedures and gave their written consent.
Table 1 The anthropometric characteristics of the participants (in the morning after an overnight fast before tests I and II). Inclusion criteria
The inclusion criteria were a minimum of 5 years of training, a minimum total training time of 240 minutes per week, membership of the Polish rowing team and completion of the 2000 meter ergometer test.
Exclusion criteria
The exclusion criteria were antibiotic therapy, probiotics, prebiotics, metformin, dietary regimen, and health problems in the past three months.
Training program
The exercise profile, including intensity, volume (in minutes), and type (specific, i.e., rowing: endurance, speed, technical; and nonspecific: strength, jogging), was recorded daily. In addition, the intensity of the training was classified based on the LA threshold (4 mmol/l): an extensive (below the LA threshold) or an intensive (above the LA threshold) workload (Table 2).
Table 2 Pre-test training program Food intake
Total food intake was analyzed by a dietitian before each test using the 24-hour dietary recall method. The dietitian carefully checked each questionnaire and was available to participants during all meals. Energy, carbohydrates, proteins and fats were then measured via the commercially available DietetykPro program (DietetykPro, Wrocław, Poland).
figure 1 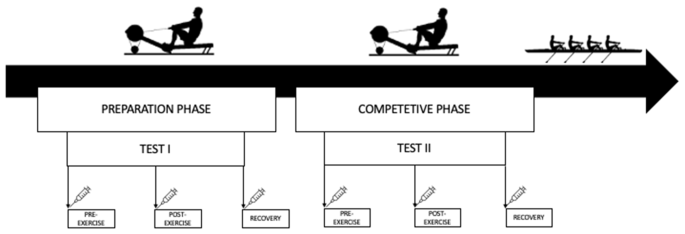
The research design and timeline
Exercise test
For tests I and II, the athletes performed a controlled test at a distance of 2000 m (Fig. 1). The break between tests was almost 10 weeks (68 days). Test I was conducted at the beginning of the preparatory phase, while Test II was conducted at the beginning of the competitive phase. The participants rowed a distance of 2000 m as quickly as possible on the ergometer (Concept II, USA), as the test results were taken into account when selecting for the champion team. The athletes were therefore highly motivated to perform both tests with maximum effort. The exercise test was performed every day at 10:00 am. Before the test, participants ate a small, light meal and were hydrated (Table 1). Before testing, each participant completed an individual 5-minute warm-up.
Collect and research material
Samples were collected at the same three time points: before (before training), after an overnight fast; Post (immediately after training) and recovery (after 1 hour of recovery) for tests I II.
Blood samples were collected from the antecubital vein into 9 ml polyethylene tubes (to obtain serum) and centrifuged at 3000 rpm for 10 minutes. The serum was frozen and stored at −80°C until analysis. In addition, capillary blood samples were collected from the earlobe before and immediately after the exercise test to assess LA levels.
Dimensions
Serum zonulin, intestinal fatty acid binding protein (I-FABP), LPS, LBP, and interleukin 6 (IL-6) were measured using commercially available enzyme-linked immunosorbent assays (ELISAs; SunRed Biotechnology Company, Shanghai, China). The test range was 0.25–70 ng/ml for zonulin, 0.3–80 ng/ml for I-FABP, 12–4000 endotoxin units (EU)/l for LPS, 0.2–60 µg/ml for LBP and 1–300 ng/l for IL-6. In addition, LA in capillary blood was measured immediately after sampling using a commercially available kit (Diaglobal, Berlin, Germany). The LA concentrations are presented as mmol/l.
static analysis
Statistical analysis was performed using GraphPad Prism 9 (GraphPad Software, USA). Descriptive statistics such as mean and standard deviation were used to identify patterns and trends. To investigate whether the variables had a normal distribution, the Shapiro-Wilk test was performed. To measure the equality of variances, the Brown-Forsythe test was used. One-way repeated measures analysis of variance (ANOVA), with Tukey’s post hoc analysis, was used to assess differences in measured variables from the three assessment points (Pre, Post, and Recovery) for Tests I and II. A t test was used to compare food intake, anthropometric characteristics and 2000-m test results (power, time and LA) between tests I and II. Cohen’s d was calculated to determine effect size. It was interpreted as small (0.2), moderate (0.5), or large (0.8) (Cohen, 1988). For correlation analysis, Pearson linear correlation coefficients were calculated. Significance of all statistical analyzes was set at p ≤ 0.05. Based on a power analysis, all tests that produced significant results had a power above 0.9, as calculated by G Power 3.1(G Power, (13).
-

Appointment of deputy general manager
Appointment of Sandrine Carle
as deputy general managerEcully, November 7, 2023-The Spineway Group, specialists in innovative implants for the treatment of serious spinal disorders, announces the appointment of Sandrine Carle as Deputy Chief Executive Officer. Ms. Carle joined Spineway in July 2022, at the time of the acquisition of Spine Innovations, where she was CEO. She was instrumental in the successful integration of Spine Innovations into the Spineway Group.
After obtaining a degree in biomedical engineering (UT Compiègne) and an Executive MBA at HEC in Paris, Sandrine Carle worked for more than 20 years in the orthopedic surgery sector, and more specifically in the spine surgery sector at Medtronic (Europe), Kyphon (USA) and Vexim (France). She held marketing and management positions in France and the US before being appointed CEO of Spine Innovations in 2020.
Ms. Carle led the creation of this entity following a spin-off in 20201 and the development of this activity between 2020 and 2022. She led the recruitment and management of about fifteen employees, set up the functional and operational organization of the team and also obtained the company’s certification from the notified body G-MED (France ).
Together with Stéphane Le Roux, CEO of Spineway, Sandrine Carle is responsible for executing the Group’s overall roadmap, in particular the business development plan aimed at returning to operational break-even,2 as well as all R&D projects (short, medium and long term).
Stéphane Le Roux said: “I am pleased that Sandrine is joining me as Deputy Chief Executive Officer of Spineway. I am confident that her leadership, strategic insight and deep market knowledge will help shape our future. She will strengthen our highly experienced management team. Sandrine will also lead the Group’s development plan as we remain committed to our core values of quality and innovation. She will work closely with me, our management team and all our employees to achieve our goal: to become an innovative player in France and internationally, a leader in less invasive spine treatments.”
Next event:
November 10, 2023: Extraordinary General MeetingSPINEWAY ELIGIBLE FOR PEA-SME (Small and Medium Business Equity Savings Plans)
Find out all about Spineway at www.spineway.comThis press release has been drawn up in both English and French. In case of contradictions, the French version shall prevail.
Spineway designs, produces and sells innovative implants and surgical instruments for the treatment of serious spinal conditions.
Spineway has an international network of more than 50 independent distributors and 90% of its turnover comes from exports.
Spineway, which is eligible for investment through FCPIs (French unit trusts specialized in innovation), has received the OSEO Excellence Award since 2011 and the Deloitte Fast 50 Award (2011). Rhône Alpes INPI Patent Innovation Award (2013) – INPI Talent Award (2015).
ISIN: FR001400BVK2 – ALSPWContacts:
SPINEWAY Shareholder services line
Available from Tuesday to Thursday
+33 (0)806 706 060
Suitable PEA/PME ALSPW
Euonext growth
HEAVEN Office & Communications
Relations with investors
Solène Kennis
Spineway@aelium.fr
1 Spine Innovations was a spin-off born in 2020 from the sale of Groupe FH Orthopedics (France) to the Spineway Group.
2 Positive operating result
-

Zimmer Biomet reports third quarter 2023 financial results
- Third quarter net sales of $1.754 billion increased 5.0% and 4.7% at constant exchange rates1 base
- Third quarter diluted earnings per share were $0.77; adjusted1 diluted earnings per share were $1.65
- The company updates reported 2023 revenue expectations due to currency expectations and reaffirms consistent 2023 foreign exchange revenue growth and adjusted1 financial guidelines for earnings per share
WARSAW, Ind., Nov. 7, 2023 /PRNewswire/ — Zimmer Biomet Holdings, Inc. (NYSE and SIX: ZBH) today reported financial results for the quarter ended September 30, 2023. The company reported third quarter net sales of $1.754 billion, up 5.0% from the same period last year, and an increase of 4.7% at constant exchange rates1 base. Net income for the third quarter was $162.7 million, or $346.5 million adjusted1 base.
Diluted earnings per share were $0.77 for the third quarter and were adjusted1 diluted earnings per share were $1.65.
1. Reconciliations of these measures to the corresponding US generally accepted accounting principles are included in this press release. “We are very pleased to report another Zimmer Biomet quarter of strong revenue growth and earnings per share. Our team continues to successfully drive execution and growth with a focus on innovation to create value for the stakeholders we serve,” said Ivan Tornos, President and Chief Executive Officer of Zimmer Biomet. “As the new CEO of ZB, I am more confident than ever in our team, our full-year expectations for 2023 and that our solid growth – both top and bottom line – will continue in 2024.”
Recent Highlights
In line with the ongoing transformation of Zimmer Biomet’s business, key recent highlights include:
- Appointment of Ivan Tornos as President and Chief Executive Officer and expansion of Chief Financial Officer Suketu (Suky) Upadhyay’s role to CFO and EVP, Finance, Operations & Supply Chain as part of Zimmer Biomet’s increased focus on innovation and commercial execution
- Major updates to the Zimmer Biomet Executive Leadership Team, including the promotion of Wilfred van Zuilen to Group President, EMEA and Mark Bezjak to President of the Americas, as well as the appointment of Chief Science, Technology and Innovation Officer Nitin Goyal, MD to the Executive Leadership team
- Registration of 100,000 patients since the launch of mymobility® care management platform, which provides a guided orthopedic patient experience, with automation, data and insights for physicians
- Continued recognition for our Environmental, Social and Governance (ESG) programs with inclusion on the Newsweek Americas Greenest Companies 2024 and Sustainability Magazine Top 10: Sustainable Healthcare Device Companies lists
Geographic and product category sales
The following sales tables provide results by geography and product category for the three- and nine-month periods ended September 30, 2023, as well as the percentage change compared to the applicable prior year period, both on a reported and constant currency basis.
SEE FINANCES HERE
-

Testing the athletic shoulder with Ben Ashworth
Standardized tests are often performed in the health and performance world to establish baselines, monitor performance, or help an athlete return to sports.
The lower extremity has received the most attention, but the ASH test, or athletic shoulder test, popularized by Ben Ashworth, is a great option for the upper extremity.
In this episode I talk to Ben about the ASH test and how to best use it for both rehabilitation and performance.
Special offer for Ben’s online courses

Plus, Ben was super friendly and gets a great discount on his new online courses on testing and training the athletic shoulder! Click the button below and make sure you use the coupon code REYNOLD at checkout!
https://mikereinold.com/athleticshoulder/
Show notes
Ben works as a consultant with teams and individuals to solve shoulder performance issues. He has over twenty years of experience as a practitioner with Masters degrees in both Physiotherapy and Strength & Conditioning.
Social tools for COS:
– Instagram: @athleticshoulder -

Research shows that depression increases the risk of disability in patients with rheumatoid arthritis
In a review published in Nature Reviews Rheumatologyresearchers discussed the interactions between central and peripheral immunobiological mechanisms associated with rheumatoid arthritis (RA) and major depressive disorder (MDD).
They further described the role of inflammatory proteins, the effect of peripheral inflammation on different parts of the brain, and the relationship between changes in the brain and inflammation-induced depression.
 Study: Immune mechanisms of depression in rheumatoid arthritis. Image credits: pikselstock/Shutterstock.com
Study: Immune mechanisms of depression in rheumatoid arthritis. Image credits: pikselstock/Shutterstock.comBackground
RA is a chronic autoimmune inflammatory disease that negatively affects synovial joints and several other organs. Depression is a common, clinically heterogeneous condition that affects all other patients with RA. There is increasing evidence that RA and depression have overlapping features and can be modulated by each other.
Data suggest that depression is a risk factor for RA, and that patients diagnosed with RA at a young age are more susceptible to depression. Furthermore, RA patients with depression are observed to exhibit functional progression as well as decreased response to treatment, leading to poor outcomes. However, the precise biological mechanisms underlying this association are not clearly understood.
Therefore, this review focuses on understanding the link between these two conditions and the underlying mechanisms, while exploring the interplay between the nervous system and the immune system in RA patients.
Shared cytokines in RA and depression
Proinflammatory cytokines amplified in RA are also known to be causally linked to depression. Several cytokines have been implicated in RA and depression, including interleukin (IL)-16, IL-18, IL-1, IL-6, and tumor necrosis factor (TNF).
Peripheral immune signals to the brain
The peripheral immune system signals the brain through two known pathways: neural and humoral. In the neural pathway, molecules that mediate inflammation can bind and activate receptors on sensory neurons, including those in the dorsal root ganglia (DRG) and the vagus nerve.
The activated sensory neurons then send the signal back to the cerebral cortex of the brain via the spinal cord. The signal is then passed on to higher brain centers, which modulate the immune system locally and systemically.
Through the humoral pathway, immune cells release molecules capable of crossing the blood-brain barrier (BBB) and affecting brain cells or activating the endothelial cells of BBB.
As observed in experimental studies in mice, this pathway leads to the release of chemokines involved in neuronal plasticity, resulting in depression-like behavior and cognitive impairment.
Immune responses in the brain
In the brain, existing neural cells and recruited immune cells release various inflammatory proteins that support neuroimmune communication. When cytokines and chemokines are released by neurons, microglia, astrocytes, peripheral immune cells and endothelial cells, they influence neurological and immunological processes.
For example, during inflammation, the recruitment of peripheral monocytes to the brain is associated with dendritic remodeling and cognitive impairment, potentially leading to depression. Chronic peripheral inflammation in RA induces local microglial activation in the brain, leading to altered microglial expression.
Although microglia are often associated with inflammatory changes in the brain, recent studies indicate a more complex role for microglia in neurological health.
Contrary to previous belief, microglia found in the brain, according to studies in mice, originate not only from peripheral blood, but also from meninges and bone marrow in the skull. However, there is a lack of studies examining this aspect in humans.
Astrocytes also play a role in brain inflammation. Activation of astrocytes by cytokines from microglia has been shown to result in the release of neurotoxic factors that influence neuronal health and behavior.
Mechanisms linking depression and inflammation
Immune-related inflammation has been implicated in the pathophysiology of depression. In RA, several pathways are activated, which can lead to inflammation-related behavior.
These pathways include inflammasome activation, the kynurenine pathway, neuroplasticity, and the pathways of the glutamatergic and serotonergic systems.
Regional variation in the brain
Although regional changes in the brain and the underlying mechanisms continue to be studied, mainly using animal models, neuroimaging studies in humans have significantly improved our understanding of inflammation-related changes in the brain.
Advances in magnetic resonance imaging (MRI) have provided insights into the role of inflammation in depression beyond traditional structural assessments and histology-based studies. Emerging evidence suggests that the brain regions affected by inflammation and depression are the striatum, hippocampus, amygdala, and insula.
Conclusion
This review article provides a comprehensive overview of the association between immune mechanisms and depression in patients with rheumatoid arthritis. It highlights the need for further research in this area.
Furthermore, data from clinical trials suggest that immune modulation may be a promising approach for treating comorbid depression in patients with rheumatoid arthritis, potentially reducing the global burden of this debilitating condition.
-

Sports managers need sports trainers for a better heat policy
Exercise-induced heat illness: policy adoption and influence on contextual factors reported by athletic administrators
Scarneo-Miller SE, Adams WM, Coleman KA, Lopez RM. Sports Health. Mar 5, 2023: 19417381231155107. doi: 10.1177/19417381231155107. E-publishing prior to printing. PMID: 36872595.
https://journals.sagepub.com/doi/10.1177/19417381231155107
Take home message
Most high school athletic administrators reported having a written heat illness policy in place, but they were often missing key components. The presence of an athletic trainer helped create a written policy that included more components.
Background
Sports administrators play an important role in policy acceptance. Policy measures such as addressing acute heat illness are critical as improper management can lead to poor outcomes. Unfortunately, we know little about the factors that promote and hinder the implementation of heat illness policies.
Study aim
The authors surveyed high school athletic administrators in the United States to describe the adoption of exertional heat illness policies and to examine factors that influence the adoption of these policies.
Methods
During the 2018-2019 academic school year, the research team emailed nearly 7,000 athletic administrators inviting them to complete a questionnaire asking about 1) demographics, 2) exercise-related illness policies, 3) monitoring and modification of written policy, and 4) enablers and barriers to policy development. The researchers used the precautionary adoption process model to assess an athletics administrator’s willingness to adopt policies. The adoption model is based on 8 phases, from not being aware to maintaining a written policy for more than 6 months.
Results
Of 466 athletics administrators (~48 years old, 82% male, 77% worked in the field for more than 15 years), 78% reported having a written policy on the prevention and treatment of exertional heat illness. Only 6% adopted all eleven essential elements of an exertional heat illness policy. Almost half of the managers indicated that they adopted fewer than 5 essential elements.
Older athletics administrators, those who had previously dealt with heat illness, or those with an athletic trainer on their staff were more likely to have a written policy. Additionally, state mandates and having a medical professional were the most commonly cited facilitators for adopting policies on exertional illness prevention and use of a rectal thermometer. Similarly, the most commonly reported barrier to comprehensive heat illness management was the lack of a full-time athletic trainer (11). Administrators also recognized budget constraints that limited the use of a cold water immersion pool (23%), and the top barriers to using a rectal thermometer were discomfort using the thermometer (32%), parent/guardian resistance (30 %), resistance from parents/guardians (30%). coaches (30%) and liability issues (27%).
Viewpoints
Nearly 80% of athletics administrators surveyed reported that they had a written policy on exertional heat illness. Few integrated or were aware of all the necessary components to meet best clinical practices. The authors found that access to athletic training services was associated with better adoption of exercise health policies. This finding is consistent with it being an athletic trainer who would implement such a policy. It’s worth recognizing that only 7% of administrators contacted completed the survey. Therefore, these results may not accurately reflect what is happening in high schools across the country. One possibility is that people more interested in policy or heat illness completed the survey. So these results may show us the best-case scenario for written policies (78%) that include all components (6%) – which is a worrying sign.
Clinical implications
Encouraging state mandates and schools to hire athletic trainers can ensure that there are written policies to address heat illness. Clinicians may also want to consider strategies to educate coaches and parents/guardians about the reasons for this policy, such as rectal thermometers and cold water plunge pools.
Questions for discussion
Are you having trouble adding rectal temperature to your exercise heat illness protocol? Do you communicate with your athletics administrator regarding the approval, implementation and annual review/practice of your emergency policy?
related posts
- Management of exertional heat stroke still leaves something to be desired
- A little more education about heat stroke due to exertion could go a long way
- Clinical Pearl: prevention and treatment of exertional heat stroke
- Tag us! What do coaches know about heat stroke during exertion and the role of the athletic trainer?
- Follow guidelines to prevent exertional heat illness? Let’s reconsider these guidelines
Written by Jane McDevitt
Reviewed by Jeffrey Driban
-
You Don’t Look Sick – Living with Rheumatoid Arthritis: HAWAII DAY 1
Well, my start to my trip to Hawaii definitely started with a bang. First I got up early and got to the airport well in time. I had a wonderful taxi driver who was very sweet and he took me and my luggage to the airport lobby and arranged a wheelchair for me. I was so early that I was ahead of the people pushing the wheelchairs to your gate. So I had to sit and wait for about half an hour for someone to push me to my gate.
Getting through TSA was a lesson in patience. Since I was in a wheelchair, I was wheeled to the front of the line, but then had to wait for a female TSA agent to check my trunk. My boot had to be taken off and put through the X-ray machine and then my sock had to be inspected. I offered to take off my sock and they can take it to the x-ray machine, but they refused and instead felt all over my foot. It seemed kind of stupid. That whole process took about another 45 minutes.
My flight was very nice. I sat next to two very nice women who both wore masks the entire time and we were super helpful when we landed. In Hawaii the plane lands right on the tarmac and you have to walk down a flight of stairs. The two women carried my backpack and medicine bag so I could hold on to the railing.
Once I had my luggage, I waited in a long line to get the shuttle to the rental car. When I got to the rental car, I went to the Fast Track thinking I would get my rental car, but unfortunately they claimed I didn’t have my fast track for this reservation. So I had to wait in a long line for him to pick up my rental car. Luckily there were some very nice people in line who held my seat while I sat down for a while. It was very hot and I stood for a long time.
Finally I get to the front of the line and pick up my rental car. I drove away happily and went to the supermarket to get food. I drove just 20 miles further and it was clear something was wrong with the car. Every time I drove over 60 miles per hour there was a chattering sound like someone was banging in the trunk. After stopping a few times to see if I could see what the problem was, I called roadside assistance. That was an incredibly useless call because the guy kept asking me where I was, but I just knew I was on a highway in the middle of nowhere in Hawaii. So I finally turned around and went back to the airport.
Once back at the car rental company at the airport, I saw the same service representative I had spoken to twice. I called him and told him what happened and he quickly brought my new car over.
When the car came by, I had some really nice people helping me with my bags and groceries. This time the car was great. I arrived at the hotel and the nice lady at the reception helped me with my bags and groceries.
To give you an idea, I landed at 11:30 AM and arrived at the hotel at 6:00 PM. It took 6.5 hours to get off the plane, pick up my luggage, go to the rental location, get car #1, then a grocery store and drive 20 miles and then drive back and get car #2 and then drive 2 hours to the hotel. It was a lot of standing. Let’s see how my feet feel tomorrow. Oh yeah, I was late for dinner, so I ate snacks.
See you tomorrow…
