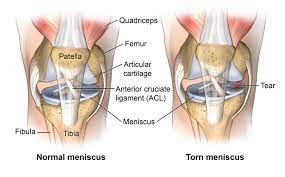
We will be discussing meniscus tears, their function, and why surgery might not be the best option. The meniscus is a fibrocartilaginous structure located between the femur and tibia in the knee joint. There are two menisci in each knee, the medial meniscus, and the lateral meniscus. They function to provide shock absorption, force transmission, and stability to the knee joint.
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears have a distinct mechanism of injury, while non-traumatic tears occur secondary to age-related changes. Meniscus tears are often classified according to location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Surgery to repair or remove the meniscus was performed in the past to reduce symptoms of pain and mechanical symptoms, such as clicking, catching, and locking of the knee. However, the current scientific literature does not fully support this theory.
symptoms and signs of a meniscus tear:
- Pain and swelling in the knee joint
- Difficulty straightening or bending the knee
- Feeling a popping sensation in the knee
- A locking or catching sensation in the knee joint
If you suspect you have a meniscus tear, it’s important to see a doctor for an accurate diagnosis and appropriate treatment.
Key Takeaways
- Mechanical symptoms are not a reliable indicator of the presence of meniscal tears.
- Meniscus tears are common in asymptomatic individuals.
- Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions.
Understanding Meniscus Tears
We want to provide you with a comprehensive understanding of meniscus tears. The meniscus is a fibrocartilaginous structure located between the femur and tibia bones in the knee joint. There are two menisci in each knee, the medial meniscus located on the inner portion of the knee and the lateral meniscus located on the outer portion. The menisci function to provide shock absorption, force transmission, and stability to the knee joint.
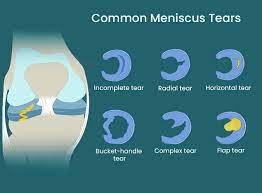
Meniscus tears are either traumatic or non-traumatic. Traumatic tears occur due to a distinct mechanism of injury, whereas non-traumatic tears occur secondary to age-related changes. Meniscus tears are often classified according to location and orientation, including vertical, longitudinal, radial, horizontal, oblique, or complex tears. Vertical or oblique tears that twist and fold over within the joint are termed bucket handle tears.
In the past, the presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. However, current scientific literature does not fully support this theory. Researchers have found that mechanical symptoms are equally prevalent in patients with and without a meniscal tear and are common in those with knee problems in general. Therefore, these symptoms have limited utility as an indicator for the presence of meniscal tears or are not useful clues to the diagnosis.
Meniscus tears are common in asymptomatic individuals. One study found that in 230 uninjured knees, 30 percent had meniscal tears. If tears are prevalent in a non-painful population, it brings into question the efficacy of surgery in reducing symptoms. Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, a brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain function and quality of life compared to placebo surgery.
At this moment, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears. Exercise has been shown to be just as effective in the long term for both populations. We have one study that showed exercise led to similar improvements in pain function and quality of life after 12 months in a younger population with mostly traumatic tears and another study that showed no clinically relevant difference in the function after two years in an older population with degenerative tears.
We want to provide you with a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category. The first category is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. You should aim to restore extension and flexion that is equal to your uninjured side. We recommend three options for knee extension or straightening and three options for knee flexion or bending.
The second category is hip, knee, and ankle strength. We recommend a four-step split squat progression, which will help increase your tolerance to weight-bearing knee flexion in deeper positions. We also recommend a single-leg knee extension and hamstring sliders to work on quadriceps and hamstring strength.
In conclusion, meniscus tears are a common knee injury that can be managed conservatively through exercise. Surgery has not been shown to provide better outcomes compared to other interventions. Our comprehensive rehab program covers multiple categories aimed at increasing your capacity and tolerance to various stressors. We recommend following this program for non-surgical cases. Always talk to your doctor or physical therapist before starting any exercise program.
Myths About Meniscus Tears
We often hear that meniscus tears are the cause of knee pain and mechanical symptoms such as clicking, catching, and locking of the knee. However, recent scientific literature does not fully support this theory. Here are three things you should know about meniscus tears:
- There is not a simple cause and effect relationship between symptoms and tears. Patients with and without a meniscal tear have been found to have the same mechanical symptoms, which are actually common in those with knee problems in general.
- Meniscus tears are common in asymptomatic individuals. In one study, 30% of uninjured knees had meniscal tears, which brings into question the efficacy of surgery in reducing symptoms.
- Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, surgery can even lead to an increased risk of developing radiographic knee osteoarthritis.
Given this information, conservative management is favored for those with degenerative meniscus tears. Exercise has been shown to be just as effective in the long term for both younger patients with traumatic tears and older patients with degenerative tears.
We provide a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In the knee range of motion category, we recommend exercises such as seated active quad contractions, propping your heel up on an elevated surface, and banded tke. In the hip, knee, and ankle strength category, we recommend exercises such as the four-step split squat progression and single leg knee extensions for the quadriceps, and standing knee flexion with an ankle weight or hamstring sliders for the hamstrings.
It is important to note that these exercises are intended for non-surgical cases. If you had surgery, you should talk to your doctor or physical therapist before starting any exercise program.
Research on Meniscus Tears
The meniscus is a fibrocartilaginous structure that is located between the femur and tibia in the knee joint. There are two menisci in each knee, the medial and lateral meniscus. They provide shock absorption, force transmission, and stability to the knee joint.
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears occur due to a distinct mechanism of injury, while non-traumatic tears occur secondary to age-related changes. Tears can be classified according to their location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Bucket handle tears are vertical or oblique tears that twist and fold over within the joint.
In the past, the presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. Therefore, surgery to repair or remove the meniscus was performed to reduce symptoms. However, current scientific literature does not fully support this theory.
There is not a simple cause and effect relationship between symptoms and tears. Mechanical symptoms are equally prevalent in patients with and without a meniscal tear, and are actually common in those with knee problems in general. Meniscus tears are also common in asymptomatic individuals, with one study finding that 30 percent of uninjured knees had meniscal tears.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. A popular study compared a partial meniscectomy to a placebo or sham surgery and found that surgery provided no more benefit for knee symptoms or function than placebo surgery. It even led to an increased risk of developing radiographic knee osteoarthritis. A brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery.
Exercise has been shown to be just as effective in the long term for both younger and older populations with meniscus tears. Clinical practice guidelines favor conservative management in those with degenerative meniscus tears.
We provide a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. The program includes knee range of motion exercises, hip, knee, and ankle strength exercises, balance and proprioception exercises, and cardiovascular exercise.
Surgical Interventions
We have learned that surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. In fact, a recent Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery. Therefore, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears.
Instead, we recommend a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. We will provide multiple exercise options within each category, ultimately giving you two different workouts to follow. These exercises are intended for non-surgical cases. If you had surgery, you should talk to your doctor or physical therapist before starting, as you may have weight-bearing precautions or other considerations to consider.
The first category is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side. For knee extension or straightening, we recommend seated active quad contractions, propping your heel up on an elevated surface, and banded tke. For knee flexion or bending, we recommend using a stationary bike, heel slides, and quadruped rock backs or tall kneeling rock backs.
The second category is hip, knee, and ankle strength. For quadriceps, we recommend a four-step split squat progression and a single-leg knee extension. For hamstrings, we recommend standing knee flexion with an ankle weight, machines, or hamstring sliders.
By following these exercises, you can increase your tolerance to weight-bearing knee flexion in deeper positions and improve your knee symptoms related to a degenerative meniscus tear.
Non-Surgical Interventions
We understand that meniscus tears can cause pain and other mechanical symptoms in the knee joint. However, surgery may not always be the best option for treating this condition. In fact, current scientific literature does not fully support the idea that surgery to repair or remove the meniscus leads to better outcomes compared to other interventions.
Therefore, we recommend a comprehensive rehab program that includes exercise progressions with sets and reps. This program aims to increase your capacity and tolerance to various stressors within each category. We have categorized the exercises into two main categories:
Category One: Knee Range of Motion
The first category focuses on restoring knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. If not, you should aim to restore extension and flexion that is equal to your uninjured side.
Here are three exercises that can help with knee extension:
- Seated Active Quad Contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot to intensify the stretch.
- Heel Prop: Prop your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration.
- Banded TKE: Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion, here are three exercises that can help:
- Stationary Bike: Start with the seat at a higher level, and as your range of motion improves, lower the seat to expose the knee to more flexion.
- Heel Slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, at least three times a day, every day.
- Quadruped Rock Backs or Tall Kneeling Rock Backs: Kneel on a pad or pillow for these exercises. You can even experiment with using a towel behind the knee, which can help patients move into more knee flexion with less discomfort.
Category Two: Hip, Knee, and Ankle Strength
The second category focuses on hip, knee, and ankle strength. We recommend a four-step split squat progression that will help increase your tolerance to weight-bearing knee flexion in deeper positions.
Here are the four levels of the split squat progression:
- Body Weight Squat: Perform three sets of 20 repetitions, getting your hips to at least parallel. If you need to, start with hand assistance, such as using a TRX or another object.
- Heels Elevated Squat: Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Perform three sets of 20 repetitions, and again, try to get your hips to at least parallel.
- Split Squat: Stand in a split stance and lower down while driving the front knee forward as far as you can. Perform three sets of 15 controlled reps on each leg before progressing.
- Front Foot Elevated Split Squat: Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the hamstrings, we recommend standing knee flexion with an ankle weight, using machines, or performing hamstring sliders. Start with double-leg eccentric sliders for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity, but to start, you can shorten the range of motion or even perform with no weight if needed.
In conclusion, exercise has been shown to be just as effective in the long term for treating meniscus tears compared to surgery. Therefore, we recommend a comprehensive rehab program that includes these exercises to help you recover from this condition.
Exercise as a Treatment Option
We have seen that surgery for meniscus tears may not be the best option, and that exercise can be just as effective in the long term for both younger and older populations. Therefore, we present a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category.
Knee Range of Motion
The first category we will cover is knee range of motion. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, we recommend three options. The first is seated active quad contractions, where you straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot in order to intensify the stretch.
Another option is propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
Finally, once you gain more range of motion, strength, and control, add in a banded tke. Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend three options. You can use a stationary bike and start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion. Another option is heel slides. You can use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, so at least three times a day, every day.
Finally, a more advanced option is quadruped rock backs or tall kneeling rock backs. We recommend kneeling on a pad or pillow for these, and you can even experiment with using a towel behind the knee. Anecdotally, we have found this to help patients move into more knee flexion with less discomfort.
Hip, Knee, and Ankle Strength
The second category we will cover is hip, knee, and ankle strength. Let’s start with a four-step split squat progression, which will help increase your tolerance to weight bearing knee flexion in deeper positions.
Level 1 is a bodyweight squat. Your goal is to perform three sets of 20 repetitions, getting your hips to at least parallel. If you need, start with hand assistance such as using a TRX or another object.
Level 2 is a heels elevated squat. Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Your goal is three sets of 20 repetitions, and again, try to get your hips to at least parallel.
Level 3 is a split squat. Stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
Level 4 is a front foot elevated split squat. Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the quadriceps, we recommend a single leg knee extension for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity, but to start, you can shorten the range of motion or even perform with no weight if needed.
For the hamstrings, the first option will emphasize knee flexion. You can perform standing knee flexion with an ankle weight, use machines, or an exercise we like to use called hamstring sliders. Start with double leg eccentric sliders before progressing to single leg eccentric sliders.
We hope this comprehensive rehab program will help you increase your capacity and tolerance to various stressors, ultimately leading to better knee function and quality of life.
Rehab Program
We will now discuss a comprehensive rehab program for meniscus tears, which includes exercise progressions with sets and reps. The meniscus is a fibrocartilaginous structure located between the femur and tibia bones in the knee joint. There are two menisci in each knee, the medial meniscus on the inner portion and the lateral meniscus on the outer portion. The menisci provide shock absorption, force transmission, and stability to the knee joint.
Meniscus tears can be either traumatic or non-traumatic. Traumatic tears occur due to a specific injury, while non-traumatic tears occur due to age-related changes. Tears can be classified according to location and orientation, such as vertical, longitudinal, radial, horizontal, oblique, or complex. Vertical or oblique tears that twist and fold over within the joint are termed bucket handle tears.
In the past, pain and mechanical symptoms such as clicking, catching, and locking of the knee were thought to be caused by a meniscus tear. Therefore, surgery to repair or remove the meniscus was performed to reduce symptoms. However, current scientific literature does not fully support this theory.
There is not a simple cause and effect relationship between symptoms and tears. For example, a 2018 study found that mechanical symptoms were equally prevalent in patients with and without a meniscal tear and are actually common in those with knee problems in general. Other research has concluded that these symptoms have limited utility as an indicator for the presence of meniscal tears or are not useful clues to the diagnosis.
Meniscus tears are common in asymptomatic individuals. In one study, researchers found that in 230 uninjured knees, 30 percent had meniscal tears. If tears are prevalent in a non-painful population, it questions the efficacy of surgery in reducing symptoms.
Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions. For example, a popular study compared a partial meniscectomy to a placebo or sham surgery over the course of five years. Surgery provided no more benefit for knee symptoms or function than placebo surgery. It even led to an increased risk of developing radiographic knee osteoarthritis. In fact, a brand new Cochrane review concluded that arthroscopic surgery for degenerative meniscal tears provides little to no clinical benefit for pain, function, and quality of life compared to placebo surgery.
Exercise has been shown to be just as effective in the long term for both populations. One study showed exercise led to similar improvements in pain, function, and quality of life after 12 months in a younger population with mostly traumatic tears. Another study showed no clinically relevant difference in function after two years in an older population with degenerative tears.
Therefore, current clinical practice guidelines favor conservative management in those with degenerative meniscus tears. We will now present a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors within each category. We will provide multiple exercise options, ultimately giving you two different workouts to follow.
Before diving into these exercises, there is one caveat we want to mention. These exercises are intended for non-surgical cases. If you had surgery, you will ultimately follow a similar framework, but before starting, talk to your doctor or physical therapist as you may have weight-bearing precautions or other considerations to consider.
Category One: Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At a minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, here are three options:
- Seated active quad contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot to intensify the stretch.
- Propping your heel up on an elevated surface: Elevate your heel on a surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
- Banded TKE: Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, here are three options:
- Stationary bike: Start with the seat at a higher level and lower it as range of motion improves to expose the knee to more flexion.
- Heel slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions.
Knee Range of Motion Exercises
We will now discuss knee range of motion exercises that are essential for rehabilitating meniscus tears. The meniscus is a vital structure that provides shock absorption, force transmission, and stability to the knee joint. Meniscus tears can be traumatic or non-traumatic and can be classified based on their location and orientation. The presence of pain and mechanical symptoms such as clicking, catching, and locking of the knee were traditionally thought to be caused by a meniscus tear. However, surgery to repair or remove the meniscus has not been shown to lead to better outcomes compared to other interventions.
Therefore, we recommend a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In the first category, we will focus on knee range of motion exercises. Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, we recommend three options. The first is seated active quad contractions, where you straighten your leg and squeeze your quad for 10 seconds, repeat this for 10 repetitions, three times a day. Another option is propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. Finally, once you gain more range of motion, strength, and control, add in a banded tke. Place a band behind the back of your knee, anchor it to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend three options. You can use a stationary bike and start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion. Another option is heel slides. You can use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, at least three times a day, every day. Finally, a more advanced option is quadruped rock backs or tall kneeling rock backs. We recommend kneeling on a pad or pillow for these, and you can even experiment with using a towel behind the knee.
These knee range of motion exercises will help increase your knee’s flexibility and strength. It is essential to perform these exercises regularly to help you recover from your injury.
Hip, Knee and Ankle Strength Exercises
We have put together a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. Within each category, we will provide multiple exercise options ultimately giving you two different workouts to follow.
Before diving into these exercises, we want to mention that these exercises are intended for non-surgical cases. If you had surgery, you will ultimately follow a similar framework but before starting, talk to your doctor or physical therapist as you may have weight-bearing precautions or other considerations to consider.
Category One: Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.
For knee extension or straightening, here are three options:
- Seated active quad contractions: Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, three times a day. If your motion is improving, you can use a towel or strap to pull up on your foot in order to intensify the stretch.
- Propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration, so while it may feel slightly uncomfortable, it should not be unbearable.
- Banded TKE: Place a band behind the back of your knee, anchor to an object, and perform the same quad contractions against resistance.
For knee flexion or bending, here are three options:
- Stationary bike: Start with the seat at a higher level. As range of motion improves, lower the seat to expose the knee to more flexion.
- Heel slides: Use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. You should do these often, so at least three times a day every day.
- Quadruped rock backs or tall kneeling rock backs: Kneel on a pad or pillow for these and experiment with using a towel behind the knee. Anecdotally, we have found this to help patients move into more knee flexion with less discomfort.
Category Two: Hip, Knee and Ankle Strength
Let’s start with a four-step split squat progression which will help increase your tolerance to weight-bearing knee flexion in deeper positions.
Level 1: Body weight squat – Your goal is to perform 3 sets of 20 repetitions, getting your hips to at least parallel. If you need, start with hand assistance such as using a TRX or another object.
Level 2: Heels elevated squat – Elevate your heels two to three inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Your goal is 3 sets of 20 repetitions, and again try to get your hips to at least parallel.
Level 3: Split squat – Stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
Level 4: Front foot elevated split squat – Elevate your front foot on an object two to four inches high and lower it down, driving the front knee forward. Over time, you can increase depth and add weight.
For the hamstrings, the first option will emphasize knee flexion. You can perform standing knee flexion with an ankle weight, use machines, or an exercise we like to use, hamstring sliders. Start with double leg eccentric sliders.
We have put together a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. In this section, we will focus on knee range of motion and hip, knee, and ankle strength.
Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. In order to restore extension and flexion equal to your uninjured side, we recommend the following exercises:
- Seated active quad contractions: straighten your leg and squeeze your quad for 10 seconds. Repeat for 10 repetitions, three times a day. You can use a towel or strap to pull up on your foot in order to intensify the stretch.
- Propping your heel up on an elevated surface for 10 to 15 minutes, three times a day. You can add a weight just above your knee to enhance the stretch.
- Banded tke: place a band behind the back of your knee and perform the same quad contractions against resistance.
For knee flexion or bending, we recommend the following exercises:
- Stationary bike: start with the seat at a higher level and as range of motion improves, lower the seat to expose the knee to more flexion.
- Heel slides: actively slide your heel towards your butt for 10 to 15 repetitions. As motion improves, progress by using a towel or strap to pull the knee into more flexion. Do these at least three times a day every day.
- Quadruped rock backs or tall kneeling rock backs: kneel on a pad or pillow and use a towel behind the knee. This will help you move into more knee flexion with less discomfort.
Hip, Knee, and Ankle Strength
We recommend the following exercises to increase your tolerance to weight bearing knee flexion in deeper positions:
- Four step split squat progression:
- Level 1: Body weight squat – perform 3 sets of 20 repetitions getting your hips to at least parallel.
- Level 2: Heels elevated squat – elevate your heels two to three inches to allow you to go deeper. Your goal is 3 sets of 20 repetitions and again try to get your hips to at least parallel.
- Level 3: Split squat – stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is three sets of 15 controlled reps on each leg before progressing.
- Level 4: Front foot elevated split squat – elevate your front foot on an object two to four inches high and lower it down driving the front knee forward. Over time, you can increase depth and add weight.
- Single leg knee extension: perform for three to four sets of 10 to 15 reps on each leg. Your goal is to move through the full range of motion with the weight at a challenging intensity.
- Hamstring sliders: start with double leg eccentric sliders and progress to single leg. Your goal is to move through the full range of motion with the weight at a challenging intensity.
By following these exercises, you can increase your capacity and tolerance to various stressors and ultimately improve your overall knee function.

