A few weeks ago I worked virtually with a client who was 10 weeks post-surgery. We had started working together around week 3 and so far he had absolutely dominated the recovery process.
In addition to his physical therapy appointments, he would meet with me virtually once a week to determine the best plan of attack for his workouts with the Neubie… and then he would get after it. By incorporating our recommended workouts with the Neubie 3x per day into his routine, he regained full strength and range of motion before 8 weeks post-surgery.
But around week 10, they started increasing the load at his physical therapy appointments. In particular, they started trying to increase the weight of his exercise on the knee extension machine, which led to a bit of pain in the front of the knee. Each day he returned to do the knee extensions, the pain in the front of his knee increased.
As I mentioned earlier, this client met with me once a week, and by the time we met again, he had reached a point where the pain continued even in his daily activities. He no longer had the ability to fully extend the knee without pain.
Despite doing everything right and botching the first eight weeks of the recovery process, he experienced a setback in week 10.
Setbacks can be difficult, but with the right strategies you can overcome them quickly and emerge stronger.
WARSAW, Ind., October 19, 2023 (GLOBE NEWSWIRE) —Orthopediatrics Corp. (“OrthoPediatrics”) (NASDAQ: KIDS), a company focused solely on advancing the field of pediatric orthopedics, today announced that it has released the new Pediatric Nailing Platform TIBIA System and has successfully completed the first cases of the limited launch has completed. The company received 510(k) clearance from the U.S. Food and Drug Administration (FDA) for the system in September 2023.
PNP Tibia is part of the Trauma & Deformity Correction product range and represents another pediatric-focused solution for the treatment of patients with lower extremity fractures and deformities. It expands the company’s offering to 52 unique systems specifically designed to help address the needs of pediatric patients. The PNP tibial system features rigid cannulated nails ranging in diameter from 7 mm to 12 mm and includes specialized instrumentation to facilitate multiple surgical techniques. Like other OrthoPediatrics products, this system is designed for the anatomy of children and growing patients.
The versatility and scope of the PNP Tibia System were on full display in these two surgical cases. One case was a trauma procedure for a 6-foot teenager requiring a large nail (12mm x 420mm), while the other was a deformity correction procedure for a 15-year-old of smaller stature requiring a 7mm x 285mm was used. These two cases reflect that OP has the broadest scope of pediatric-focused cannulated nails in the industry, allowing surgeons to treat children of all sizes and needs.
Joe Hauser, president of OrthoPediatrics Trauma & Deformity Correction, said: “It is extremely gratifying to see the system perform successfully in two unique and challenging cases. It shows that the surgeon’s expert design team together with the OP engineers have achieved a goal in designing a system that will help many children for years to come.”
About OrthoPediatrics Corp. Founded in 2006, OrthoPediatrics is an orthopedic company focused exclusively on advancing the field of pediatric orthopedics. As such, it has developed the most comprehensive product offering for the pediatric orthopedic market to improve the lives of children with orthopedic conditions. OrthoPediatrics currently markets 52 systems serving three of the largest categories within the pediatric orthopedic market. This product offering includes trauma and deformity, scoliosis and sports medicine/other procedures. OrthoPediatrics’ global sales organization focuses exclusively on pediatric orthopedics and distributes its products in the United States and more than 70 countries outside the United States. For more information, please visit www.orthopediatrics.com.
Contact person for investors Philip Trip Taylor Gilmartin Group philip@gilmartinir.com 415-937-5406
Your immune system is supposed to protect your body, but when you have rheumatoid arthritis (RA), it accidentally attacks healthy joints, tissues, and organs, including the eyes and lungs. As a result, the chronic autoimmune disease causes pain, swelling, stiffness and loss of function in the joints. It can also cause other symptoms, including fatigue, loss of appetite and dry eyes.
RA affects 1.5 million Americans and there is no cure. But it can be managed with medications and lifestyle changes.
Women’s health
Women’s Health magazine featured four women – including Mariah Leach, founder of Mamas Facing Forward – discussing the diagnosis of rheumatoid arthritis, how they cope and what they’ve learned from living with RA.
4 women get real about living with rheumatoid arthritis
A healthy diet is essential for building strong bones and a long, independent life. However, many people are hesitant to change their eating habits. Taste is often the main reason.
Fortunately, research has shown that it is possible to retrain our taste buds. By reshaping our response to certain tastes, we can turn healthy foods we don’t like into delicious, delectable treats.
Today you will discover the science behind taste and how you can apply that knowledge to retrain your taste buds. Once you discover the deliciousness of healthier foods, meeting your nutrition goals will become much easier.
The physical effect of taste
Taste is a multifaceted sensation, where information is obtained from different sources.
On the tongue, receptors convert chemical compounds in food into neural signals. These receptors are your taste buds. When certain compounds come into contact with your taste buds, they identify the compounds as sweet, salty, bitter, sour, or savory.
About half of your taste buds can detect all five taste types to varying degrees, and the other half specializes in detecting the intensity of only one of the five.
Our genetic makeup determines which compounds our taste buds can detect. Scientists have observed how differences in certain genes determine people’s food preferences.1
However, taste buds are not the only source of flavor. Olfactory nerves also transmit information that indicates what food tastes like. That’s why losing your sense of smell can drastically change the way you taste food.
In addition, other forms of sensory information about how something tastes are taken into account, such as temperature, texture and whether a food is spicy. Our brain combines all this sensory information to generate the taste sensation.
Short content
Our taste buds sense chemical compounds in food and send signals to our brain about whether that food is sweet, salty, bitter, sour, or savory. Our olfactory nerves provide information about smell that is included in our perception of taste. In addition, physical sensations such as temperature, texture and spice level influence our sense of taste.
Experience also shapes taste
Exposure and habit also influence our sense of taste. For example, babies prefer foods that their mothers consume during pregnancy. Exposure to those foods in the womb helped them develop a taste for them before they were born. This indicates a relationship between what we eat and how we experience taste.
Eating foods high in sugar can reduce our ability to taste sweetness. Our taste buds adapt based on exposure levels. When they experience high levels of sweetness, they respond by lowering their signal levels. Research has even shown that the number of sweetness-sensitive cells can decrease in response to overstimulation.2
The same goes for salty foods. A high-salt diet causes your taste buds to underestimate the saltiness of food. To achieve the experience of saltiness, even more salt is needed.
Short content
Babies show a preference for foods their mothers ate during pregnancy, showing that experience determines taste. If you often eat foods high in sugar or salt, your taste buds begin to under-report the sweetness and saltiness of your food. Then you have to add more sugar or salt to get the same level of flavor.
Manufactured foods have distorted our sense of taste
Processed foods are notorious for containing excessive amounts of sugar and salt. Because eating too many of those flavors numbs their receptors, processed and manufactured foods reduce our ability to taste salty and sweet.
To accommodate this reduced sensitivity, manufacturers of these processed foods therefore increase the sugar and salt content. This creates a terrible feedback loop that makes processed foods even unhealthier.
While manufactured foods become less and less healthy, pure, unprocessed foods remain the same.
This means that even a delicious fruit or vegetable can taste bland if your taste buds are dulled by excessive sugar and salt intake. Natural foods no longer register as tasty because of the way a diet of processed and manufactured foods has changed your taste buds.
Short content
Processed foods are notoriously high in sugar and salt. Consuming overly salty and sugary foods numbs your taste receptors. Then even more salt and sugar are needed to achieve the same taste level. That means a great-tasting piece of produce might not taste good to someone whose taste buds have been altered by eating foods high in sugar and salt.
We can retrain our taste buds
Research presented by the European Society of Cardiology revealed that participants with hypertension were able to adjust their taste perception to increase their appreciation of a low-sodium diet.
Over the course of the 16-week program, participants reduced their salt intake by 30% and increased their enjoyment of a low-salt diet from a rating of 4.8 to a rating of 6.5 on a 10-point scale.3
A study published in the journal Current Biology found that rats given access to water sweetened with 30% liquid sucrose for four weeks experienced a reduced response to sweetness and even a reduced number of taste buds. However, they also found that when they removed the sucrose fluid from the rats’ water, the effects reversed over the course of just four weeks.4
These studies, involving both humans and animals, show that within weeks you can recalibrate your taste buds to enjoy the authentic taste of whole foods. Try these four strategies to reset your taste buds:
Avoid processed and manufactured foods. – Processed foods are packed with salt, sugar and artificial ingredients. This includes TV dinners, microwaved meals and ready-made meals. Preparing meals from scratch with whole ingredients gives you control over sugar and salt content.
Choose less sweet and less salty ingredients for your recipes and meals. – For example, instead of a bar, take a square of dark chocolate; use unsweetened creamer in your coffee; and swap the white sugar in a recipe for the recommended amount of a plant-based sugar-free sweetener such as stevia or monk fruit.
Eat more produce. – Increase the amount of fresh produce in your diet. Add fresh vegetables to your meals, add spinach to your morning smoothie, or eat a piece of fruit and a handful of almonds instead of a snack bar.
Consume more fiber. – Choose fiber-rich foods, including leafy greens, whole grains and legumes. The extra fiber ensures that you feel full for longer and reduces the need for unhealthy snacks.
Short content
Research has shown that eating foods that are too salty or high in sugar can damage our sense of taste. However, research has also shown that by eliminating excess salt or sugar from your diet, you can restore your natural response to those flavors. By adjusting your diet to reduce salt and sugar intake, you can increase your ability to detect these flavors in food, helping you enjoy a healthier diet.
An alkaline diet of whole foods nourishes your bones
Reducing sugar consumption is beneficial for bone health. Consistently high sugar levels disrupt the bone remodeling cycle and prevent healthy bone development.
Additionally, you’ll provide your body with essential nutrients to build strong bones by eating a diet rich in whole fruits and vegetables. That change also supports the 80/20 pH balanced diet, because fruits and vegetables are alkalizing.
However, this doesn’t mean you can’t enjoy the other foods you love. This diet is not about denial. In fact, the 80/20 pH-balanced diet actually requires that 20 percent of each meal consist of acidifying foods. This can include acidifying plant foods, such as most beans, as well as animal products that contain protein and bone-building minerals, such as eggs, fish and organ meats.
Because reducing salt and sugar intake increases your sensitivity to those flavors, you may develop a taste for healthy foods, making them more flavorful. When your bone-building diet is delicious, it becomes irresistible.
Short content
Reducing sugar intake supports bone health. A diet rich in fruits and vegetables reduces added sugars and salt, while adding bone-building nutrients and helping to achieve the 80/20 balance between alkalizing and acidifying foods. The 20 percent of each meal that sours can be plant foods or animal products.
What this means for you
You have the power to shape your own taste preferences. With a little intentional effort, you can unlock a new world of sweetness and flavor hidden in the whole, natural, mostly alkalizing foods in your grocery store’s produce aisle.
The Save Institute developed Bone Appétite to help you turn these healthy ingredients into great meals. With the right preparation, you can turn a vegetable you fancy into a dish you look forward to. By turning healthy eating into delicious dining, Bone Appétite makes building stronger bones irresistible.
Take back control of your taste buds. Instead of letting the food processing industry dictate your taste, build your palate to appreciate the depth and breadth of flavor of natural, whole foods.
All participants (demographic and anthropometric data are shown in Table 1) successfully completed the experimental sessions without side effects, except for some cases of mild tingling in the fingers at the end of the measurements. Regarding RTD, three men had to be excluded from the data analyzes because the occlusion of arterial blood flow was not possible with the MS and/or LS cuff due to the painful pinching of the skin fold and the stretching of the cuff up to the yield point. In addition, one female was excluded from data analyzes for vsysRPP, SMO2and tHb because arterial blood flow was already occluded at 20% overlap using the HS cuff.
Table 1 Participant characteristics expressed as means ± standard deviations
Overlap to occlusion
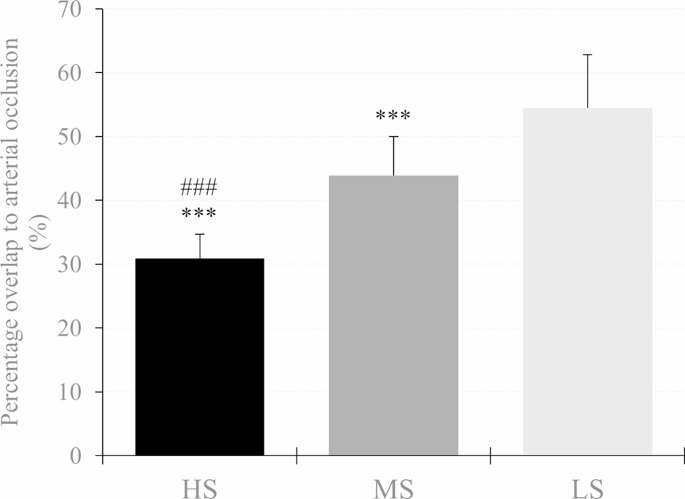
There was a main effect of cuff (F2.62 = 175.679, P< 0.001, theP2= 0.850) and post hoc analysis indicated that RTD was lower in the HS compared to the MS (MD = -13.06% (-16.18 to -9.93%), P< 0.001, D= 2.06) and LS cuff (MD = -23.78% (-26.90 to -20.65%), P< 0.001, D= 3.75). In addition, RTD was also lower using the MS compared to the LS cuff (MD = -10.72% (-13.85 to -7.60%), P< 0.001, D= 1.69). Descriptive data are shown in Table 2; Fig. 3.
Table 2 Hemodynamic, physiological and perceptual responses to progressive practical blood flow restrictions (10%, 20% and 30% overlap relative to the individual’s upper arm circumference) using a high stiffness (HS), medium stiffness cuff ( MS) and low stiffness (LS). Data are expressed as means ± standard deviations
Fig. 3
Percent overlap needed for arterial occlusion in the high stiffness (HS), medium stiffness (MS), and low stiffness (LS) cuff. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ### p < 0.001 respectively
Peak systolic velocity of blood flow
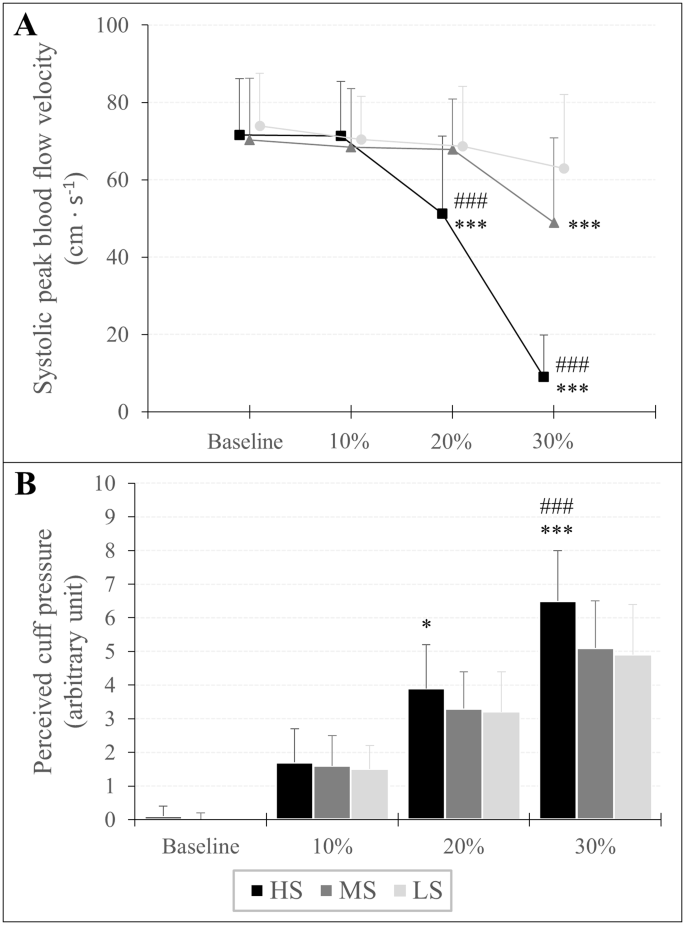
There was an overlap × cuff interaction (F3,642,120,192 = 71.952, P< 0.001, theP2= 0.686) and a main effect of overlap (F1,770,58,422 = 161.427, P< 0.001, theP2= 0.830) and cuff (F2.66 = 50.380, P< 0.001, theP2= 0.604) for vsys. Post hoc analysis showed that vsys was lower at 30% overlap in each cuff compared to baseline (HS: MD = -62.67 cm s− 1(-70.97 to -54.37 cm s− 1 ), P< 0.001, D= 3.95; MS: MD = -21.53 cm s− 1(-29.83 to -13.24 cm s− 1 ), P< 0.001, D= 1.36; LS: MD = -11.02 cm s− 1(-19.31 to -2.72 cm s− 1 ), P< 0.001, D= 0.69). Furthermore, when the HS cuff was applied, vsys was also lower at 20% overlap compared to baseline (MD = -20.51 cm s− 1(-28.80 to -12.21 cm s− 1 ), P< 0.001, D= 1.29). As for cuff differences, vsys was lower at 20% and 30% overlap using the HS cuff compared to the MS (MD = -16.89 cm s− 1(-26.08 to -7.70 cm s− 1 ), P< 0.001, D= 1.07 and MD = -39.91 cm s− 1(-49.11 to -30.71 cm s− 1 ), P< 0.001, D= 2.52, respectively) and the LS cuff (MD = -17.60 cm s− 1(-26.80 to -8.41 cm s− 1 ), P< 0.001, D= 1.11 and MD = -53.99 cm s− 1(-63.18 to -44.79 cm s− 1 ), P< 0.001, D= 3.40 respectively). Furthermore vsys was also lower at 30% overlap using the MS compared to the LS cuff (MD = -14.08 cm s− 1(-23.27 to -4.88 cm s− 1), P< 0.001, D= 0.89). Descriptive data are shown in Table 2; Fig. 4.
Fig. 4
Peak systolic velocity of blood flow (A) and assessment of perceived cuff pressure (B) in response to progressive practical pressure on blood flow restriction, expressed as percent overlap in relation to the individual’s arm circumference. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ###p < 0.001 respectively
Assessment of perceived cuff pressure
An overlap × cuff interaction (F3,946,130,209 = 13.994, P< 0.001, theP2= 0.298) and a main effect of overlap (F1,668,55,046 = 674.771, P< 0.001, theP2= 0.953) and cuff (F2.66 = 11.067, P< 0.001, theP2= 0.251) was found for RPP. A post hoc analysis showed that RPP increased at each %overlap stage compared to baseline for all three cuffs (HS10%: MD = 1.57 au (0.98 to 2.17 au), P< 0.001, D= 1.51; HS20%: MD = 3.80 au (3.21 to 4.40 au), P< 0.001, D= 3.66; HS30%: MD = 6.41 au (5.82 to 7.00 au), P< 0.001, D= 6.16; MS10%: MD = 1.54 au (0.94 to 2.13 au), P< 0.001, D= 1.48; MS20%: MD = 3.32 au (2.72 to 3.91 au), P< 0.001, D= 3.19; MS30%: MD = 5.03 au (4.44 to 5.63 au), P< 0.001, D= 4.84; LS10%: MD = 1.46 au (0.87 to 2.05 au), P< 0.001, D= 1.40; LS20%: MD = 3.18 au (2.59 to 3.77 au), P< 0.001, D= 3.05; LS30%: MD = 4.95 au (4.36 to 5.55 au), P< 0.001, D= 4.76). Regarding differences between cuffs, RPP was higher using the HS cuff with 20% overlap compared to the LS cuff (MD = 0.71 au (0.06 to 1.37 au), P= 0.016, D= 0.69) and with an overlap of 30% compared to Member States (MD = 1.43 (0.78 to 2.09 au), P< 0.001, D= 1.38) and LS cuff (MD = 1.54 au (0.89 to 2.19 au), P< 0.001, D= 1.48). Descriptive data are shown in Table 2; Fig. 4.
Oxygenation of the muscles
SMO2: There was an overlap × cuff interaction (F2,374,78,326 = 3.232, P= 0.037, theP2= 0.089) and a main effect of overlap (F1,297,42,808 = 404,914.= P< 0.001, theP2= 0.925) and gender (F1.33 = 5.096, P= 0.031, theP2= 0.134) for SMO2. Post hoc analysis showed that SMO2 was lower at 20% overlap (HS: MD = -9.94% (-12.43 to -7.45%), P< 0.001, D= 1.15; MS = -8.28% (-10.77 to -5.78%), P< 0.001, D= 0.96; LS: MD = -7.42% (-9.98 to -5.00%), P< 0.001, D= 0.87) and 30% overlap (HS: MD = -17.46% (-19.95 to -14.97%), P< 0.001, D= 2.02; MS: MD = -14.91% (-17.42 to -12.42%), P< 0.001, D= 1.72; LS: MD = -13.79% (-16.28 to -11.30%), P< 0.001, D= 1.59) compared to baseline. Furthermore, the main effect of sex indicated that regardless of overlap and cuff used, SMO2 was lower in men than in women (MD = -5.16% (-9.80 to -0.51%), P= 0.031, D= 0.60).
tHb: An overlap × cuff (F3,072,101,386 = 6,440, P< 0.001, theP2= 0.163) and overlap × sex interaction (F1,187,39,158 = 14.814, P< 0.001, theP2= 0.310) and a main effect of overlap (F1,187,39,158 = 117,125.= P< 0.001, theP2= 0.780) and gender (F1.33 = 27.981, P< 0.001, theP2= 0.459) was found for tHb. Post hoc tests showed that tHb was higher at 20% overlap (HS: MD = 0.13 au (0.09 to 0.18 au), P< 0.001, D= 0.45; MS: MD = 0.10 au (0.05 to 0.14 au), P< 0.001, D= 0.32; LS: MD = 0.06 au (0.02 to 0.11 au), P< 0.001, D= 0.20) and 30% overlap (HS: MD = 0.22 au (0.18 to 0.27 au), P< 0.001, D= 0.75; MS: MD = 0.17 au (0.12 to 0.21 au), P< 0.001, D= 0.55; LS: MD = 0.15 au (0.10 to 0.19 au), P< 0.001, D= 0.45) compared to baseline. Moreover, tHb was already higher at a 10% overlap using the HS (MD = 0.05 au (0.00 to 0.09 au), P= 0.018, D= 0.16) compared to baseline. Regarding sex differences, post hoc analysis showed that regardless of cuff, tHb was higher by 10% (MD = 0.06 au (0.01 to 0.10 au), P= 0.003, D= 0.20), 20% (MD = 0.15 au (0.11 to 0.20 au), P< 0.001, D= 0.52) and 30% overlap (MD = 0.24 au (0.19 to 0.29 au), P< 0.001, D= 0.80) in men, while in women tHb was only higher during a 30% overlap compared to baseline (MD = 0.12 au (0.07 to 0.16 au), P< 0.001, D= 0.39). In addition, tHb was higher in men compared to women at baseline (MD = 0.51 au (0.31 to 0.70 au), P< 0.001, D= 1.69). Descriptive data are shown in Table 2.
Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion pain.
Corns and calluses on the friction site of the big toe and second toe
Limited movement of the big toe
What is a lapiplasty?
People often have the misconception that bunions can be fixed by just shaving off the bone, thinking it is an overgrowth. In reality, there are deeper issues that are causing the problems you are experiencing. In the past, bunion surgery approached the problem on a two-dimensional plane, while the problem to be addressed was three-dimensional. This is where Lapiplasty comes into play. With LapiplastyⓇ 3D Bunion Correction, instead of doing what traditional bunion surgery does, which is cutting the bone in half and shifting, Lapiplasty rotates the entire spine of the foot to repair the anatomical deformity that causes the bunions to form. By doing this, the chance of your bunions returning is minimal.
If you suffer from bunions, Bone and Joint Specialists Orthopedic & Spine Center is the right place for you. With 4 locations in Indiana, we offer extensive access to our physicians who can provide you with world-class service. Working with us means you work with the best. Contact us today at 219.795.3360 or visit us online at www.orthopedicdoctors.com to schedule your consultation.
It is usually normal for your knee to feel numb and tingly after ACL surgery. This is because some small nerves are cut during the surgical procedure. Don’t worry, we’re not talking about the really important nerves that allow you to bend and straighten your knee, but the nerves that allow you to feel things around your knee. This video below explains all the reasons why your knee may feel numb and tingly after ACL surgery. For more information, read this blog about 5 tips to help you recover after ACL surgery.
Lauren Youssef, a physiotherapy student at the University of Toronto, explains why your knee may feel numb and tingly after ACL surgery.
Read Lauren’s blog: Why is my knee numb and tingling after ACL surgery? | Curovat
There are also 5 great blogs written by Lauren on our site where you can learn more about surgery and injury recovery.
If you have had an ACL injury or surgery, download Curovate from the links below. Curovate is a physical therapy app that offers daily video-guided exercises, progress tracking, in-app chat with a physical therapist to answer your questions about surgery or injury, and the ability to measure your knee’s range of motion using just your phone.
If you need more tailored help during your surgery or recovery from your injury, check out our Virtual Physiotherapy page to book your 1-on-1 video session with a physiotherapist.
Other blogs related to ACL injuries:
References
1. Horteur, C., Cavalié, G., Gaulin, B., Cohen Bacry, M., Morin, V., Cavaignac, E., & Pailhé, R. (2020). Saphenous nerve damage after anterior cruciate ligament reconstruction: Decreased area of numbness after ligamentoplasty using the quadriceps tendon compared to the hamstring tendon. The Knee, 27(4), 1151–1157.
2. Inderhaug, E., Strand, T., and Solheim, E. (2015). The impact of sensory deficits after hamstring autograft harvesting for ACL reconstruction. Knee surgery, sports traumatology, arthroscopy: Official Journal of the ESSKA, 23(4), 1060–1064.
3. Kjaergaard, J., Faunø, L. Z., & Faunø, P. (2008). Loss of sensation after ACL reconstruction with hamstring graft. International Journal of Sports Medicine, 29(6), 507–511.
4. Nerve Blocks for Surgery – Yale Medicine. (2020, July 02). Retrieved from https://www.yalemedicine.org/conditions/nerve-blocks-for-surgery
5. Ochiai, S., Hagino, T., Senga, S., Yamashita, T., Oda, K., & Haro, H. (2017). Damage to the infrapatellar branch of the saphenous nerve in anterior cruciate ligament reconstruction using vertical skin incision for hamstring harvesting: risk factors and influence on treatment outcome. Journal of Orthopedic Surgery and Research, 12(1), 101.
6. Sanders, B., Rolf, R., McClelland, W., and Xerogeanes, J. (2007). Prevalence of saphenous nerve damage after autogenous hamstring harvest: an anatomical and clinical study of tailor branch injury. Arthroscopy: The Journal of Arthroscopic and Related Surgery: Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 23(9), 956–963.
7. Wang, H. D., Zhang, H., Wang, T. R., Zhang, W. F., Wang, F. S., & Zhang, Y. Z. (2018). Comparison of clinical outcomes after anterior cruciate ligament reconstruction with hamstring tendon autograft versus soft tissue allograft: a meta-analysis of randomized controlled trials. International Journal of Surgery (London, England), 56, 174–183.
This opportunity allows highly motivated students interested in orthopedics to be integrated into our academic orthopedics department for a year. You will be in constant conversation with faculty, residents, and department researchers as you learn the basics of research design, methodology, data analysis, and how to navigate the process from IRB application to manuscript submission. In addition to research, there are weekly opportunities for clinical exposure including surgery, clinic and department conferences. There are 3 tracks available: Basic Sciences, Pediatric Orthopedics, centered at the Children’s Hospital of New Orleans, and Adult Orthopedics, centered on the LSU medical school campus (however, all fellows will spend some time at each location).
A commitment for 1 academic year (fall to summer).
Develop and complete at least 2-3 independent research projects
Facilitate ongoing student/resident research projects where necessary.
Manage the content of research websites
Transporting research material, for example from operating theater to laboratories
Personal transportation required
Present your progress at monthly department research meetings
Attend weekly clinics and/or surgeries with various faculty members
Participate in the LSU Ortho student research committee
Participate in health disparities research (a department priority), including tissue bank projects, proposals, and grant submissions
Attend all department didactic/teaching sessions
Assist in developing/maintaining databases for surgical research
Effectively communicate the status of each project and progress with research team members
Select 1 of the 3 tracks (basic sciences, clinical adults/trauma, clinical pediatrics)
Full-time position, approximately $1150/month stipend
For more information please contact Dr. Vinod Dasa (This email address is being protected from spambots. You need JavaScript enabled to view it.) with regard to the orthopedic direction of adult and basic sciences or Dr. Carter Clement (This email address is being protected from spambots. You need JavaScript enabled to view it.) regarding pediatric orthopedics training.
This morning started early after a long day yesterday. The burning sensation disappeared. I’m pretty sure it was something in the bath oil that caused me to have a bad reaction.
I drove to Yosemite (it’s an hour away) via the one-way bridge that cars cross in both directions. I got into the Yosemite gate pretty quickly. I drove another 20 minutes to the meeting spot. I was early so I stopped to take some photos at some take-out points.
I met up with Katherine and we got in her car to go to the next spot. It was Tuolumne Grove to see the gigantic majestic redwood trees. We walk through the forest.
Then we got in the car and drove to Olmsted Point where we walked a bit, took pictures and meditated for a while. There’s a fire in the park, so today the air was smoky.
Then we went to Taneya Lake where we ate a packed lunch she brought. It was nice to sit in her camp chairs and have lunch by a beautiful lake. One interesting fact: the boulders and trees all had rings around them. It was a trail left by the lake this year after the historic snowfall. The water rose so high!
Then we went to Tuolumne Meadow to Soda Springs. It’s a nice walk to see water that is actually naturally carbonated. Scientists can’t figure out why. I also used an outhouse for the first time in a long time.
We then headed back to Olmsted Point because the smoke cleared and I was able to get a better photo.
That was the end of my tour/walk for the day. I drove back to the room to shower and get ready for dinner. Tonight I decided to get take out and eat on my porch.
Now I have to go to bed, because tomorrow is coming soon. It was going to rain, so this walk will be interesting!
By the way, if you’re interested in the dog, she was caught watching football with her boyfriend.
Most of us know from experience that tossing and turning at night means you’ll feel bad the next day. And many of us understand that there are long-term health consequences when we get too little sleep.
But recently I discovered something new from a fascinating study into sleep and its effect on how quickly women’s genes age after menopause – what’s known as their ‘epigenetic age’. (Carroll et al. 2017)
In the study, postmenopausal women with five insomnia symptoms were biologically almost two years older than comparable women without insomnia symptoms. The more symptoms of insomnia – Waking up during the night, not being able to fall asleep, disturbed sleep and so on – the greater the effect. However, if you only sleep six hours a night, it appears that your epigenetic age does not increase, as long as it is a good night’s sleep. And that, of course, is what many of us have problems with.
So what can we do about this? I would like to point out that the research shows that our genes are not completely out of our control, and that we can influence how they respond by taking better care of ourselves. For those of us who have gone through menopause and may be having trouble sleeping, this means looking at ways we can improve our rest.
4 sleep tips to try
Keep a regular schedule. Your brain likes consistency, so go to bed at 11 p.m. and at the same regular time every night and in a dark room. When you get up, immediately soak up the morning light by going outside or opening a window. Ensuring good light health is key to your circadian health.
Turn off the electronics! Computers, TVs, phones: they’re all the enemy of sleep. Even a short duration of light shining into your eyes tricks your brain into thinking it’s time to wake up. Every night at least an hour before bed, turn off the phone and put it on the charger in another room so you aren’t tempted to look at it when you can’t sleep.
Eat early and in moderation. Heavy meals just before bed disrupt sleep, while avoiding caffeine and stimuli (such as dramatic/stressful TV shows) can also help with sleep.
Once you’re in bed, stay relaxed. Once you’re in bed, consider practicing relaxing belly breathing or guided visualizations like that of Yoga Nidra.
In the checklist above you will see some of my favorite sleep remedies, including of course L-Tryptophan, which can be combined with magnesium for an even more relaxing effect.
Reference: Carroll, JE et al. 2017. Epigenetic aging and immune aging in women with insomnia symptoms: findings from the Women’s Health Initiative Study, Biological Psychiatry 81(2):136-144.
I am Dr. Susan E. Brown. I am a clinical nutritionist, medical anthropologist, writer and motivational coach speaker. Learn my proven 6-step natural approach to bone health in my online courses.






 Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion
Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion 












 4 sleep tips to try
4 sleep tips to try I am Dr. Susan E. Brown. I am a clinical nutritionist, medical anthropologist, writer and motivational coach speaker. Learn my proven 6-step natural approach to
I am Dr. Susan E. Brown. I am a clinical nutritionist, medical anthropologist, writer and motivational coach speaker. Learn my proven 6-step natural approach to