The Bone Health & Osteoporosis Foundation (BHOF) is currently collecting written stories as part of a support initiative called Voices of Osteoporosis: Stories of Hope and Inspiration.
If you have experienced osteoporosis as a patient or caregiver, we invite you to share your story. Your story can inspire others to learn how to protect their ability to live their best life and stay strong.
If you are interested in participating in this initiative, please contact us click here to complete a short interest form online. A BHOF representative will then contact you to answer any questions you may have and coordinate the time frame for your submission.
Below are some important details about participating in this initiative:
Examples –click here for a few sample stories that others have shared before: if you scroll down the page, you’ll see some listed and you can click on each story to expand it.
Length – We request that all stories be submitted in a Word document; stories must be written in the first person and are typically about 800 words long.
To process – BHOF only very minimally, if at all, edits each person’s story because we want it to come directly from each person as his or her own lived experience.
Title – Add an inspiring title to your story.
Photos – We request that you submit 2-3 photos of yourself along with your story. At least one of the photos must be horizontal, as it will be placed as the main image at the top of your story web page. The ideal size for the horizontal image is 1400×600.
Release form – Once you complete the online interest form, a BHOF representative will contact you to answer any questions you may have and coordinate the time frame for your submission. At that time they will also ask you that sign this release form and send it back before sharing your story.
Process & BHOF Contact – You can forward all articles to your BHOF contact person by e-mail. They will also help you with any questions you may have throughout the process.
Share your story – Your story may be shared through a variety of channels including the Bone Talk blog, the BHOF website, email communications and social media.
Do you have questions? Your BHOF contact will be happy to help you every step of the way!
by Danielle Dupont, PT, DPT, RRS, NASM-CNC – North Central Phoenix
Whether you’re a seasoned marathon runner or just starting your fitness journey, running and physical therapy can play a crucial role in optimizing your performance. PT can also help prevent injuries and promote overall well-being.
Top 10 Reasons Why Runners Should Seek a Physical Therapist:
Injury prevention: Physical therapists can assess your running biomechanics and identify potential problems that could lead to injuries. They can provide personalized advice and exercises to address weaknesses, imbalances or poor running form. Reducing the risk of injuries such as shin splints, stress fractures or runner’s knee.
Rehabilitation: If you have already suffered a running injury, physical therapists can tailor a rehabilitation program to help you recover safely and quickly. They use evidence-based techniques to restore strength, flexibility and range of motion. This allows you to start running again with less risk of new injuries.
Performance improvement: Physical therapists can work with you to improve your running efficiency and technique. They can identify areas where you can improve your stride, posture and gait so you can run faster and with less effort. This can be especially valuable for competitive runners who want to achieve personal bests.
Custom training plans: Physiotherapists can develop personalized training plans that take into account your individual strengths and weaknesses. This can help you avoid overtraining and make safe progress toward your running goals.
Pain Management: If you experience persistent pain during or after running, a physical therapist can provide pain relief strategies such as manual therapy, modalities such as ultrasound or electrical stimulation, and education on self-care techniques.
Biomechanical analysis: A physical therapist can perform a comprehensive assessment of your walking biomechanics. This may include analyzing your footstep pattern, joint movements and muscle activation to recommend appropriate footwear, orthotics or exercises to optimize your walking mechanics.
Postoperative rehabilitation: If you have had surgery for a running injury, physical therapists can guide you through postoperative rehabilitation to ensure a successful recovery and a gradual return to running.
Education and guidance: Physical therapists can educate you on proper warm-up and cool-down techniques, stretching exercises, and injury prevention strategies. They can also give you advice on how to adjust your running program as you get older or encounter new challenges.
Motivation and support: Building a strong relationship with a physical therapist can provide the motivation needed to continue your rehabilitation. They can encourage and support you as you work toward your running goals.
Whole body health: Physiotherapists take a holistic approach to health, taking into account the impact of various factors on your running performance. Including nutrition, sleep and stress management. They can guide you in optimizing these aspects of your life to support your running efforts.
Physiotherapists are movement experts who improve the quality of life through practice-oriented care, patient education and prescribed movement. Seeking the expertise of a physical therapist can be extremely helpful for runners of all levels. Whether you want to prevent injuries, improve performance, or recover from an injury, a physical therapist can provide personalized care and guidance to help you achieve your running goals safely and effectively.
Find a location near you for a free port analysis and tips to start your pain-free running journey.
You have been diagnosed with osteoporosis or osteopenia and told that exercise can help. But what kind of exercise should you do? How do you know you won’t hurt yourself? What if you’ve never exercised before – how do you even get started? Or if you’re already an exercise enthusiast, what else can you do that you may have overlooked before?
Let’s start by identifying how exercise can benefit your bones. Your bones are living tissue that change thickness, mass and shape with use, just like your muscles. If you wanted to strengthen your muscles, you would use them by pulling objects (like lifting weights) and pushing things (like push-ups). You can strengthen your bones in much the same way.
Your bones adapt and respond to loads by strengthening and strengthening themselves to be able to bear that same load again in the future. When you resist external forces like gravity or weights, your bones reap the reward. On the other hand, not using your bones results in a weakening of their structure and composition. Ever seen the wrist of someone whose cast has just been removed? The wrist size has generally become smaller compared to the other wrist due to its immobility and lack of use. Similarly, NASA research has shown how the absence of gravity in space, which also limits the ability of muscles to pull on bones, causes reductions in bone mass.
To know which type of exercise to engage in, you need to understand that bone is built from three sources when it comes to activity:
1–Weight load
Every time you stand upright, you are working against gravity and supporting the weight of your body. When you crawl or exercise on the floor and support your body with your hands and wrists, you similarly support your weight through your forearm bones.
2–Resistance
Your muscles facilitate movement against additional forces such as weights, bands or pulleys when you exercise. They also contract during daily activities such as carrying objects and moving furniture.
3–Effect
Your bones respond to compressive forces and receive further stimuli to become stronger when a greater force is added that increases the gravitational effect. You’re probably familiar with the term “high impact,” which refers to activities like running and jumping that some people find uncomfortable on their joints as they get older. High impact may not be recommended if you have osteoporosis, and especially if you have had a fracture, but it is important for building maximum bone mass in younger individuals. Low impact can be achieved by repeatedly stomping your feet or dropping your heels.
Knowing which exercises to perform – and even which type of exercise (strength training, Pilates, yoga, HIIT, aerobics, to name a few examples) – depends on your physical capacity, history of physical activity and history of fractures . (If you have had a fracture, you should get permission from your doctor to begin an exercise program.)
To actually increase bone density through exercise after menopause, you probably need high-intensity exercise (lifting heavy weights with a load of at least 80% of the maximum you can lift in a single repetition, along with a high impact). That assumes you don’t have any comorbidities (other conditions) or safety concerns that could make it contraindicated, and you have access to a gym and a trainer to supervise you.
You can also aim to maintain the bone density you have, train for strength and power, and absorb impact at lower loads. No matter what, to avoid injuries, maintain good form by mastering basic movements and training for mobility to achieve the necessary range of motion in your joints.
So when the question arises as to what is the one form of exercise you should be doing for osteoporosis, there is not ONE! The three bone-strengthening elements mentioned above are essential in addition to mobility training, but as the 2014 consensus document ‘Too Fit to Fracture’ pointed out, the best strategy is a multimodal approach that also combines balance and posture training (which we will discuss in this article). a future part of this series.)
A few important things to keep in mind as you begin your training journey:
Be consistent. As with any activity or skill, consistency is key to experiencing results and promoting motivation
Keep challenging yourself. Your bones and muscles are both adaptive organs. So to continue to reap the benefits of exercise, you need to continually and gradually make things harder so you don’t plateau.
Make it fun. If you find it annoying, you’re more likely to procrastinate and avoid it! The best exercise is the one you are going to do.
Sometimes getting started is the biggest hurdle you have to overcome. Know that exercise affects more than just your bones and muscles, joints and soft tissues. It is multisystemic and can improve other systems of your body, such as your digestion, your circulation and your cognition. Furthermore, the more physically active you become, the stronger you feel. One of the often overlooked aspects of osteoporosis is the emotional difficulty that patients experience, regardless of whether they have suffered a fracture. Taking charge of your health through exercise can be one of the best actions you can take to transform yourself from a sense of fear and vulnerability to a sense of confidence and capability.
Stay tuned for the next part of this series demonstrating specific posture training exercises that you can incorporate into your daily life. The smallest change in body position can make a big difference in the experience and effects of your exercise program.
A few weeks ago I worked virtually with a client who was 10 weeks post-surgery. We had started working together around week 3 and so far he had absolutely dominated the recovery process.
In addition to his physical therapy appointments, he would meet with me virtually once a week to determine the best plan of attack for his workouts with the Neubie… and then he would get after it. By incorporating our recommended workouts with the Neubie 3x per day into his routine, he regained full strength and range of motion before 8 weeks post-surgery.
But around week 10, they started increasing the load at his physical therapy appointments. In particular, they started trying to increase the weight of his exercise on the knee extension machine, which led to a bit of pain in the front of the knee. Each day he returned to do the knee extensions, the pain in the front of his knee increased.
As I mentioned earlier, this client met with me once a week, and by the time we met again, he had reached a point where the pain continued even in his daily activities. He no longer had the ability to fully extend the knee without pain.
Despite doing everything right and botching the first eight weeks of the recovery process, he experienced a setback in week 10.
Setbacks can be difficult, but with the right strategies you can overcome them quickly and emerge stronger.
WARSAW, Ind., October 19, 2023 (GLOBE NEWSWIRE) —Orthopediatrics Corp. (“OrthoPediatrics”) (NASDAQ: KIDS), a company focused solely on advancing the field of pediatric orthopedics, today announced that it has released the new Pediatric Nailing Platform TIBIA System and has successfully completed the first cases of the limited launch has completed. The company received 510(k) clearance from the U.S. Food and Drug Administration (FDA) for the system in September 2023.
PNP Tibia is part of the Trauma & Deformity Correction product range and represents another pediatric-focused solution for the treatment of patients with lower extremity fractures and deformities. It expands the company’s offering to 52 unique systems specifically designed to help address the needs of pediatric patients. The PNP tibial system features rigid cannulated nails ranging in diameter from 7 mm to 12 mm and includes specialized instrumentation to facilitate multiple surgical techniques. Like other OrthoPediatrics products, this system is designed for the anatomy of children and growing patients.
The versatility and scope of the PNP Tibia System were on full display in these two surgical cases. One case was a trauma procedure for a 6-foot teenager requiring a large nail (12mm x 420mm), while the other was a deformity correction procedure for a 15-year-old of smaller stature requiring a 7mm x 285mm was used. These two cases reflect that OP has the broadest scope of pediatric-focused cannulated nails in the industry, allowing surgeons to treat children of all sizes and needs.
Joe Hauser, president of OrthoPediatrics Trauma & Deformity Correction, said: “It is extremely gratifying to see the system perform successfully in two unique and challenging cases. It shows that the surgeon’s expert design team together with the OP engineers have achieved a goal in designing a system that will help many children for years to come.”
About OrthoPediatrics Corp.
Founded in 2006, OrthoPediatrics is an orthopedic company focused exclusively on advancing the field of pediatric orthopedics. As such, it has developed the most comprehensive product offering for the pediatric orthopedic market to improve the lives of children with orthopedic conditions. OrthoPediatrics currently markets 52 systems serving three of the largest categories within the pediatric orthopedic market. This product offering includes trauma and deformity, scoliosis and sports medicine/other procedures. OrthoPediatrics’ global sales organization focuses exclusively on pediatric orthopedics and distributes its products in the United States and more than 70 countries outside the United States. For more information, please visit www.orthopediatrics.com.
Contact person for investors
Philip Trip Taylor
Gilmartin Group
philip@gilmartinir.com
415-937-5406
All participants (demographic and anthropometric data are shown in Table 1) successfully completed the experimental sessions without side effects, except for some cases of mild tingling in the fingers at the end of the measurements. Regarding RTD, three men had to be excluded from the data analyzes because the occlusion of arterial blood flow was not possible with the MS and/or LS cuff due to the painful pinching of the skin fold and the stretching of the cuff up to the yield point. In addition, one female was excluded from data analyzes for vsysRPP, SMO2and tHb because arterial blood flow was already occluded at 20% overlap using the HS cuff.
Table 1 Participant characteristics expressed as means ± standard deviations
Overlap to occlusion
There was a main effect of cuff (F2.62 = 175.679, P< 0.001, theP2= 0.850) and post hoc analysis indicated that RTD was lower in the HS compared to the MS (MD = -13.06% (-16.18 to -9.93%), P< 0.001, D= 2.06) and LS cuff (MD = -23.78% (-26.90 to -20.65%), P< 0.001, D= 3.75). In addition, RTD was also lower using the MS compared to the LS cuff (MD = -10.72% (-13.85 to -7.60%), P< 0.001, D= 1.69). Descriptive data are shown in Table 2; Fig. 3.
Table 2 Hemodynamic, physiological and perceptual responses to progressive practical blood flow restrictions (10%, 20% and 30% overlap relative to the individual’s upper arm circumference) using a high stiffness (HS), medium stiffness cuff ( MS) and low stiffness (LS). Data are expressed as means ± standard deviations
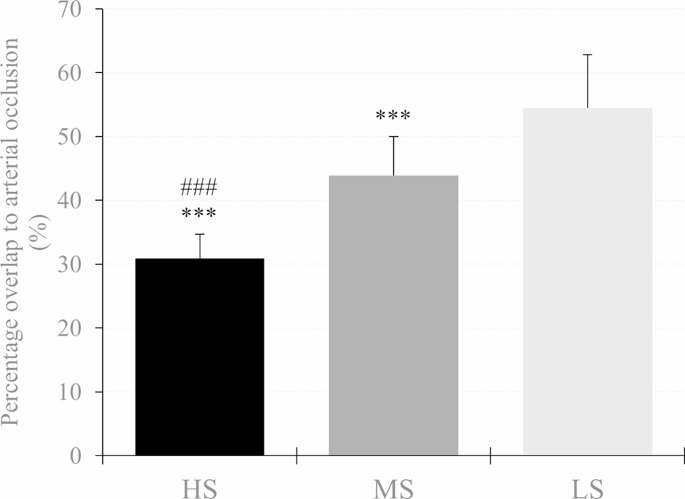
Fig. 3
Percent overlap needed for arterial occlusion in the high stiffness (HS), medium stiffness (MS), and low stiffness (LS) cuff. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ### p < 0.001 respectively
Peak systolic velocity of blood flow
There was an overlap × cuff interaction (F3,642,120,192 = 71.952, P< 0.001, theP2= 0.686) and a main effect of overlap (F1,770,58,422 = 161.427, P< 0.001, theP2= 0.830) and cuff (F2.66 = 50.380, P< 0.001, theP2= 0.604) for vsys. Post hoc analysis showed that vsys was lower at 30% overlap in each cuff compared to baseline (HS: MD = -62.67 cm s− 1(-70.97 to -54.37 cm s− 1 ), P< 0.001, D= 3.95; MS: MD = -21.53 cm s− 1(-29.83 to -13.24 cm s− 1 ), P< 0.001, D= 1.36; LS: MD = -11.02 cm s− 1(-19.31 to -2.72 cm s− 1 ), P< 0.001, D= 0.69). Furthermore, when the HS cuff was applied, vsys was also lower at 20% overlap compared to baseline (MD = -20.51 cm s− 1(-28.80 to -12.21 cm s− 1 ), P< 0.001, D= 1.29). As for cuff differences, vsys was lower at 20% and 30% overlap using the HS cuff compared to the MS (MD = -16.89 cm s− 1(-26.08 to -7.70 cm s− 1 ), P< 0.001, D= 1.07 and MD = -39.91 cm s− 1(-49.11 to -30.71 cm s− 1 ), P< 0.001, D= 2.52, respectively) and the LS cuff (MD = -17.60 cm s− 1(-26.80 to -8.41 cm s− 1 ), P< 0.001, D= 1.11 and MD = -53.99 cm s− 1(-63.18 to -44.79 cm s− 1 ), P< 0.001, D= 3.40 respectively). Furthermore vsys was also lower at 30% overlap using the MS compared to the LS cuff (MD = -14.08 cm s− 1(-23.27 to -4.88 cm s− 1), P< 0.001, D= 0.89). Descriptive data are shown in Table 2; Fig. 4.
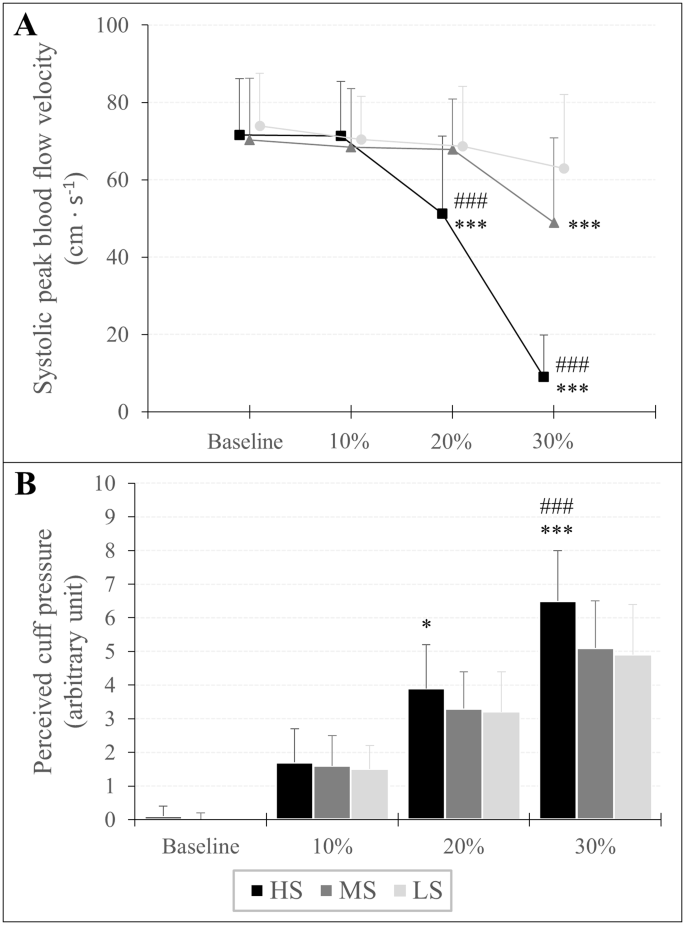
Fig. 4
Peak systolic velocity of blood flow (A) and assessment of perceived cuff pressure (B) in response to progressive practical pressure on blood flow restriction, expressed as percent overlap in relation to the individual’s arm circumference. A significant difference between LS and MS is shown as *p<0.05, **p < 0.01, ***p < 0.001 and #p<0.05, ##p < 0.01, ###p < 0.001 respectively
Assessment of perceived cuff pressure
An overlap × cuff interaction (F3,946,130,209 = 13.994, P< 0.001, theP2= 0.298) and a main effect of overlap (F1,668,55,046 = 674.771, P< 0.001, theP2= 0.953) and cuff (F2.66 = 11.067, P< 0.001, theP2= 0.251) was found for RPP. A post hoc analysis showed that RPP increased at each %overlap stage compared to baseline for all three cuffs (HS10%: MD = 1.57 au (0.98 to 2.17 au), P< 0.001, D= 1.51; HS20%: MD = 3.80 au (3.21 to 4.40 au), P< 0.001, D= 3.66; HS30%: MD = 6.41 au (5.82 to 7.00 au), P< 0.001, D= 6.16; MS10%: MD = 1.54 au (0.94 to 2.13 au), P< 0.001, D= 1.48; MS20%: MD = 3.32 au (2.72 to 3.91 au), P< 0.001, D= 3.19; MS30%: MD = 5.03 au (4.44 to 5.63 au), P< 0.001, D= 4.84; LS10%: MD = 1.46 au (0.87 to 2.05 au), P< 0.001, D= 1.40; LS20%: MD = 3.18 au (2.59 to 3.77 au), P< 0.001, D= 3.05; LS30%: MD = 4.95 au (4.36 to 5.55 au), P< 0.001, D= 4.76). Regarding differences between cuffs, RPP was higher using the HS cuff with 20% overlap compared to the LS cuff (MD = 0.71 au (0.06 to 1.37 au), P= 0.016, D= 0.69) and with an overlap of 30% compared to Member States (MD = 1.43 (0.78 to 2.09 au), P< 0.001, D= 1.38) and LS cuff (MD = 1.54 au (0.89 to 2.19 au), P< 0.001, D= 1.48). Descriptive data are shown in Table 2; Fig. 4.
Oxygenation of the muscles
SMO2: There was an overlap × cuff interaction (F2,374,78,326 = 3.232, P= 0.037, theP2= 0.089) and a main effect of overlap (F1,297,42,808 = 404,914.= P< 0.001, theP2= 0.925) and gender (F1.33 = 5.096, P= 0.031, theP2= 0.134) for SMO2. Post hoc analysis showed that SMO2 was lower at 20% overlap (HS: MD = -9.94% (-12.43 to -7.45%), P< 0.001, D= 1.15; MS = -8.28% (-10.77 to -5.78%), P< 0.001, D= 0.96; LS: MD = -7.42% (-9.98 to -5.00%), P< 0.001, D= 0.87) and 30% overlap (HS: MD = -17.46% (-19.95 to -14.97%), P< 0.001, D= 2.02; MS: MD = -14.91% (-17.42 to -12.42%), P< 0.001, D= 1.72; LS: MD = -13.79% (-16.28 to -11.30%), P< 0.001, D= 1.59) compared to baseline. Furthermore, the main effect of sex indicated that regardless of overlap and cuff used, SMO2 was lower in men than in women (MD = -5.16% (-9.80 to -0.51%), P= 0.031, D= 0.60).
tHb: An overlap × cuff (F3,072,101,386 = 6,440, P< 0.001, theP2= 0.163) and overlap × sex interaction (F1,187,39,158 = 14.814, P< 0.001, theP2= 0.310) and a main effect of overlap (F1,187,39,158 = 117,125.= P< 0.001, theP2= 0.780) and gender (F1.33 = 27.981, P< 0.001, theP2= 0.459) was found for tHb. Post hoc tests showed that tHb was higher at 20% overlap (HS: MD = 0.13 au (0.09 to 0.18 au), P< 0.001, D= 0.45; MS: MD = 0.10 au (0.05 to 0.14 au), P< 0.001, D= 0.32; LS: MD = 0.06 au (0.02 to 0.11 au), P< 0.001, D= 0.20) and 30% overlap (HS: MD = 0.22 au (0.18 to 0.27 au), P< 0.001, D= 0.75; MS: MD = 0.17 au (0.12 to 0.21 au), P< 0.001, D= 0.55; LS: MD = 0.15 au (0.10 to 0.19 au), P< 0.001, D= 0.45) compared to baseline. Moreover, tHb was already higher at a 10% overlap using the HS (MD = 0.05 au (0.00 to 0.09 au), P= 0.018, D= 0.16) compared to baseline. Regarding sex differences, post hoc analysis showed that regardless of cuff, tHb was higher by 10% (MD = 0.06 au (0.01 to 0.10 au), P= 0.003, D= 0.20), 20% (MD = 0.15 au (0.11 to 0.20 au), P< 0.001, D= 0.52) and 30% overlap (MD = 0.24 au (0.19 to 0.29 au), P< 0.001, D= 0.80) in men, while in women tHb was only higher during a 30% overlap compared to baseline (MD = 0.12 au (0.07 to 0.16 au), P< 0.001, D= 0.39). In addition, tHb was higher in men compared to women at baseline (MD = 0.51 au (0.31 to 0.70 au), P< 0.001, D= 1.69). Descriptive data are shown in Table 2.
Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion pain.
Corns and calluses on the friction site of the big toe and second toe
Limited movement of the big toe
What is a lapiplasty?
People often have the misconception that bunions can be fixed by just shaving off the bone, thinking it is an overgrowth. In reality, there are deeper issues that are causing the problems you are experiencing. In the past, bunion surgery approached the problem on a two-dimensional plane, while the problem to be addressed was three-dimensional. This is where Lapiplasty comes into play. With LapiplastyⓇ 3D Bunion Correction, instead of doing what traditional bunion surgery does, which is cutting the bone in half and shifting, Lapiplasty rotates the entire spine of the foot to repair the anatomical deformity that causes the bunions to form. By doing this, the chance of your bunions returning is minimal.
If you suffer from bunions, Bone and Joint Specialists Orthopedic & Spine Center is the right place for you. With 4 locations in Indiana, we offer extensive access to our physicians who can provide you with world-class service. Working with us means you work with the best. Contact us today at 219.795.3360 or visit us online at www.orthopedicdoctors.com to schedule your consultation.
It is usually normal for your knee to feel numb and tingly after ACL surgery. This is because some small nerves are cut during the surgical procedure. Don’t worry, we’re not talking about the really important nerves that allow you to bend and straighten your knee, but the nerves that allow you to feel things around your knee. This video below explains all the reasons why your knee may feel numb and tingly after ACL surgery. For more information, read this blog about 5 tips to help you recover after ACL surgery.
Lauren Youssef, a physiotherapy student at the University of Toronto, explains why your knee may feel numb and tingly after ACL surgery.
Read Lauren’s blog: Why is my knee numb and tingling after ACL surgery? | Curovat
There are also 5 great blogs written by Lauren on our site where you can learn more about surgery and injury recovery.
If you have had an ACL injury or surgery, download Curovate from the links below. Curovate is a physical therapy app that offers daily video-guided exercises, progress tracking, in-app chat with a physical therapist to answer your questions about surgery or injury, and the ability to measure your knee’s range of motion using just your phone.
If you need more tailored help during your surgery or recovery from your injury, check out our Virtual Physiotherapy page to book your 1-on-1 video session with a physiotherapist.
Other blogs related to ACL injuries:
References
1. Horteur, C., Cavalié, G., Gaulin, B., Cohen Bacry, M., Morin, V., Cavaignac, E., & Pailhé, R. (2020). Saphenous nerve damage after anterior cruciate ligament reconstruction: Decreased area of numbness after ligamentoplasty using the quadriceps tendon compared to the hamstring tendon. The Knee, 27(4), 1151–1157.
2. Inderhaug, E., Strand, T., and Solheim, E. (2015). The impact of sensory deficits after hamstring autograft harvesting for ACL reconstruction. Knee surgery, sports traumatology, arthroscopy: Official Journal of the ESSKA, 23(4), 1060–1064.
3. Kjaergaard, J., Faunø, L. Z., & Faunø, P. (2008). Loss of sensation after ACL reconstruction with hamstring graft. International Journal of Sports Medicine, 29(6), 507–511.
4. Nerve Blocks for Surgery – Yale Medicine. (2020, July 02). Retrieved from https://www.yalemedicine.org/conditions/nerve-blocks-for-surgery
5. Ochiai, S., Hagino, T., Senga, S., Yamashita, T., Oda, K., & Haro, H. (2017). Damage to the infrapatellar branch of the saphenous nerve in anterior cruciate ligament reconstruction using vertical skin incision for hamstring harvesting: risk factors and influence on treatment outcome. Journal of Orthopedic Surgery and Research, 12(1), 101.
6. Sanders, B., Rolf, R., McClelland, W., and Xerogeanes, J. (2007). Prevalence of saphenous nerve damage after autogenous hamstring harvest: an anatomical and clinical study of tailor branch injury. Arthroscopy: The Journal of Arthroscopic and Related Surgery: Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 23(9), 956–963.
7. Wang, H. D., Zhang, H., Wang, T. R., Zhang, W. F., Wang, F. S., & Zhang, Y. Z. (2018). Comparison of clinical outcomes after anterior cruciate ligament reconstruction with hamstring tendon autograft versus soft tissue allograft: a meta-analysis of randomized controlled trials. International Journal of Surgery (London, England), 56, 174–183.
This opportunity allows highly motivated students interested in orthopedics to be integrated into our academic orthopedics department for a year. You will be in constant conversation with faculty, residents, and department researchers as you learn the basics of research design, methodology, data analysis, and how to navigate the process from IRB application to manuscript submission. In addition to research, there are weekly opportunities for clinical exposure including surgery, clinic and department conferences. There are 3 tracks available: Basic Sciences, Pediatric Orthopedics, centered at the Children’s Hospital of New Orleans, and Adult Orthopedics, centered on the LSU medical school campus (however, all fellows will spend some time at each location).
A commitment for 1 academic year (fall to summer).
Develop and complete at least 2-3 independent research projects
Facilitate ongoing student/resident research projects where necessary.
Manage the content of research websites
Transporting research material, for example from operating theater to laboratories
Personal transportation required
Present your progress at monthly department research meetings
Attend weekly clinics and/or surgeries with various faculty members
Participate in the LSU Ortho student research committee
Participate in health disparities research (a department priority), including tissue bank projects, proposals, and grant submissions
Attend all department didactic/teaching sessions
Assist in developing/maintaining databases for surgical research
Effectively communicate the status of each project and progress with research team members
Select 1 of the 3 tracks (basic sciences, clinical adults/trauma, clinical pediatrics)
Full-time position, approximately $1150/month stipend
For more information please contact Dr. Vinod Dasa (This email address is being protected from spambots. You need JavaScript enabled to view it.) with regard to the orthopedic direction of adult and basic sciences or Dr. Carter Clement (This email address is being protected from spambots. You need JavaScript enabled to view it.) regarding pediatric orthopedics training.
This morning started early after a long day yesterday. The burning sensation disappeared. I’m pretty sure it was something in the bath oil that caused me to have a bad reaction.
I drove to Yosemite (it’s an hour away) via the one-way bridge that cars cross in both directions. I got into the Yosemite gate pretty quickly. I drove another 20 minutes to the meeting spot. I was early so I stopped to take some photos at some take-out points.
I met up with Katherine and we got in her car to go to the next spot. It was Tuolumne Grove to see the gigantic majestic redwood trees. We walk through the forest.
Then we got in the car and drove to Olmsted Point where we walked a bit, took pictures and meditated for a while. There’s a fire in the park, so today the air was smoky.
Then we went to Taneya Lake where we ate a packed lunch she brought. It was nice to sit in her camp chairs and have lunch by a beautiful lake. One interesting fact: the boulders and trees all had rings around them. It was a trail left by the lake this year after the historic snowfall. The water rose so high!
Then we went to Tuolumne Meadow to Soda Springs. It’s a nice walk to see water that is actually naturally carbonated. Scientists can’t figure out why. I also used an outhouse for the first time in a long time.
We then headed back to Olmsted Point because the smoke cleared and I was able to get a better photo.
That was the end of my tour/walk for the day. I drove back to the room to shower and get ready for dinner. Tonight I decided to get take out and eat on my porch.
Now I have to go to bed, because tomorrow is coming soon. It was going to rain, so this walk will be interesting!
By the way, if you’re interested in the dog, she was caught watching football with her boyfriend.









 Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion
Bunions can be a real pain to deal with on your own. The symptoms of a bunion can be very disabling, making it difficult to walk or get from one place to another. The good news is that some treatment options can help you repair your bunion. With the right approach, your bunion problem can be a thing of the past. A lapiplasty is an approach that many people use to treat their bunion problems. Let’s take a closer look at what exactly a lapiplasty is and how it can help you say goodbye to bunion