In this study, YKL-40 serum levels are influenced by factors such as age, inflammation and diagnosis of autoimmune diseases (RA/MII)3. Currently, due to its participation in tissue remodeling and degradation, attempts have been made to use it as a biomarker in pro-inflammatory states and as an indicator of poor prognosis in inflammatory diseases.6.7. However, its usefulness is still controversial because its full biological effects are still unknown. Furthermore, the specific factors that promote its expression, as well as its interaction with the majority of cytokines and molecules involved in the development and establishment of autoimmune inflammatory diseases, are not well established.17.
YKL-40 serum levels have been reported to increase with age in various cardiovascular, metabolic and systemic inflammatory diseases3. Bojesen et al. found that serum levels of YKL-40 increased exponentially with aging. In subjects with two YKL-40 measurements ten years apart, the average increase in YKL-40 was 1.5 μg/l/year18. Regarding inflammatory diseases, increased serum levels of YKL-40 were reported in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis, which was hypothesized to play a role in promoting chemotaxis, tissue damage and vascular damage.19.
In RA it has been recognized as a potential candidate autoantigen. Furthermore, in these patients it is produced and secreted by monocytes differentiated into macrophages, articular chondrocytes, synovium, peripheral blood mononuclear cells (PBMCs), and endothelium.17,19,20. It has been proposed that the pathogenic mechanism of YKL-40 in RA initiates through its binding to the HLA-DR4 peptide-binding motif promoting mononuclear cell proliferation, and HLA-DM plays a key role in presenting YKL-40 to CD4+ T cells. Furthermore, antigen-presenting cells (APCs) present YKL-40 at early-stage RA sites, suggesting an association for YKL-40 in the pathogenesis of RA.20,21,22. On the other hand, differentiated DR4+ dendritic cells and macrophages are similar to APCs of synovial joints and have the potential to carry out MHC II presentation of YKL-40 epitopes, resulting in higher levels in synovial and serum.21,22. Although the pathogenic mechanism in RA has been elucidated, agents that promote YKL-40 expression in RA are still lacking. It has been associated with the development of chronic, destructive, relapsing arthritis due to its role in tissue remodeling and breakdown. . It is considered an effective marker in estimating RA disease activities and prognostic value, and may be a therapeutic target19.
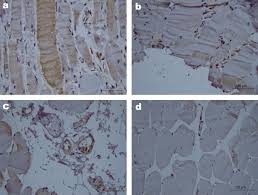
As for IIM, information is even more limited as few studies have been conducted in this regard and thus the role YKL-40 plays in this area has not yet been established. Regarding the pro-inflammatory effect and its relationship with the diagnosis and phenotype of IIM, Noguchi et al. found significantly increased serum in patients with PM/DM compared to the healthy population, as well as age-adjusted serum YKL-40 levels were significantly increased in patients with PM/DM compared to HC. In muscle biopsies, infiltration of YKL-40-positive inflammatory cells (probably macrophages) in the endomysium and perimysium was found. This suggests that cells other than CD8+ and CD4+ T cells can cause inflammation.23.
Ming-Zhu Gao et al. measured YKL-40 levels in patients with DM/PM and HI and reported significantly higher levels in patients with IIM compared to controls (51.6 vs. 27.8 ng/ml, respectively)6. In a systematic review by Cui et al. reports levels of 84.09 ng/ml in patients with PM and DM versus 27.37 ng/ml in HI24. On the other hand, Carboni et al. analyzed YKL-40 serum levels and its expression in muscle tissue in patients with ASSD. However, serum levels of YKL-40 did not correlate with other clinical, laboratory, disease status, or therapeutic parameters. Furthermore, YKL-40 was expressed by the inflammatory cells of the muscle tissue.13. Our study reinforces these results with serum levels of 187.80 ng/ml in patients with IIM versus 46.82 ng/ml in RA and 57.17 ng/ml in HI, as well as their presence mainly in inflammatory cells. This increase can be explained by inflammation, activation of macrophages, destruction of fibroblasts and existing vascular changes.
As previously mentioned, several biological effects of YKL-40 are known, such as inflammation and tissue remodeling, as well as its main sources, which, however, highlights its exacerbated expression in inflammatory diseases such as RA or SLE; some researchers have pointed out that this expression may vary depending on the disease type, which could be due to the multi-organ damage in IIM compared to RA, where the damage is mainly directed against the joints19.24. Tang et al. found that YKL-40 concentration was significantly higher in IIM patients with myocardial injury than without myocardial injury25.
In addition, YKL-40 plays a role in cardiovascular diseases such as early atherosclerosis, essential hypertension and other progressive vascular complications. In IIM patients, as in many other autoimmune diseases, serum levels of this protein have a positive association, particularly with atherosclerosis, and may predict both overall and cardiovascular mortality.5,26,27.
We wanted to know whether YKL-40 is affected by certain factors in IIM, as mentioned by Tizaoui et al. First, we compared some demographic, laboratory and clinical variables between patients with RA and IIM mentioned in Table 1. Of all After analyzing the variants, we found a significant difference in pDBP (P = 0.024) and pMBP (P = 0.035) which were higher in IIM patients. This may be due to the fact that blood vessels suffer damage in the early stages of the development of inflammatory diseases, altering blood pressure and increasing the risk of cardiovascular damage.28.29. Furthermore, the endothelial changes in IIM progress to microangiopathy, causing blood pressure changes12. Although information on exactly how the process occurs is scarce, it has been suggested that cardiovascular disease and cardiovascular risk increase mortality in IIM patients, but this is becoming controversial because a single center cross-sectional study recently reported that it risk of cardiovascular disease increases. factors in IIM patients are not significant compared to HI, but are significant in IIM if they are related to age, disease duration, duration of therapy and body composition, which could be related to our patients included in our study25.30. Although these evaluated variables were significant between these two groups, serum levels of YKL-40 were the most significant variable (P = 0.010). These were higher in IIM than in RA patients (187.80 ng/ml). vs 46.82 ng/ml, respectively).
Once we established that IIM exhibits higher serum levels of YKL-40 than RA, we examined whether serum levels of YKL-40 were influenced by age or disease duration. Our results show that only aging has a positive correlation with increased YKL-40, but not with disease duration. The reports conducted by Johansen in 2006 and Schultz 2010 have clearly shown that aging is predictive of the increase of YKL-40 in HI, but in our IIM patients the concentration of this protein is higher due to inflammation and damage to multiple organs.2.3.
We evaluated the predictive value of inflammatory state, age and diagnosis of IIM on serum levels of YKL-40 and clarified that CRP has predictive value on serum YKL-40 levels in IIM patients.P= 0.038) which corresponds to a cross-sectional survey and systematic review published by Cui andYou at the . In addition, age and the IIM diagnosis ( P=0.008AndP=0.001respectively) were found to be powerful predictors of YKL-40 serum levels24. On the other hand, we confirmed that age and IIM diagnosis have an important influence on YKL-40 concentration, because YKL-40 serum levels are the highest compared to control and RA groups, thus we know that the presence of the disease or its type influences the disease. the YKL-40 concentration. Some reports state that the YKL-40 concentration in HI is stable for many years, but increases with aging or inflammatory conditions. Other researchers reported that normal YKL-40 serum levels may be different among a healthy population. Therefore, they recommend establishing baseline values for each study, because in addition to environmental factors, genetic load is another variable that can influence the expression pattern. of this protein26. We previously mentioned the pathogenic mechanism by which YKL-40 expression is mediated in RA and its possible role in IIM, but the information is still insufficient.
Regarding the in situ analysis of YKL-40 muscle expression, we observed that YKL-40 is mainly expressed in inflammatory cells rather than in muscle cells. We also observed that YKL-40 expression is associated with higher CPK serum levels and MYOACT score which are often related. to higher inflammation and muscle weakness. This observation is in agreement with the unique previous report of YKL-40 in muscle tissue made by Carboni et al.13It thus supports its role in inflammation, as well as its function as a clinical marker for poor prognosis in inflammatory diseases.
Taking into account all our findings, we demonstrated the expression of YKL-40 in both HI and in patients with RA and IIM and the possible factors that could influence its expression.
WARSAW, Ind., November 6, 2023 (GLOBE NEWSWIRE) — Orthopediatrics Corp. (“OrthoPediatrics”) (NASDAQ: KIDS), a company solely focused on advancing the field of pediatric orthopedics, today announced that the company has entered into an exclusive distribution agreement with Montreal-based Ora Medical to market Ora’s gait trainer. Medical, The Levity, a device designed for children with mobility problems.
The Levity supports a child with an innovative partial weight bearing mechanism. This allows the child to interact with the world using his arms, unlocking countless possibilities. Thanks to the unique design, each child can receive personalized treatment. The Levity comes with versatile features to meet a wide range of needs: body weight support, harness, speed and direction of the device are adjustable, and the foldable design offers easy transportation. The Levity is suitable for most children between the ages of 3 and 12.
The Levity supports a child at the waist, allowing for a unique hands-free experience that strengthens the muscles most important for optimal walking rehabilitation. This opens up a whole new experience for children and therapists, as the latter can now fully concentrate on patient engagement.
Joe Hauser, president of Trauma and Deformity Correction at OrthoPediatrics, added: “Our new partnership with the team at Ora Medical is an exciting step in our non-surgical business. By partnering with great organizations with world-class technology, we can help more children with orthopedic conditions worldwide. The Levity running trainer will be a great addition to our portfolio of mobility solutions under the Specialty Bracing brand.”
Sarah Lambert, CEO and co-founder of Ora Medical, said: “As we begin to expand beyond Canadian borders, our partnership with OrthoPediatrics is perfectly timed. Their established market presence and expertise will facilitate the distribution of our device, furthering our mission to improve the mobility of children worldwide.”
About OrthoPediatrics Corp.
Founded in 2006, OrthoPediatrics is an orthopedic company focused exclusively on advancing the field of pediatric orthopedics. As such, it has developed the most comprehensive product offering for the pediatric orthopedic market to improve the lives of children with orthopedic conditions. OrthoPediatrics currently markets 53 products serving three of the largest categories within the pediatric orthopedic market. This product offering includes trauma and deformity, scoliosis and sports medicine/other procedures. OrthoPediatrics’ global sales organization focuses exclusively on pediatric orthopedics and distributes its products in the United States and more than 70 countries outside the United States. For more information, please visit www.orthopediatrics.com.
Contact person for investors
Philip Trip Taylor
Gilmartin Group
philip@gilmartinir.com
415-937-5406
In the current systematic review, we aimed to evaluate the impact of different triathlon events on the profile of cytokines (pro- and anti-inflammatory) and metabolic markers in triathletes. First, we verified the increase in pro-inflammatory cytokines including IL-1, IL-2, IL-6, IL-8, IL-12p40, INF-γ, MCP-1, TNF-α in PBMC, serum and plasma levels after different triathlon competitions. Second, in most studies we observed an increase in the production of anti-inflammatory cytokines (IL-4 and IL-10) at serum and plasma levels after the sprint, long-distance and Ironman races. Third, among metabolic factors, we observed an increase in the concentration of blood and plasma markers of muscle damage (CK, LDH and Myostatin), muscle fatigue (FFA and lactate), physiological stress (Cortisol) and inflammatory phase. (CRP) in athletes from different triathlon events.
Cytokines are signaling proteins produced by immune and non-immune cells that have cell signaling functions, positive and/or negative regulation of various genes and their transcription factors, and even stimulate or restrain inflammation promoted by various stimuli, including bacteria and viruses. [32, 33]. Alves et al. 2022, through a systematic review with meta-analysis, demonstrated that exposure to high running volume (exercise time, duration and distance covered) is associated with a higher concentration of pro-inflammatory cytokines, including IL-1β, IL-8 and TNF -α. Furthermore, serum levels of IL-1ra and IL-10 increased as a result of long-term aerobic exercise [6]. However, the authors only considered long-distance modalities (half marathon, marathon and ultramarathon), with the exception of triathlon. Similarly, from the data in the current systematic table it was concluded that several triathlon races promoted an increase in PMBC, serum or plasma concentration of pro-inflammatory cytokines. [6, 9].
High concentrations of pro-inflammatory cytokines are observed at the end of triathlon races and can be explained by the volume of the race, including the intensity of the exercise. In contrast, they had no association with the triathlon distance. This result confirms studies on endurance athletes. Studies have observed leukocytosis and high serum levels of pro-inflammatory cytokines after marathon races [34,35,36]. The metabolic activity and damage observed in muscle cells as a result of long-distance races, such as triathlon, appear to serve as important catalysts for the migration of some leukocytes, along with the release of cytokines. In addition, there are neuroendocrinological and metabolic multifactorial mechanisms that involve extreme stimuli and underlying consequences. Strenuous physical exertion such as triathlon increases immunosuppression [9, 37, 38]. The possible relationship between exercise and UTRI can be explained and modeled by a “J” curve, which can occur during competitions as well as during training, usually caused by rhinovirus, adenovirus and parainfluenza virus [19, 39, 40]. Furthermore, this profile of disease involvement may affect health and performance-related physical fitness components such as maximum oxygen volume, respiratory coefficient, and lactate threshold. [35, 36].
The anti-inflammatory response was assessed by serum levels of IL10 and IL4. Studies have shown that strenuous exercise can increase IL-10 levels, allowing it to return to basal levels during the rest period [41]. Furthermore, Santos et al. (2019) have shown that the magnitude of plasma IL-10 increases is related to the duration of exercise [42]. Furthermore, there is evidence that increases in serum levels of IL-10 are correlated with low levels of chronic, low-grade inflammation and tissue health. [7]. Huang et al. An increase in plasma IL-4 was found in 2019. Nevertheless, Suzuki et al., 2006 did not see any difference between serum levels before and after IL-4. According to our findings, there is no significant improvement in IL-4 due to the different aerobic exercise protocols [43]. Furthermore, the low serum IL-4 levels observed at the end of triathlon races can be explained by the strong inhibitory effects of IL-10 and IL-6 observed after long-distance triathlon races. These jointly contribute to the prevention of excessive systemic inflammation [44].
Long-term training protocols such as triathlons are known to cause changes in other biomarkers (gene expression and protein levels) [40]. A significant expansion of EGF and VEGF levels in many hematopoietic, endothelial and smooth muscle cells of the vasculature towards epithelial cells was observed. [40]. Furthermore, evidence has shown that aerobic exercise should activate the production and release of EGF and VEGF due to physiological adaptation to exercise, such as angiogenesis, indicating that EGF and VEGF are important biomarkers of aerobic exercise. [45]. At the same time, the studies noted that plasma CK levels increased after the race. As observed in a randomized double-blind crossover study by Galan et al. In 2018, CK serum levels improved after treadmill running to exhaustion [46].
Furthermore, Danielsson et al., 2017 reported an increase in CK levels after an Ironman distance triathlon, which is associated with masculinity [8]. Subsequently, it was known to improve FFA and LDH levels in sprint, Ironman and long-distance triathlons. Finally, cortisol levels were increased during triathlon protocols. It is known that the physiological demands of long-distance running such as triathlon should cause an increase in FFA, LDH, cortisol and lactate levels due to adaptation to the extensive energy expenditure of long-distance training protocols. [47,48,49]. Finally, according to previous evidence, an increased Myostatin level was reported in the aftermath of the Sprint and Iron Man Triathlon. Ben-Zaken et al., 2017 found that Myostatin expression was associated with a favorable outcome in long-distance running performance [50].
Because chronic systemic inflammation can be considered a factor affecting the performance of triathlon athletes, recommendations for managing the pillars of improving physical capacity (nutrient availability, sleep behavior, strength training) are important to modulate the immune response. In addition, it reduces both physical and physiological problems and accelerates the recovery and rehabilitation process after injuries. In this regard, individuals who practice triathlon can benefit from the immunomodulatory effects of a strength training strategy in combination with training for the sport. [51, 52]. Furthermore, adequate nutrient availability is known to benefit immune function, including cell-mediated immunity and a balanced inflammatory response. Finally, studies have shown that good sleep behaviors could be a complementary approach to reducing chronic inflammation [53, 54].
Strengths and limitations
The current systematic review presents important limitations that should be taken into account when generalizing the findings. First, we considered different distances of the triathlon race, which means that the generalization of the findings must be specific. The limitations of this systematic review mainly related to the methods of the studies. For example, the lack of control over the covariates (such as age, nutritional status, sleep quality, etc.) may be an important source of bias among the included studies. Another important point is the characteristics of the recorded sample. Because we only described gender and distance of participation, additional information such as level of competition and training characteristics may be useful in future research.
Therefore, the heterogeneity in the quality of reference sources is the strength of this review, as it observed efforts of serum levels of the inflammatory cytokine, as well as biomarkers associated with performance in different triathlon races. On the other hand, it must be emphasized that the studies did not randomize their populations, a procedure recognized by PRISMA. Some studies have not examined all outcomes considered relevant in this scenario. However, we find our work equally relevant because it systematically summarizes the available evidence for future research.
Dr. Hartl is the Hansen-MacDonald Professor of Neurological Surgery and director of Spinal Surgery at the Weill Cornell Brain and Spine Center in New York, and co-director of New York-Presbyterian Och Spine.
Dr. Hartl becomes Aclarion’s 2NL KOL to gain access to an MRI center authorized to perform Nociscans, adding NYC to Denver as the second active KOL location.
Aclarion will report on year-to-date Nociscan volumes before year-end and add this key metric to quarterly reporting starting in 2024.
BROOMFIELD, CO, November 6, 2023 (GLOBE NEWSWIRE) – via NewMediaWire — Aclarion, Inc., (“Aclarion” or the “Company”) (Nasdaq: ACON, ACONW), a healthcare technology company that uses biomarkers and proprietary enhanced intelligence algorithms to help physicians identify the location of chronic low back pain, today announced that Roger Hartl, MD, Hansen-MacDonald Professor of Neurological Surgery and director of Spinal Surgery at Weill Cornell Brain and Spine Center in New York, as well as New York-Presbyterian co-director Och Spine, will advise the company nationally as a key thought leader (KOL).
The practice of Dr. Hartl emphasizes an interdisciplinary approach to disease processes, and he works very closely with other specialists to personalize patients’ treatments. “My clinical interests focus on simple and complex spine surgery for degenerative conditions, as well as biological approaches for intervertebral disc repair and regeneration,” said Dr. Hartl. “Aclarion’s technology addresses a major gap in the current diagnosis of discogenic low back pain. I expect that Nociscan will provide valuable, objective information for our interdisciplinary approach to the treatment of degenerative intervertebral discs. Furthermore, I believe Nociscan will be equally valuable in our efforts to better understand less invasive surgical and biological treatment strategies for degenerative diseases of the spine.”
Chronic low back pain (cLBP) is a leading cause of opioid addiction in the US and the most expensive diagnosis in the United States. Aclarion’s Nociscan solution is the first science-based SaaS platform that helps physicians non-invasively distinguish between painful and non-painful intervertebral discs in the lumbar spine. Nociscan objectively quantifies chemical biomarkers shown to be associated with disc pain. Biomarker data is fed into proprietary algorithms to indicate whether a disc may be a source of pain. When combined with other diagnostic tools, Nociscan provides critical insights into the location of a patient’s low back pain, giving clinicians clarity to optimize treatment strategies.
“Dr. Hartl is a world-renowned neurosurgeon who continues to make advances in the diagnosis and treatment of low back pain,” said Brent Ness, CEO of Aclarion. “With immediate access to a Nociscan-activated MRI on Park Avenue in New York City, Dr. Hartl is already using Nociscan and will continue to gain clinical insights into the condition of his patients well into the future.”
Over the past 18 months, Aclarion has built a leading consortium of 10 KOL surgeons. Dr. Hartl represents the 10e and latest KOL addition to Aclarion’s panel. The company is now in the critical phase of activating MRIs for each of its KOLs so they can begin using the technology, track clinical outcomes, and advocate for payer coverage decisions to expand access to Nociscan for all expand patients. The company will announce additional MRI activations for the remaining KOLs as they become available and will begin reporting on scan volumes as Nociscan usage increases with these MRI activations.
For information about using Nociscan in New York City, please contact Aclarion at info@aclarion.com.
About Aclarion, Inc.
Aclarion is a healthcare technology company that uses magnetic resonance spectroscopy (“MRS”), proprietary signal processing techniques, biomarkers and enhanced intelligence algorithms to optimize clinical treatments. The company is entering the chronic low back pain market for the first time with Nociscan, the first evidence-based SaaS platform that helps physicians non-invasively distinguish between painful and non-painful discs in the lumbar spine. Through a cloud connection, Nociscan receives magnetic resonance spectroscopy (MRS) data from an MRI machine for each lumbar disc being evaluated. In the cloud, proprietary signal processing techniques extract and quantify chemical biomarkers shown to be associated with disc pain. Biomarker data is fed into proprietary algorithms to indicate whether a disc may be a source of pain. When combined with other diagnostic tools, Nociscan provides critical insights into the location of a patient’s low back pain, giving clinicians clarity to optimize treatment strategies. For more information please visit www.aclarion.com.
Forward-Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934 about the Company’s current expectations about future results, performance, prospects and opportunities. Statements that are not historical facts, such as “anticipates,” “believes” and “expects” or similar expressions, are forward-looking statements. These forward-looking statements are based on management’s current plans and expectations and are subject to a number of uncertainties and risks that could materially affect the company’s current plans and expectations, as well as its future results of operations and financial condition. These and other risks and uncertainties are discussed in more detail in our filings with the Securities and Exchange Commission. Readers are encouraged to read the section entitled “Risk Factors” in the Company’s April 21, 2022 Prospectus as filed with the Securities and Exchange Commission on April 25, 2022 under Rule 424(b)(4), as well as other disclosures. included in the Prospectus and subsequent filings with the Securities and Exchange Commission. Forward-looking statements in this announcement are made as of this date and the Company undertakes no obligation to publicly update or revise any forward-looking statements, whether as a result of new information, future events or otherwise.
Investor contacts:
Kirin M. Smith
PCG Advice, Inc.
646.823.8656 ksmith@pcgadvisory.com
Media contacts:
Jodi Lamberti
SPRIG advice
612.812.7477 jodi@sprigconsulting.com
Partnering with a therapist-owned physical therapy practice will improve patient care in Arizona
PHOENIX, AZ / ACCESS WIRE / November 6, 2023 / Foothills Sports Medicine Physical Therapy (Foothills PT) is proud to announce its newest addition with Camelback Sports Therapy, a therapist-owned physical therapy practice based in Phoenix, Arizona. With a combined experience of more than 40 years in the Valley, these two companies have an exciting opportunity to continue to provide comprehensive care to patients and expand their reach across a larger region
“We have been looking for a reputable business partner who can help us continue this growth trajectory, and we couldn’t be more excited to partner with Foothills PT,” said Natalie Semon, PT, MPT, CSCS, Cert. DN, CKTP, CEO of Camelback Sports Therapy. “Their established practice, with a reputation for superior customer service and quality care, is a perfect fit for us. We look forward to what our new collaboration will bring us!”
Patients with Camelback Sports Therapy will continue to receive the same high-quality care from the same familiar faces they know and trust. However, the clinical team will now have access to Foothills PT’s parent company, Confluent Health, and their established ecosystem of management services, as well as education and musculoskeletal healthcare resources. Support services include efficient community outreach, digital innovations, value-based care pathway models, and marketing and financial tools. Resources include best-in-class partnerships in physical therapy, such as the PTPN Network, continuing education programs and workforce development opportunities with Evidence in Motion, a nationally recognized training provider in residency, fellowship and certification in physical therapy and occupational therapy programs, and Fit For Work, the leading provider of worker safety.
“Since we opened our doors, our vision has been to provide the highest level of service to our patients and referring physicians at all of our clinics and throughout the state of Arizona,” said Mike Basten, PT, DPT, MTC, CEO of Foothills P.T. “We are pleased that this partnership will allow us to continue this vision and reach more residents than before.”
This partnership will further expand Foothills PT’s footprint, making it the proud owner of 41 clinics throughout Arizona. Dr. Kristi Henderson, DNP, FAAN and CEO of Confluent Health, stated, “We are extremely proud of our partnership with Foothills PT and welcome Camelback Sports Therapy to the Confluent Health family. The expertise and excellence this practice embodies will undoubtedly enhance our growth trajectory, unlocking countless opportunities for optimizing patient care.”
For more information about Foothills PT, visit their website at foothillsrehab.com. To schedule an appointment with one of Camelback Sports Therapy’s expert therapists, visit their website at camelbacksportstherapy.com or call 602-808-8989.
Rheumatoid arthritis is an inflammatory disease that can cause severe pain and swelling of the joints. But a new exercise intervention could help improve physical function and quality of life in people struggling with this debilitating condition.
In a new trial, researchers from the University of South Australia are working with Arthritis SA to investigate the potential of Blood Flow Restriction (BFR) training to improve the strength and mobility of people with rheumatoid arthritis.
BFR training is an exercise technique in which people wear pressurized bands – much like blood pressure cuffs – to slow blood flow to the muscles while they exercise. The cuff allows blood flow to the limb but slows its outflow, developing muscle strength without the need for heavy weights.
In Australia, rheumatoid arthritis is the second most common form of arthritis, affecting more than 450,000 people. More than 18 million people worldwide live with a condition. Women are two to three times more likely to develop rheumatoid arthritis than men.
Sports scientist Dr. UniSA’s Hunter Bennett says the research hopes to identify interventions that can improve the quality of life for people with rheumatoid arthritis.
“Rheumatoid arthritis can be a particularly debilitating disease. It is caused by the immune system attacking healthy tissues, leading to pain and swelling, joint destruction and loss of muscle mass and strength,” says Dr. Bennett.
Although medications can reduce symptoms, they do not address the loss of muscle strength and function.
The best way to increase strength and combat muscle loss is through resistance training, but this is often problematic for people with rheumatoid arthritis due to pain, fatigue or risk of injury.
Blood flow restriction training (BFR) offers an alternative. BRF is used in many sports and rehabilitation settings in Australia and is considered a safe and effective method for improving strength and function in many clinical populations, including people with osteoarthritis.
Because this technique uses very low loads, it is a viable option for people with rheumatoid arthritis. So in our research we look at how BRF can increase people’s strength and hopefully increase their freedom of movement and overall well-being.”
Dr. Hunter Bennett, exercise scientist, UniSA
The research team is currently seeking expressions of interest from women and men aged 45 to 75 years diagnosed with rheumatoid arthritis.
Exercise intervention eases pain for people with rheumatoid arthritis
We will be discussing meniscus tears, their function, and why surgery might not be the best option. The meniscus is a fibrocartilaginous structure located between the femur and tibia in the knee joint. There are two menisci in each knee, the medial meniscus, and the lateral meniscus. They function to provide shock absorption, force transmission, and stability to the knee joint.
https://youtu.be/hJ_NPyEJfBI?si=FAzhgmeK2iS6EELK
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears have a distinct mechanism of injury, while non-traumatic tears occur secondary to age-related changes. Meniscus tears are often classified according to location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Surgery to repair or remove the meniscus was performed in the past to reduce symptoms of pain and mechanical symptoms, such as clicking, catching, and locking of the knee. However, the current scientific literature does not fully support this theory.
If you suspect you have a meniscus tear, it’s important to see a doctor for an accurate diagnosis and appropriate treatment.
Key Takeaways
Mechanical symptoms are not a reliable indicator of the presence of meniscal tears.
Meniscus tears are common in asymptomatic individuals.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions.
Understanding Meniscus Tears
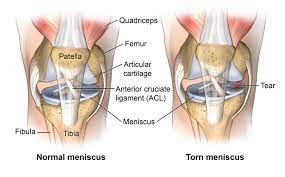
We want to provide you with a comprehensive understanding of meniscus tears. The meniscus is a fibrocartilaginous structure located between the femur and tibia bones in the knee joint. There are two menisci in each knee, the medial meniscus located on the inner portion of the knee and the lateral meniscus located on the outer portion. The menisci function to provide shock absorption, force transmission, and stability to the knee joint.
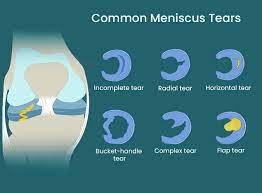
Meniscus tears are either traumatic or non-traumatic. Traumatic tears occur due to a distinct mechanism of injury, whereas non-traumatic tears occur secondary to age-related changes. Meniscus tears are often classified according to location and orientation, including vertical, longitudinal, radial, horizontal, oblique, or complex tears. Vertical or oblique tears that twist and fold over within the joint are termed bucket handle tears.
In the past, the presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. However, current scientific literature does not fully support this theory. Researchers have found that mechanical symptoms are equally prevalent in patients with and without a meniscal tear and are common in those with knee problems in general. Therefore, these symptoms have limited utility as an indicator for the presence of meniscal tears or are not useful clues to the diagnosis.
Meniscus tears are common in asymptomatic individuals. One study found that in 230 uninjured knees, 30 percent had meniscal tears. If tears are prevalent in a non-painful population, it brings into question the efficacy of surgery in reducing symptoms. Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, a brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain function and quality of life compared to placebo surgery.
At this moment, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears. Exercise has been shown to be just as effective in the long term for both populations. We have one study that showed exercise led to similar improvements in pain function and quality of life after 12 months in a younger population with mostly traumatic tears and another study that showed no clinically relevant difference in the function after two years in an older population with degenerative tears.
We want to provide you with a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category. The first category is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. You should aim to restore extension and flexion that is equal to your uninjured side. We recommend three options for knee extension or straightening and three options for knee flexion or bending.
The second category is hip, knee, and ankle strength. We recommend a four-step split squat progression, which will help increase your tolerance to weight-bearing knee flexion in deeper positions. We also recommend a single-leg knee extension and hamstring sliders to work on quadriceps and hamstring strength.
In conclusion, meniscus tears are a common knee injury that can be managed conservatively through exercise. Surgery has not been shown to provide better outcomes compared to other interventions. Our comprehensive rehab program covers multiple categories aimed at increasing your capacity and tolerance to various stressors. We recommend following this program for non-surgical cases. Always talk to your doctor or physical therapist before starting any exercise program.
Myths About Meniscus Tears
We often hear that meniscus tears are the cause of knee pain and mechanical symptoms such as clicking, catching, and locking of the knee. However, recent scientific literature does not fully support this theory. Here are three things you should know about meniscus tears:
There is not a simple cause and effect relationship between symptoms and tears. Patients with and without a meniscal tear have been found to have the same mechanical symptoms, which are actually common in those with knee problems in general.
Meniscus tears are common in asymptomatic individuals. In one study, 30% of uninjured knees had meniscal tears, which brings into question the efficacy of surgery in reducing symptoms.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, surgery can even lead to an increased risk of developing radiographic knee osteoarthritis.
Given this information, conservative management is favored for those with degenerative meniscus tears. Exercise has been shown to be just as effective in the long term for both younger patients with traumatic tears and older patients with degenerative tears.
We provide a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In the knee range of motion category, we recommend exercises such as seated active quad contractions, propping your heel up on an elevated surface, and banded tke. In the hip, knee, and ankle strength category, we recommend exercises such as the four-step split squat progression and single leg knee extensions for the quadriceps, and standing knee flexion with an ankle weight or hamstring sliders for the hamstrings.
It is important to note that these exercises are intended for non-surgical cases. If you had surgery, you should talk to your doctor or physical therapist before starting any exercise program.
Research on Meniscus Tears
The meniscus is a fibrocartilaginous structure that is located between the femur and tibia in the knee joint. There are two menisci in each knee, the medial and lateral meniscus. They provide shock absorption, force transmission, and stability to the knee joint.
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears occur due to a distinct mechanism of injury, while non-traumatic tears occur secondary to age-related changes. Tears can be classified according to their location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Bucket handle tears are vertical or oblique tears that twist and fold over within the joint.
In the past, the presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. Therefore, surgery to repair or remove the meniscus was performed to reduce symptoms. However, current scientific literature does not fully support this theory.
There is not a simple cause and effect relationship between symptoms and tears. Mechanical symptoms are equally prevalent in patients with and without a meniscal tear, and are actually common in those with knee problems in general. Meniscus tears are also common in asymptomatic individuals, with one study finding that 30 percent of uninjured knees had meniscal tears.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. A popular study compared a partial meniscectomy to a placebo or sham surgery and found that surgery provided no more benefit for knee symptoms or function than placebo surgery. It even led to an increased risk of developing radiographic knee osteoarthritis. A brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery.
Exercise has been shown to be just as effective in the long term for both younger and older populations with meniscus tears. Clinical practice guidelines favor conservative management in those with degenerative meniscus tears.
We provide a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. The program includes knee range of motion exercises, hip, knee, and ankle strength exercises, balance and proprioception exercises, and cardiovascular exercise.
Surgical Interventions
We have learned that surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, a recent Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery. Therefore, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears.
https://youtu.be/v4lpu0AYxU4?si=L5AVX1pr0upKPySV
Instead, we recommend a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. We will provide multiple exercise options within each category, ultimately giving you two different workouts to follow. These exercises are intended for non-surgical cases. If you had surgery, you should talk to your doctor or physical therapist before starting, as you may have weight-bearing precautions or other considerations to consider.
The first category is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side. For knee extension or straightening, we recommend seated active quad contractions, propping your heel up on an elevated surface, and banded tke. For knee flexion or bending, we recommend using a stationary bike, heel slides, and quadruped rock backs or tall kneeling rock backs.
The second category is hip, knee, and ankle strength. For quadriceps, we recommend a four-step split squat progression and a single-leg knee extension. For hamstrings, we recommend standing knee flexion with an ankle weight, machines, or hamstring sliders.
By following these exercises, you can increase your tolerance to weight-bearing knee flexion in deeper positions and improve your knee symptoms related to a degenerative meniscus tear.
Non-Surgical Interventions
We understand that meniscus tears can cause pain and other mechanical symptoms in the knee joint. However, surgery may not always be the best option for treating this condition. In fact, current scientific literature does not fully support the idea that surgery to repair or remove the meniscus leads to better outcomes compared to other interventions.
Therefore, we recommend a comprehensive rehab program that includes exercise progressions with sets and reps. This program aims to increase your capacity and tolerance to various stressors within each category. We have categorized the exercises into two main categories:
Category One: Knee Range of Motion
The first category focuses on restoring knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. If not, you should aim to restore extension and flexion that is equal to your uninjured side.
Here are three exercises that can help with knee extension:
Seated Active Quad Contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot to intensify the stretch.
Heel Prop: Prop your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration.
Banded TKE: Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion, here are three exercises that can help:
Stationary Bike: Start with the seat at a higher level, and as your range of motion improves, lower the seat to expose the knee to more flexion.
Heel Slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, at least three times a day, every day.
Quadruped Rock Backs or Tall Kneeling Rock Backs: Kneel on a pad or pillow for these exercises. You can even experiment with using a towel behind the knee, which can help patients move into more knee flexion with less discomfort.
Category Two: Hip, Knee, and Ankle Strength
The second category focuses on hip, knee, and ankle strength. We recommend a four-step split squat progression that will help increase your tolerance to weight-bearing knee flexion in deeper positions.
Here are the four levels of the split squat progression:
Body Weight Squat: Perform three sets of 20 repetitions, getting your hips to at least parallel. If you need to, start with hand assistance, such as using a TRX or another object.
Heels Elevated Squat: Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Perform three sets of 20 repetitions, and again, try to get your hips to at least parallel.
Split Squat: Stand in a split stance and lower down while driving the front knee forward as far as you can. Perform three sets of 15 controlled reps on each leg before progressing.
Front Foot Elevated Split Squat: Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the hamstrings, we recommend standing knee flexion with an ankle weight, using machines, or performing hamstring sliders. Start with double-leg eccentric sliders for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity, but to start, you can shorten the range of motion or even perform with no weight if needed.
In conclusion, exercise has been shown to be just as effective in the long term for treating meniscus tears compared to surgery. Therefore, we recommend a comprehensive rehab program that includes these exercises to help you recover from this condition.
Exercise as a Treatment Option
We have seen that surgery for meniscus tears may not be the best option, and that exercise can be just as effective in the long term for both younger and older populations. Therefore, we present a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category.
Knee Range of Motion
The first category we will cover is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, we recommend three options. The first is seated active quad contractions, where you straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot in order to intensify the stretch.
Another option is propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
Finally, once you gain more range of motion, strength, and control, add in a banded tke. Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend three options. You can use a stationary bike and start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion. Another option is heel slides. You can use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, so at least three times a day, every day.
Finally, a more advanced option is quadruped rock backs or tall kneeling rock backs. We recommend kneeling on a pad or pillow for these, and you can even experiment with using a towel behind the knee. Anecdotally, we have found this to help patients move into more knee flexion with less discomfort.
Hip, Knee, and Ankle Strength
The second category we will cover is hip, knee, and ankle strength. Let’s start with a four-step split squat progression, which will help increase your tolerance to weight bearing knee flexion in deeper positions.
Level 1 is a bodyweight squat. Your goal is to perform three sets of 20 repetitions, getting your hips to at least parallel. If you need, start with hand assistance such as using a TRX or another object.
Level 2 is a heels elevated squat. Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Your goal is three sets of 20 repetitions, and again, try to get your hips to at least parallel.
Level 3 is a split squat. Stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
Level 4 is a front foot elevated split squat. Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the quadriceps, we recommend a single leg knee extension for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity, but to start, you can shorten the range of motion or even perform with no weight if needed.
For the hamstrings, the first option will emphasize knee flexion. You can perform standing knee flexion with an ankle weight, use machines, or an exercise we like to use called hamstring sliders. Start with double leg eccentric sliders before progressing to single leg eccentric sliders.
We hope this comprehensive rehab program will help you increase your capacity and tolerance to various stressors, ultimately leading to better knee function and quality of life.
Rehab Program
We will now discuss a comprehensive rehab program for meniscus tears, which includes exercise progressions with sets and reps. The meniscus is a fibrocartilaginous structure located between the femur and tibia bones in the knee joint. There are two menisci in each knee, the medial meniscus on the inner portion and the lateral meniscus on the outer portion. The menisci provide shock absorption, force transmission, and stability to the knee joint.
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears occur due to a specific injury, while non-traumatic tears occur due to age-related changes. Tears can be classified according to location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Vertical or oblique tears that twist and fold over within the joint are termed bucket handle tears.
In the past, pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. Therefore, surgery to repair or remove the meniscus was performed to reduce symptoms. However, current scientific literature does not fully support this theory.
There is not a simple cause and effect relationship between symptoms and tears. For example, a 2018 study found that mechanical symptoms were equally prevalent in patients with and without a meniscal tear and are actually common in those with knee problems in general. Other research has concluded that these symptoms have limited utility as an indicator for the presence of meniscal tears or are not useful clues to the diagnosis.
Meniscus tears are common in asymptomatic individuals. In one study, researchers found that in 230 uninjured knees, 30 percent had meniscal tears. If tears are prevalent in a non-painful population, it questions the efficacy of surgery in reducing symptoms.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. For example, a popular study compared a partial meniscectomy to a placebo or sham surgery over the course of five years. Surgery provided no more benefit for knee symptoms or function than placebo surgery. It even led to an increased risk of developing radiographic knee osteoarthritis. In fact, a brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery.
Exercise has been shown to be just as effective in the long term for both populations. One study showed exercise led to similar improvements in pain, function, and quality of life after 12 months in a younger population with mostly traumatic tears. Another study showed no clinically relevant difference in function after two years in an older population with degenerative tears.
Therefore, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears. We will now present a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category. We will provide multiple exercise options, ultimately giving you two different workouts to follow.
Before diving into these exercises, there is one caveat we want to mention. These exercises are intended for non-surgical cases. If you had surgery, you will ultimately follow a similar framework, but before starting, talk to your doctor or physical therapist as you may have weight-bearing precautions or other considerations to consider.
Category One: Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At a minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, here are three options:
Seated active quad contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot to intensify the stretch.
Propping your heel up on an elevated surface: Elevate your heel on a surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
Banded TKE: Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, here are three options:
Stationary bike: Start with the seat at a higher level and lower it as range of motion improves to expose the knee to more flexion.
Heel slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions.
Knee Range of Motion Exercises
We will now discuss knee range of motion exercises that are essential for rehabilitating meniscus tears. The meniscus is a vital structure that provides shock absorption, force transmission, and stability to the knee joint. Meniscus tears can be traumatic or non-traumatic and can be classified based on their location and orientation. The presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were traditionally thought to be caused by a meniscus tear. However, surgery to repair or remove the meniscus has not been shown to lead to better outcomes compared to other interventions.
Therefore, we recommend a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In the first category, we will focus on knee range of motion exercises. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, we recommend three options. The first is seated active quad contractions, where you straighten your leg and squeeze your quad for 10 seconds, repeat this for 10 repetitions, three times a day. Another option is propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. Finally, once you gain more range of motion, strength, and control, add in a banded tke. Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend three options. You can use a stationary bike and start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion. Another option is heel slides. You can use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, at least three times a day, every day. Finally, a more advanced option is quadruped rock backs or tall kneeling rock backs. We recommend kneeling on a pad or pillow for these, and you can even experiment with using a towel behind the knee.
These knee range of motion exercises will help increase your knee’s flexibility and strength. It is essential to perform these exercises regularly to help you recover from your injury.
Hip, Knee and Ankle Strength Exercises
We have put together a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. Within each category, we will provide multiple exercise options ultimately giving you two different workouts to follow.
Before diving into these exercises, we want to mention that these exercises are intended for non-surgical cases. If you had surgery, you will ultimately follow a similar framework but before starting, talk to your doctor or physical therapist as you may have weight-bearing precautions or other considerations to consider.
Category One: Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, here are three options:
Seated active quad contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot in order to intensify the stretch.
Propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
Banded TKE: Place a band behind the back of your knee, anchor to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, here are three options:
Stationary bike: Start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion.
Heel slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, so at least three times a day every day.
Quadruped rock backs or tall kneeling rock backs: Kneel on a pad or pillow for these and experiment with using a towel behind the knee. Anecdotally, we have found this to help patients move into more knee flexion with less discomfort.
Category Two: Hip, Knee and Ankle Strength
Let’s start with a four-step split squat progression which will help increase your tolerance to weight-bearing knee flexion in deeper positions.
Level 1: Body weight squat – Your goal is to perform 3 sets of 20 repetitions, getting your hips to at least parallel. If you need, start with hand assistance such as using a TRX or another object.
Level 2: Heels elevated squat – Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Your goal is 3 sets of 20 repetitions, and again try to get your hips to at least parallel.
Level 3: Split squat – Stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
Level 4: Front foot elevated split squat – Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the hamstrings, the first option will emphasize knee flexion. You can perform standing knee flexion with an ankle weight, use machines, or an exercise we like to use, hamstring sliders. Start with double leg eccentric sliders.
We have put together a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In this section, we will focus on knee range of motion and hip, knee, and ankle strength.
Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. In order to restore extension and flexion equal to your uninjured side, we recommend the following exercises:
Seated active quad contractions: straighten your leg and squeeze your quad for 10 seconds. Repeat for 10 repetitions, three times a day. You can use a towel or strap to pull up on your foot in order to intensify the stretch.
Propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. You can add a weight just above your knee to enhance the stretch.
Banded tke: place a band behind the back of your knee and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend the following exercises:
Stationary bike: start with the seat at a higher level and as range of motion improves, lower the seat to expose the knee to more flexion.
Heel slides: actively slide your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. Do these at least three times a day every day.
Quadruped rock backs or tall kneeling rock backs: kneel on a pad or pillow and use a towel behind the knee. This will help you move into more knee flexion with less discomfort.
Hip, Knee, and Ankle Strength
We recommend the following exercises to increase your tolerance to weight bearing knee flexion in deeper positions:
Four step split squat progression:
Level 1: Body weight squat – perform 3 sets of 20 repetitions getting your hips to at least parallel.
Level 2: Heels elevated squat – elevate your heels two to three inches to allow you to go deeper. Your goal is 3 sets of 20 repetitions and again try to get your hips to at least parallel.
Level 3: Split squat – stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
Level 4: Front foot elevated split squat – elevate your front foot on an object two to four inches high and lower it down driving the front knee forward. Over time, you can increase depth and add weight.
Single leg knee extension: perform for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity.
Hamstring sliders: start with double leg eccentric sliders and progress to single leg. Your goal is to move through the full range of motion with the weight at a challenging intensity.
By following these exercises, you can increase your capacity and tolerance to various stressors and ultimately improve your overall knee function.
So far, there is no clarity on how exercise intensity affects the emission and concentration of aerosol particles in exhaled air. Using a new experimental setup, a research team from Munich has shown that aerosol emissions increase exponentially with intensive physical exertion – so that indoor sports activities result in a higher risk of infectious diseases such as COVID.
Before the study, it was known that tidal volume in untrained people increases from approximately 5-15 liters per minute at rest to more than 100 l/min during exercise. Highly trained athletes even reach levels of 200 l/min. It was also known that many people have become infected with the SARS-CoV-2 virus when they exercise indoors.
However, it was unclear how exercise intensity was related to the concentration of aerosol particles in exhaled air and the actual amount of aerosols an individual exhaled per minute, and thus to the potential risk of spreading infectious diseases such as SARS-CoV-2. However, this information is urgently needed, for example to design mitigation measures for gyms and other indoor sports facilities, fitness studios or discos to avoid closures in the event of serious infection waves.
New methodology produces individually measurable aerosol values
A team led by Henning Wackerhage, professor of exercise biology at the Technical University of Munich (TUM), and Prof. Christian J. Kähler, director of the Institute for Fluid Mechanics and Aerodynamics at the Universität der Bundeswehr Munich, has developed a new research method to study questions. Their experimental equipment initially filtered the aerosols already present in the ambient air. During the subsequent ergometer stress test, the subjects inhaled the purified air through a special mask that covered the mouth and nose. Exercise intensity was gradually increased from rest to the point of physical exhaustion. The mask was connected to a two-way valve that allowed only exhaled air to escape. The amount of aerosol particles emitted per minute was then measured and directly linked to the current performance of the healthy, 18-40 year old subjects.
Moderate aerosol emissions during moderate exertion
This allowed the researchers to investigate for the first time how many aerosol particles are exhaled per minute by an individual at different levels of exercise intensity. The result: aerosol emissions during exercise initially increased only moderately, reaching an average load of about 2 watts per kilogram of body weight. However, above that point they increased exponentially. This means that someone weighing 75 kilograms reaches that threshold at an ergometer setting of approximately 150 watts. This equates to moderate exertion for a casual athlete, perhaps comparable to the exercise intensity of moderate jogging.
The aerosol output of well-trained athletes was significantly higher than that of untrained subjects at maximum exertion, due to their much higher minute ventilation. The researchers found no significant differences in particle emissions between genders.
Protective measures are important for high-intensity training
Although the aerosol experiments provide only indirect knowledge about the amount of viruses in exhaled air, the research suggests useful principles for managing indoor activities when a wave of infections combined with a poorly immunized population threatens to overwhelm the healthcare system.
“Based on our results, we distinguish between moderate endurance training with an intensity of up to 2 watts per kilogram of body weight and training at high to maximum intensity. Due to the sharp increase in aerosol emissions at high-intensity loads above that initial benchmark, special protective measures are necessary if there is a high risk of infections with serious consequences,” says research leader Prof. Wackerhage: “Ideally, that type of training would be moved outside. If that is not possible, testing should be done to ensure that there are no infected persons in the room. Participants must also keep sufficient distance and a highly efficient ventilation system must be running. In addition, infection risks are reduced by training at lower intensity and keeping sessions shorter. It could also be possible for fitness that young athletes should wear masks during training.” At low workloads, such as light to moderate intensity endurance training, less protection is needed, says Prof. Wackerhage, and the risk of infection can be controlled through distancing and ventilation systems.
The research team is currently conducting experiments to compare aerosol emissions during strength and endurance training and to correlate this with the age and physical characteristics of subjects.
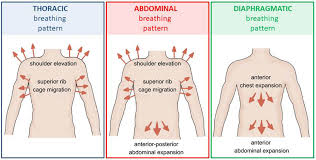
Breathing patterns are an important indicator of an individual’s health. A healthy individual breathes naturally using primary respiratory muscles (e.g., the diaphragm muscle) that produce a rhythmic observable movement of the upper rib cage, lower rib cage, and abdomen. This is known as the diaphragmatic breathing pattern, which is associated with improvements in posture, core stability and functional performance, as well as reductions in musculoskeletal injuries, pain and stress.
In contrast, individuals with altered or dysfunctional biomechanical breathing patterns are unable to contract their diaphragm to the desired extent and begin to rely on accessory respiratory muscles to breathe. They exhibit superior rib cage movements and shoulder elevation, decreased abdominal movements, and lateral expansion of the rib cage.
Previous research suggests a strong link between altered biomechanical breathing patterns and the development of musculoskeletal disorders such as low back pain, neck pain, chronic ankle instability and temporomandibular joint disorders.
Superior physical performance and the prevention of musculoskeletal injuries are critical for athletes to perform their best in competitive sports. Evidence from previous studies suggests that athletes with diaphragmatic breathing patterns exhibit improved physical and psychological performance. But since athletes with altered breathing patterns may be at greater risk of developing musculoskeletal injuries, identifying the prevalence of altered breathing patterns is of paramount importance to prevent them from developing injuries.
Now a team of researchers led by Dr. Terada of Ritsumeikan University in Japan conducted a new study, published in The Journal of Strength and Conditioning Researchto investigate the prevalence of dysfunctional and diaphragmatic breathing patterns in an athletic population, and to determine the biomechanical dimensions of these breathing patterns.
The team tested 1,933 competitive athletes from schools in Japan, across multiple sports and ages, in 2017 and 2020 using a Hi-Lo test – a test that identifies an individual’s breathing pattern. Scores for the Hi-Lo test were determined based on the presence or absence of abdominal excursion, anterior-posterior chest expansion, superior rib cage migration, and shoulder elevation. The team further classified these participants into thoracic dominant and abdominal-only breathers based on the presence of abdominal excursion.
Findings show that an alarmingly high percentage (91%) of athletes showed dysfunctional breathing patterns, while only 9.4% of them showed diaphragmatic breathing patterns. In fact, among athletes who played baseball, there was a higher rate of diaphragmatic breathing pauses than among those who played tennis, basketball, badminton and volleyball. This indicates that athletes’ breathing patterns vary depending on the type of sport they practice, as each sport has different energy needs and limitations.
Additionally, the team found that the majority of dysfunctional breathers were high school student athletes, followed by elementary school student athletes and high school student athletes. The proportion of collegiate athletes with dysfunctional breathing patterns was slightly lower in comparison.
Furthermore, among the population identified as having dysfunctional breathers, 61% of athletes were thoracic-dominant breathers, compared to the 39% who performed only abdominal breathing.
These findings suggest an overall high prevalence of dysfunctional breathing patterns in the athletic population across all age groups, which should be immediately addressed as an important sports medicine problem.
When asked about the implications of these findings, Dr. Terada: “Clinicians should consider screening breathing patterns and implementing corrective approaches that target specific components of dysfunctional breathing patterns. They should also consider evaluating sport-specific breathing adjustments and implementing sport-specific modifications. breathing training protocols.”
The findings also highlight the importance of the Hi-Lo test in recognizing the differences between subcategories (thoracic dominant and abdominal only) of breathing patterns. An understanding of these breathing patterns can help develop individualized intervention plans. Dr. Terada says: “Integrating diaphragmatic breathing exercises and techniques may have beneficial effects on restoring optimal recruitment and motor control patterns of respiratory muscles, improving the efficiency of breathing biomechanics, and reducing psychological stress in athletes with dysfunctional breathing patterns.”
New research shows that by killing essential gut bacteria, antibiotics affect athletes’ motivation and endurance. The UC Riverside-led mouse study suggests that the microbiome is a big factor that differentiates athletes from couch potatoes.
Other studies have examined how exercise influences the microbiome, but this study is one of the few to examine the converse: how gut bacteria also influence voluntary exercise behavior. Voluntary exercise involves both motivation and athleticism.
The researchers’ methods and results are now detailed in the journal Behavioral processes.
“We believed that an animal’s collection of gut bacteria, its microbiome, would influence digestive processes and muscle function, as well as motivation for various behaviors, including exercise,” said Theodore Garland, UCR evolutionary physiologist in whose laboratory the study was conducted. “Our study reinforces this belief.”
Researchers confirmed through stool samples that after ten days of antibiotics, gut bacteria were reduced in two groups of mice: some bred for high levels of running, and others not.
Neither group of mice showed any sign of sickness behavior as a result of antibiotic treatment. So when cycling was reduced by 21 percent in the athletic mice, researchers were confident that damage to the microbiome was responsible. Furthermore, the high runner mice did not recover their running behavior even 12 days after antibiotic treatment was stopped.
The behavior of the normal mice was not significantly affected during or after treatment.
“A normal athlete with a minor injury wouldn’t suffer much. But for a world-class athlete, a small setback can be much bigger,” says Monica McNamara, PhD candidate in evolutionary biology at UCR and first author of the paper . “That’s why we wanted to compare the two types of mice.” Disabling the normal gut microbiome can be compared to an injury.
One way the microbiome may influence exercise in mice or humans is through its ability to convert carbohydrates into chemicals that travel through the body and affect muscle performance.
“Metabolic end products from bacteria in the gut can be reabsorbed and used as fuel,” Garland said. “Less good bacteria means less available fuel.”
In the future, the researchers want to identify the specific bacteria responsible for increased athletic performance. “If we can identify the right microbes, there is the potential to use them as a therapeutic agent to help average people exercise more,” Garland said.
Lack of exercise is known to be a major risk factor for aspects of mental health, including depression, as well as physical health, including metabolic syndrome, diabetes, obesity, cardiovascular disease, cancer and osteoporosis. Many in the public health community would like to promote physical activity, but few have found ways to do so successfully.
“Although we study mice, their physiology is very similar to that of humans. The more we learn from them, the greater our chances of improving our own health,” Garland said.
Certain foods can also increase desirable gut bacteria. As research on “probiotics” develops, Garland recommends that those interested in promoting overall health follow a balanced diet in addition to regular exercise.
“We know from previous studies that the Western diet, which is high in fat and sugar, can have a negative effect on the biodiversity in your gut and probably, by extension, on athletic ability and possibly even motivation to exercise. Garland said.