Injuries in youth athletics are significantly reduced when coaches and parents have access to digital information about adolescent growth. It also takes twice as long for the first injury to occur. This is evident from a study by Linköping University, published in the British Journal of Sports Medicine.
Many promising athletes have had their careers ruined by injuries. One thing that almost all athletic events have in common is high loads for a short period of time, such as jumping, throwing and running. This leads to overuse injuries such as groin pain and sore shoulders, but also to sudden injuries such as ankle sprains and hamstring tears.
Jenny Jacobsson is a physiotherapist and visiting researcher at the Athletics Research Center of Linköping University. She has worked for many years as a medical coordinator for the Swedish national athletics team and has seen the impact of injuries on athletes.
“Before the 2008 Beijing Olympics, we saw a lot of injuries in our national team and tried to find out why. At the time, no research had been done into the incidence of injuries in track and field athletes. But we wanted to know what was happening among our elite. athletes aged 16 and over, including adult elite athletes,” says Jenny Jacobsson.
The research into injuries in Swedish athletics showed that one of the main causes of injuries was previous injuries. This means that the earlier an athlete is injured in their career, the more likely they are to be injured later and more often. But the causes of injuries in youth sports are a complex issue, involving everything from training amount and load to equipment and even sleep.
Together with her colleagues at the Athletics Research Center, Jenny Jacobsson has developed a digital health platform with information for parents and youth coaches about adolescent growth and how it is influenced by training, with a focus on track and field athletes aged 12-15.
To investigate whether this type of platform can prevent injuries, the researchers conducted a study in which 21 athletics clubs with athletes aged 12 to 15 were randomized into two groups: an intervention group and a control group. During the preseason, the parents and coaches of the intervention group were given access to the digital information platform for four months, which was not accessible to outsiders at the time (but is now accessible to everyone). They were also regularly encouraged to log in and explore its content.
The researchers noted that the clubs that accessed the information showed significantly lower injury incidence and took twice as long for the first injury to occur. Moreover, the effect was greater at large clubs. The results, published in the British Journal of Sports Medicine, could point the way to more injury-free athletics.
“We have not investigated the mechanism that leads to change, but we see that digital information works when it comes to injury prevention. If coaches and parents learn to recognize the problems, it is possible to reduce the training burden in time. Medically speaking, we do know.” what happens in growing bodies, but spreading the information to those who could benefit from it has been a challenge. This platform can bridge that gap,” says Jenny Jacobsson.
The research was funded by the Swedish Research Council for Sports Sciences (Centrum för idrottsforskning).
Concussions are an unfortunate reality in contact sports at the junior and senior levels. Now sports experts from the University of South Australia suggest longer recovery times may be needed for youth athletes suffering from head trauma, as new research shows concussion can increase future injury risk by 50%.
Published in the Journal for Science and Medicine in Sports,the world’s first study tracked and evaluated the long-term impact of concussion and subsequent injury risk in 1455 sub-elite junior Australian football players.
This builds on previous UniSA research which found that sub-elite Australian Rules footballers returning from injury are approximately 1.5 times more likely to suffer injury compared to players without injury.
By tracking injuries over a period of seven seasons, researchers found that football players who suffered a concussion were also about 1.5 times more likely to be injured again in the future, compared to players who were never injured. This increased risk was the same as in players returning from upper and lower limb injuries.
The finding comes ahead of the Australian Senate report on concussions and follows the AFL’s announcement of a $25 million study into the long-term effects of concussions and head impacts.
In the AFL, concussions are one of the most common injuries, with an average of six concussions per 1000 hours of play, affecting approximately 70 to 80 male players annually.
In elite junior football, as well as AFL and AFLW, concussion guidelines state that the earliest a player can return to play after concussion is 12 days after the injury, after following gradual progression through a return-to-play -program.
Lead researcher Dr. UniSA’s Hunter Bennett says the significant and increased risk of injury following concussion may indicate that some players may need a longer recovery time to recover better before returning to play.
“The current recommendation of 12 days after concussion may not be sufficient to allow full recovery in elite football players under the age of 18,” says Dr Bennett.
It may also indicate that the physical attributes affected by concussion need to be more thoroughly assessed before an athlete is cleared to return to sport.
“Concussion is a common injury in Australian football and can lead to limitations in balance, coordination, reaction time and decision-making – and these limitations can increase the risk of other injuries if an athlete returns to play before full recovery.”
A recent consensus statement on concussions in sports also indicates that children and teens may take up to four weeks to recover from a sports-related concussion.
“Concussion is a unique injury that occurs without damage to muscle tissue but affects aspects of motor control,” says Dr. Bennett.
“Recurring injuries can have a significant impact on team success, player health and career longevity.
“In elite sport, there is a possibility that young athletes may exaggerate their willingness to return to sport after injury because they worry that missing matches could exclude them from senior drafting or competition.
“Knowing that athletes are at greater risk of re-injury after a concussion suggests that we need unique and careful rehabilitation strategies to monitor when an athlete has fully recovered and is ready to return to play.”
Researchers say future research should aim to identify optimal rehabilitation and injury prevention strategies for athletes who suffer from concussions.
Does headgear prevent sports-related concussions? A systematic review and meta-analysis of randomized controlled trials involving 6311 players and 173,383 exposure hours.
Al Attar WSA, Mahmoud H, Alfadel A, Faude O. Sports health. May 19, 2023: 19417381231174461. doi: 10.1177/19417381231174461. E-publishing prior to printing. PMID: 37204092.
Full text not freely available
Take home message
Headgear worn by young football or rugby players cannot reduce the incidence of sports-related concussions.
Background
Protective headgear reduces the risk of facial and dental injuries; However, there is inconsistent research supporting the rate at which they prevent sports-related concussions.
Study aim
In this systematic review, the authors identified and summarized findings from three randomized control trials evaluating whether headgear effectively reduces the incidence of sports-related concussions.
Methods
The authors systematically searched five databases to identify randomized control trials that evaluated the extent to which headgear prevented sports-related concussions. All control groups wore no headgear. The authors recorded exposure hours and number of players to calculate injury rates and document compliance.
Results
The 3 studies had an ‘average’ to ‘good’ methodological quality on the PEDro scale. The primary outcome assessed in each study was the rate of sports-related concussions per group (headgear vs. no headgear/control). The aggregated results include 6,311 players and 173,383 exposure hours. The authors found that headgear did not prevent concussions in football or rugby. Compliance was variable between studies (99.6%, 46% and not measured in one study).
Viewpoints
The authors of this systematic review concluded that the risk of sports-related concussion was virtually identical in the group with or without headgear. It should be noted that the rugby trials exclusively involved young men. While the football trials involved women, the study focused on 14- to 16-year-olds. Therefore, it is unclear how headgear performs among older athletes and female rugby players. The authors also found that compliance was quite variable. One football study had high adherence, while one rugby study had low adherence. It would be useful to understand whether differences in compliance are related to different strategies to promote compliance, differences in sport, or personal preferences for headgear styles. Understanding what worked in football but not in rugby could help identify strategies to promote good compliance.
Clinical implications
Medical professionals should not promote the wearing of headgear for football and rugby athletes to prevent concussion. Instead, medical professionals should promote concussion education on what can prevent a concussion, such as proper form (e.g., keeping head up while dribbling/being aware of surroundings) and proper tackling technique in rugby (e.g., not using head). .
Questions for discussion
Do you encourage headgear in sports such as football and rugby? Does this systematic review change your position? Why or why not?
related posts
Headgear can reduce concussion risk in high school lacrosse
Aftermarket helmet add-ons don’t add up
Women are not only at increased risk for concussions, but also for more severe concussions
A Closer Look at Concussions 2016-2020: Increasing Prevalence and Gender Differences
Written by Jane McDevitt
Reviewed by Jeffrey Driban
Over the past two decades, more and more states have provided patients with pain with direct access to physical therapy without a physician referral. Although the state of Arizona has offered this type of access for several years, insurance companies have only recently begun paying for physical therapy without a doctor’s referral. Direct access is just one of many reasons why you should look into physical therapy first. There are many more.
There is increasing data showing that seeing a physical therapist first can reduce costs and improve the overall outcome of injury rehabilitation. The American Physical Therapy Association (APTA) just published a groundbreaking study: ‘The economic value of physical therapy in the United States,’confirming that physical therapy (PT) can help Americans live better lives while saving the healthcare system millions of dollars annually.
Historically, the process from injury to recovery has involved seeing a doctor, trying medications, receiving diagnostic imaging, resting, and hoping for a resolution. If the problem was not resolved, the next step was to try physical therapy and perhaps some type of medical intervention such as injections or surgery. However, due to the rising costs of medical care, insurance companies and patients have started looking for methods to reduce the costs of rehabilitation. One of these methods is to first try PT for musculoskeletal problems.
Top three reasons to seek PT for pain first
1. Reduce or eliminate pain without drugs or opioids.
Physiotherapy offers the opportunity to reduce or eliminate pain through specific therapeutic exercises and hands-on manual therapy techniques. Additional treatments such as ultrasound, electrical stimulation, and taping techniques can also reduce pain during recovery.
Physiotherapy has come a long way in the past 20 to 25 years, as have the patients it helps. Due to costs and other factors, the goal now is to solve the problem as quickly as possible with as little use of health care as possible. PT allows the therapist to treat the cause of the pain early and begin rehabilitation by restoring the correct mechanisms that may be causing the pain.
A 2018 study analyzed 200,000 commercial and Medicare Advantage insurance beneficiaries seeking treatment for low back pain. It found that those who were initially referred by a physical therapist, chiropractor, or acupuncturist, compared to those who had an index visit by a primary care provider, reduced the likelihood of early opioid use by 85%-91% and long-term opioid use by 73% reduced. %-78%.
2. Savings on diagnostics
Being able to go straight to physiotherapy is cost-effective. For example, a patient avoids paying to see a doctor for a referral, and the doctor may order expensive diagnostic tests before determining that PT is the appropriate treatment method. A qualified therapist will work to avoid unnecessary diagnostics during your recovery, which can increase out-of-pocket costs and affect your long-term well-being. They will also work with your doctor to explore pre-surgery, post-surgery, and non-surgery options for a full recovery.
If physical therapy can address the reasons contributing to the pain, in many cases you can avoid surgery altogether. If you do need surgery, preoperative physical therapy can improve mobility and strength and help you get into better shape, allowing you to recover from surgery faster and with better results more easily with postoperative physical therapy.
When we look at patients who went to physical therapy first, there was an average savings of over $250 in one study and over $1,000 in another. Overall, there were significant savings across the board with less imaging, less medication, and even less treatment.
3. Improve mobility.
If you have difficulty standing, walking, or with transitions, such as moving from a sitting to a standing position, exercises to improve flexibility and strength can improve your ability to move more easily, making daily activities more enjoyable. Physical therapists can help you identify areas where you’re not moving correctly, predisposing you to future injuries, and correcting those movements to keep you injury-free. A PT can also instruct and fit you for an assistive device such as a cane, crutches, or other aids designed to improve your mobility.
PTs are also trained to recognize when physical therapy is needed not the correct or best first course of action and can point patients in the best direction. The physician-PT team is still the standard in treating musculoskeletal problems and guiding people with pain to a full recovery.
The search for full recovery is a journey without shortcuts and without a finish line. A journey that will lead to astonishing and satisfying results. At Foothills Sports Medicine Physical Therapy, our therapists embrace the journey. We take you, your pain and your full recovery seriously and do not believe that a good enough recovery is good enough. We strive to do everything we can to help you regain your full, healthy life.
If you have questions about immediate access to physical therapy, contact the Foothills Sports Medicine Physical Therapy clinic nearest you and schedule a free pain assessment.
Hockey leagues in Canada should revise current rules and regulations to raise the age for body checking in the game from 13 to 15, says new research into the effect of body contact on teens.
The literature search was led by Dr. Kristian Goulet of the University of Ottawa’s Faculty of Medicine and the Children’s Hospital of Eastern Ontario (CHEO) calls on provincial and territorial governments to mandate schools – including those involved in school sports – and sports organizations to establish policies and protocols set, update and enforce to prevent concussions, with a sharp emphasis on body contact.
Currently, hockey organizations in Canada allow body contact in competitive and recreational leagues from the age of 13. But studies have shown that when body contact is initiated, injuries increase significantly, including concussions.
Nearly half of hockey injuries are caused by body checks, with injury rates four times higher for children and teens in leagues where body checks are allowed. Other studies have shown that concussions are reduced by more than 50% when body contact is eliminated. An estimated 200,000 concussions occur in Canada each year, mainly affecting children and youth. Ice hockey is the leading cause of all sports and recreation-related brain injuries in pediatric age groups, in both boys and girls.
Dr. Goulet is hopeful that this review will prompt Hockey Canada to forge a new path forward to strengthen our understanding of concussion and guidance for clinical management, especially as it relates to acute care, ongoing symptoms and prevention.
“Sports are incredibly important to the mental, physical, emotional and social health of our children. However, it is our duty as caregivers, parents, coaches, administrators and decision makers that we make every reasonable effort to make sports as safe as possible,” says Dr. Goulet, an assistant professor at the Ottawa School of Medicine and the medical director of the CHEO Concussion Clinic, the Eastern Ontario Concussion Clinic and the Pediatric Sports Medicine Clinic of Ottawa.
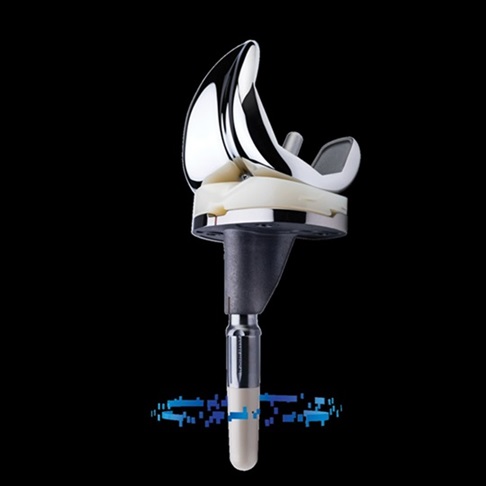
BALTIMORE , Oct. 26, 2023 /PRNewswire-PRWeb/ — Orthopedic surgeons Marc W. Hungerford, MD, Chief of Orthopedics at Mercy Medical Center, and Philip Neubauer, R.Ph., MD, Orthopedics and Joint Replacement at Mercy, are among the first surgeons in Maryland that offered “smart implant” technology during knee replacement surgeries.
Developed by ZIMMER BIOMET, the Persona IQ® has a small “smart” stem extension attached to the lower portion of the implant. This stem contains sensors that record patient-specific movement data throughout the day, analyze it overnight and present it for assessment the next day.
“Essentially, it is a joint replacement that uses a prosthesis equipped with a smart device that can monitor the patient’s progress,” said Dr. Hungerford.
Surgeons and care teams can remotely access key postoperative metrics throughout their patient’s surgical journey, allowing them to monitor post-TKA (Total Knee Arthroplasty) activity levels between office visits.
The smart knee implants provide a direct view of patient-specific data for at least 10 years, allowing surgeons to monitor their patients’ activity levels between visits. In this way, they can remain connected during the patient’s postoperative total knee arthroplasty care.
Additionally, being able to track their postoperative data can help patients feel more connected throughout their recovery journey, promoting greater patient interaction.
“Thanks to this new technology, there is greater patient involvement and surgeons can remotely monitor a patient’s progress. This means better management of postoperative care,” said Dr. Hungerford.
“With the Persona IQ, as a doctor I can no longer just estimate how well a patient’s joint is working after surgery; I have the data to determine how my patient is really doing,” said Dr. Neubauer.
“Mercy is always looking for ways to improve our patients’ experiences and treatment outcomes,” said Dr. Hungerford, “whether it be an emphasis on pre-surgical education, improvements to surgical pathways or advances in techniques and equipment. The smart implants offer real benefits for post-operative care, and we look forward to sharing them with patients.”
Founded in 1874 by The Sisters of Mercy, Mercy is home to the renowned Weinberg Center for Women’s Health & Medicine and the $400+ million, twenty-story Mary Catherine Bunting Center. Mercy is a university-affiliated teaching hospital and is nationally recognized with Magnet status for nursing excellence and named one of America’s 100 Best Hospitals for Orthopedic Surgery by Healthgrades. For more information about Mercy, visit http://www.mdmercy.com, MDMercyMedia on Facebook and Twitter(X), @MDMercy on Youtube, or call 1-800-MD-Mercy.
Media contact
Dan Collins, Mercy Medical Center, 4103329714, dcollins@mdmercy.com
Effect of the FIFA 11+ injury prevention program in collegiate female soccer players over three consecutive seasons.
Magoshi H, Hoshiba T, Tohyama M, Hirose N, Fukubayashi T. Scand J Med Sci Sports. May 21, 2023. doi: 10.1111/sms.14379. E-publishing prior to printing.
https://pubmed.ncbi.nlm.nih.gov/37211876/
Take home message
Over three seasons, injury prevention programs effectively reduce lower extremity injuries, especially those considered non-contact or moderate-severe.
Background
Injury prevention programs reduce the risk of lower extremity injuries. However, most studies have only examined the effectiveness of these programs over one season. It would be useful to verify whether these benefits persist if a team continues to implement an injury prevention program for multiple seasons.
Study aim
The authors conducted a non-randomized controlled trial to investigate the effectiveness of an injury prevention program (FIFA 11+) to reduce the risk of injury for up to three seasons among football teams in the Kanto University Women Football Association Division 1 (similar to NCAA Division 1).
Methods
Four teams agreed to run the FIFA 11+ program for 20 minutes before practicing 2-3 times a week. Three teams refused to agree to the program and represented the control group. Each team’s athletic trainer or physiotherapist recorded sports-related injuries, participation in training/matches and how often a team completed FIFA 11+. The authors defined a sports injury as an injury that causes a player to miss at least one day of training or competition.
Results
Adherence to the FIFA 11+ program was high (~88%). Compared to the other teams, the teams implementing the FIFA 11+ program have reduced the number of new injuries in a season by 36 to 61% – especially for non-contact, moderate or lower extremity injuries. Teams running FIFA 11+ may achieve better results each subsequent season (e.g. lower rate of new injuries in Season 2 versus Season 1), but this may be mainly due to the athletes who were on each team all three years.
Viewpoints
This study adds to the many previous randomized clinical trials showing that injury prevention programs reduce the risk of lower extremity injuries within a single season. This study provides good evidence that injury prevention programs can be effective over three seasons, especially for athletes who complete the program for all three years. It would be interesting to see the incidence of injuries in male football players and other sports associated with lower extremity injuries. Furthermore, it would be useful to confirm these results with a cluster-randomized clinical trial with a larger sample size to verify that athletes who perform FIFA 11+ continuously over multiple seasons experience greater protective benefits each year. Based on this research, it is unclear whether the benefits are due to the very high compliance rates (~88%), which is likely because teams actively decided to start the FIFA 11+ program rather than being randomly assigned to complete it program to execute. This highlights a major benefit of convincing a team to implement these programs.
Clinical implications
Clinicians should recommend that teams incorporate injury prevention programs into weekly team activities.
Questions for discussion
We often hear that a lack of time or coaching support for these programs is a barrier. WWhat are some strategies we can implement to combat this problem?
Would incidence remain low with a once-a-week approach if maintained during the off-season?
related posts
Coach the coach, make ACL injury prevention programs stick!
Injury prevention warm-up programs, one size fits some?
Back-to-school injury prevention programs
Forget about 7 minutes of Abs. What about the 10-minute lower extremity injury prevention program?
Written by Shelly Fetchen DiCesaro
Reviewed by Jeffrey Driban
Dynamic versus static stretching are two common methods for warming up and improving flexibility, but they serve different purposes and are best suited for different situations. Understanding the right type of stretching before and after activity is essential to improve performance and prevent injuries. When young athletes engage in physical activity, they are often encouraged by coaches and parents to stretch prior to the activity. The aim is to prepare the muscles for exercise and reduce the risk of injuries.
Preparing the body for physical activity
A thorough warm-up is intended to prepare the body for physical activity by:
Increase in core body temperature
Stimulates blood flow to the arms and legs
Improving coordinated movement
Improving range of motion
Develop body awareness of joint position sense and movement
Using movement to increase the flexibility of muscles and tendons
Dynamic stretching:
Goal: Dynamic stretching involves moving your muscles and joints through a range of motion to increase blood flow, warm up your body, and prepare your muscles and joints for physical activity. It is usually used as part of a warm-up routine before exercise or vigorous exercise.
Technology: Dynamic stretching exercises are performed by actively moving your limbs and muscles without assuming a static position. These stretches mimic the movements you perform during your activity. Examples include leg swings, arm circles, walking lunges, high knees and butt kicks.
Goal: Static stretching is used to improve overall flexibility and lengthen muscles. It involves holding a stretched position for an extended period of time, usually 15-30 seconds or more, without any bouncing or dynamic movement. It is often used for a post-exercise cooldown or as part of a general flexibility routine.
Technology: Static stretching involves stretching a specific muscle or muscle group to the point of mild discomfort and holding the position without movement. Common static stretches include touching your toes while sitting, stretching your calf against a wall or a standing quad stretch.
Advantages:
Increases flexibility and range of motion.
Helps with muscle relaxation and stress reduction.
Best suited for cooldown or recovery after exercise.
To design dynamic stretching programs:
Exercise continuously, usually in rounds for a total of 10-15 minutes
Vary the program depending on the athlete’s level
Start slow and progress to faster and more advanced movements
Avoid movements that are too intense and tire the muscles.
Take in the whole body and imitate movements used in specific sports
To design static stretching programs:
Stay in one position per muscle group
Hold the stretch for 20-30 seconds
Repeat the stretch 2-3 times per muscle group
Treat all muscle groups used in the specific sport
When should you use dynamic versus static stretching?
Dynamic stretching: Use dynamic stretching as part of your warm-up routine before activities that require strength, speed or agility. It is especially useful for sports such as basketball, football or sprinting, which require explosive movements. Dynamic stretching ensures that your muscles and joints are ready for the demands of such activities.
Static stretching: Reserve static stretching for after your workout or as a separate flexibility routine. It helps improve overall flexibility and can be useful for activities such as yoga or Pilates. Static stretching can also be beneficial for relaxation and stress reduction.
Remember that stretching should be done safely and should not cause pain or discomfort. It is essential to warm up your body before doing static stretches to prevent injuries. Incorporating both dynamic and static stretching into your fitness routine can help you maintain optimal flexibility and reduce the risk of injury during physical activities.
For help designing a stretching program, contact a Foothills Sports Medicine Clinic near you and schedule an appointment.
Dublin, October 26, 2023 (GLOBE NEWSWIRE) – The report “Scoliosis Management – Global Strategic Business Report” has been added to ResearchAndMarkets.com’s to offer.
The global scoliosis treatment market will reach $3.8 billion by 2030
The global scoliosis treatment market, estimated at USD 2.8 billion in the year 2022, is expected to reach a revised size of USD 3.8 billion by 2030, with a CAGR of 4.1% over the analysis period 2022-2030.
This data includes an analysis of the Thoracolumbosacral Orthosis (TLSO) and related orthosis markets worldwide. It includes current, historical, and future annual sales figures in thousands of dollars for the years 2022 through 2030, along with percentage compound annual growth rates (%CAGR).
The analysis is segmented into different product types, including TLSO, Cervical Thoracic Lumbar Sacral Orthosis (CTLSO), Lumbosacral Orthosis (LSO), and Other Product Types. Furthermore, within these product types a distinction is made between the Pediatric and Adult segments.
Thoracolumbosacral orthosis (TLSO), one of the segments analyzed in the report, is expected to register a CAGR of 4.4% and reach $2.9 billion by the end of the analysis period. Growth in the Cervical Thoracic Lumbar Sacral Orthosis (CTLSO) segment is estimated at 3.7% CAGR over the next eight years.
The US market is estimated at $987.6 million, while China is expected to grow at a CAGR of 5%
The US scoliosis treatment market is estimated to reach USD 987.6 million by the year 2022. China, the second largest economy in the world, is expected to reach a projected market size of USD 422.1 million by 2030, at a CAGR of 5% over recent years. analysis period 2022 to 2030.
The data provides a 16-year perspective, breaking down the percentage of value sales for different geographic regions, including the US, Canada, Japan, China, Europe, Asia Pacific and the rest of the world, for the years 2014, 2023 and 2030 Finally, it provides a comprehensive analysis of the scoliosis treatment market, including annual sales figures from 2014 through 2030, and segmented analyzes for different geographic regions.
Other notable geographic markets include Japan and Canada, each expected to grow by 3.1% and 3.4%, respectively, over the 2022-2030 period. Within Europe, Germany is expected to grow at a CAGR of approximately 4.1%.
This comprehensive report also provides detail on the approaches that leading market competitors such as Aspen Medical Products, Bauerfeind AG and Boston Orthotics & Prosthetics are taking, providing invaluable insights that you as an executive can leverage.
What’s new?
Special discussions on the global economic environment and market sentiment
Coverage on global competitiveness and key market shares of competitors
Access to digital archives and a trademarked research platform
Free updates for a year
Access curated YouTube video transcripts of market sentiments shared by CEOs, domain experts and market influencers through interviews, podcasts, press statements and event keynotes
MARKET OVERVIEW
Scoliosis: An abnormal lateral curvature of the spine
Scoliosis Management/Treatment Options
COVID-19 is casting a shadow on the scoliosis treatment market
Competition
Scoliosis Management – Percentage Market Share of Key Competitors Globally in 2023 (E)
Competitive Market Presence – Strong/Active/Niche/Trivial for Global Players in 2023 (E)
Great startup ecosystem
Global market analysis and prospects
The global scoliosis management market will demonstrate steady growth driven by innovations and advancements
North America holds a leading position in the global scoliosis management market
ThoracoLumboSacral Orthosis (TLSO) dominates the market
AIS remains the primary disease type segment
Pediatric/adolescent as an important age group segment
Hospitals and ASCs claim leading share
Technological advancements as pulsating trends drive the scoliosis treatment market forward
Increase R&D activity to drive market expansion
Market restrictions
Market challenges
Recent market activity
GLOBAL BRANDS
MARKET TRENDS & DRIVERS
Rising prevalence of idiopathic and congenital scoliosis drives market growth
Spinal fusion surgery offers great opportunities
The demand for fusionless scoliosis surgery is increasing
Tying the vertebral body provides traction
Schroth therapy – a useful approach to treat scoliosis
Strong focus on minimally invasive spine surgery and increasing use of navigation and robotics in scoliosis surgery to increase prospects
Increasing cases of scoliosis in adults and a growing aging population to propel the adult segment
Increase healthcare spending to stimulate growth
Recent technological advances/innovations in the scoliosis treatment market
New Satellite Rod-Based Sequential Correction for Severe Rigid Spinal Deformities to Reduce Surgical Risks and Other Complications
ApiFix system for correcting moderate scoliosis with single curves
Shriners Hospitals for Children’s The Tether, a device for treating scoliosis, receives FDA approval
Minimally invasive spine surgeries are becoming commonplace, but long-term research into results is essential for wider adoption
Disruptive technologies in the spine space – a review
3D printed braces have potential to improve the treatment of scoliosis
FOCUS ON SELECTED PLAYERS(Total 91 recommended)
Aspen Medical Products, LLC
Bauerfeind AG
Boston Orthoses and prosthetics
Chaneco
Enovis
Fitted, Inc.
Horton’s Orthotics and Prosthetics
Lawall Prosthetics and Orthotics
Optec USA, Inc.
Orthotec
Ottobock SE & Co. KGaA
Spinal Technology Inc.
Real
For more information about this report, visit https://www.researchandmarkets.com/r/ozemky
About ResearchAndMarkets.com
ResearchAndMarkets.com is the world’s leading source for international market research reports and market data. We provide you with the latest data on international and regional markets, key industries, top companies, new products and the latest trends.
Post-stroke patients with motor dysfunction who were hospitalized in the Department of Rehabilitation Medicine of our hospital from January 1, 2020 to January 1, 2022, aged 50 to 70 years old, were selected.
Inclusion criteria: [12] ① The patient met the diagnostic criteria for stroke established at the Fourth National Academic Conference on Cerebrovascular Diseases in 1995, [13, 14] and stroke was diagnosed as the primary disease on CT or MRI. ② The time between disease onset and enrollment ranged from two weeks to three months. ③ The patient’s vital signs were stable and the patient was conscious, able to understand the instructions and cooperate with the rehabilitation training. ④ The patient’s score on the Kinesthetic and Visual Imagery Questionnaire (KVIQ) was ≥ 25 points. ⑤ The patient signed the required informed consent form. ⑥ Age between 50 and 70 years.
Exclusion criteria: [14] ① The patient suffered from severe cardiac, hepatic or renal insufficiency, a malignant tumor, etc. ② The patient suffered from impaired consciousness, aphasia, mental disorder or severe cognitive impairment. ③ The patient has had other craniocerebral diseases or traumatic sequelae in the past. ④ The patient has previous severe osteoarticular disorders causing abnormal trunk function.
Finally, a total of 100 patients with stroke and motor dysfunction were included, and they were divided into a control group and a trial group according to the random number table, with 50 cases in each group. There was no significant difference (P > 0.05) in general data such as gender, age, disease course and KVIQ between the two groups, and they were comparable. See Table 1 for details. This study was approved by the local ethics committee (approval number: 2018-ethical review-189) and conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Table 1 Comparison of general data of patients such as gender, age, disease course and lesion site between the two groups
Treatment methods
The patients in the control group underwent routine rehabilitation therapy and remained in the supine position in the same environment for the same amount of time as the combined trunk motor imagery therapy. Meanwhile, the trial group received both routine rehabilitation therapy and combined trunk motor imagery therapy.
Routine rehabilitation therapy
The training included proper limb positioning, neuromuscular promotion techniques, such as the proprioceptive neuromuscular facilitation technique (PNF), Rood’s approach, motor relearning, occupational therapy, daily living training and traditional therapy. The participants received routine rehabilitation therapy for five hours a day, five times a week, for a period of four weeks.
Motor image therapy
The motor imagery therapy training consisted of six steps: [4, 14] ① Illustration of the task: The therapist first demonstrated and explained the content of the imagery training, asking the patients to carefully observe and identify which part of the limb was ‘active’, what kind of movement was to be performed, and the normal movement to master. feeling. ② Preview: Patients were asked to re-imagine the relevant movements. ③ Motor imagery: Patients listened to the motor imagery instruction tape and practiced the imagery. ④ Rehabilitation training: the patients repeatedly practiced the movements of imagery training. ⑤ Problem solving: The patients learned relevant skills through repeated practice. ⑥ Practical application: the patients convert relevant skills into practical skills. Before the motor images, a video of a normal person’s trunk movements was shown, including stable trunk movements with a Bobath ball, and balance movements while sitting, standing, and reaching to move a water cup. The 10-minute video and audio were shown to patients via a computer in a quiet treatment room. During each training session, patients were instructed to close their eyes and sit on a comfortable chair with their bodies relaxed. The patients then imagined the movement of their body based on the specific motor imagery instructions in the video. During the treatment, the therapist occasionally interrupted the patients to ask questions, to see if they could concentrate on the images of the physical movement. At the end of the session, the patients were asked to refocus their attention on their surroundings, after which they were sent back to their room and asked to feel their physical being. The patients were then asked to pay attention to the environmental sounds. Finally, the narrator counted down from 10 to 1, and the patients were asked to open their eyes when the countdown reached 1. A motor imagery video was shown only during the first treatment, after which the patients underwent motor imagery training according to the motor imagery. guidelines for imagery. The motor imagery therapy sessions were conducted for 30 minutes each, with a frequency of five times per week, for a total of four weeks.
Observation indicators and evaluation methods
The evaluation of the patient’s trunk control was performed before treatment and four weeks after treatment using Sheikh trunk control evaluation. The simple Fugl-Meyer assessment (FMA), the Berg rating scale (BBS), and the balance feedback trainer were used to evaluate the motor and balance functions of the patients. In addition, before and after treatment, the sEMG signals of the bilateral erector spinae and rectus abdominis in the maximum flexion and extension range at a uniform speed under the sitting position were measured by sEMG signals. All evaluations were performed in a blinded manner by the same evaluator.
Sheik Hull Check Evaluation
Sheikh is a scale for evaluating the ability to control the trunk. It involves four movements: turning from the supine position to the hemiplegic side, turning to the healthy side, sitting upright from the supine position and maintaining balance in a sitting position on the bed. The scoring method is: 0 points for non-completion, 12 points for completion but needing some assistance (grasping or leaning on an object), and 25 points for normal completion. A higher total score indicates better trunk control.
BBS rating
The balance function is divided into 14 items, from easy to difficult, and each item is scored based on a five-point scale: 0, 1, 2, 3, and 4. The highest score is 4 points and the lowest score is 0 points. . The highest integral score is 56 points, the lowest is 0 points. The higher the score, the better the balance function.
Evaluation of motor functions
FMA is used to evaluate motor function in patients. The highest score is 100. The higher the score, the better the patients’ motor functioning will be.
Evaluation of balance feedback training equipment
The ProKin 254P (PK-254P) balance feedback training device, manufactured by TecnoBody Ltd., Italy, was used to test the postural stability of the patients. Stability tests were performed in standing position with eyes open using the static mode of the PK-254P balancer. The standard standing posture includes: ① Bilaterally symmetrical standing with A1A5 as central axis. ② The patients raise their heads and look straight ahead. ③ Both upper limbs are naturally placed on either side of the body. ④ The medial edges of both feet are 10 cm apart and the highest point of the bilateral arches is on axis A3A5. Observation parameters are as follows: movement length, movement area, mean front-back movement speed, and mean left-right movement speed.
sEMG signal acquisition
While the patients are seated on a square stool, their trunk is subjected to anterior flexion and posterior extension in the maximum range at uniform velocity. The Shanghai NCC 8-channel sEMG signal acquisition system was used to acquire the bilateral erector spinae and rectus abdominis myoelectric signals. The electrodes were taped to the 3 cm lateral opening on the left and right sides of the L3 spinous process (erector spinae) and the 3 cm lateral opening on the left and right sides 3 cm above the navel (rectus abdominis). The conductive diameter of the electrodes was 1 cm and the distance between the electrodes was 2 cm. Dandruff and oil were removed with a fine gauze and alcohol before testing. The root mean square (RMS) of myoelectric signals was then analyzed. The test was repeated three times with an interval of 30 seconds to obtain the average value. The RMS of the bilateral rectus abdominis and erector spinae of the two groups was evaluated before treatment and four weeks after treatment.
static analysis
SPSS software version 16.0 was used to analyze the data. The measurement data is expressed as (\(\bar x \pm s\)). Parametric statistics were applied when the data collected met the assumptions of homogeneity of variance and normal distribution. When these assumptions were not met, non-parametric statistics were used. The paired sample T-test was used for pre- and post-treatment comparison within the same group, while the independent sample T-test was used for between-group comparison, and P< 0.05 indicated that the difference was statistically significant.